
Abstract
Outcomes for triple-negative or hormone-refractory metastatic breast cancer (MBC) are poor and treatment options are limited. Described herein are cases of two women who developed MBC following adjuvant chemotherapy and endocrine therapy for human epidermal growth factor receptor 2 (HER2)-negative ductal carcinoma. Both underwent treatment with fulvestrant, followed by paclitaxel and letrozole or nab-paclitaxel. Following disease progression, both patients started single-agent eribulin mesylate (1.4 mg/m2 on Days 1 and 8 of a 21-day cycle). The first patient is currently continuing on eribulin at full dose, despite interruption for hip surgery and the presence of grade 1 neuropathy in the hands and feet. The second patient had a partial response with eribulin, which was sustained for 4 months. She was able to tolerate the full dose of eribulin despite slight worsening of the neuropathy that was present at baseline. Eribulin may be a beneficial option for hormone-refractory MBC with extensive treatment experience.
Introduction
It is estimated that there will be >234,000 new cases and ~41,000 deaths from breast cancer in the United States in 2015, with 6% of women with breast cancer having metastatic disease at the time of diagnosis.1,2 For patients who progress to metastatic disease, the 5-year survival rate is 25%. 1 Data are unclear as to how many women progress to metastatic disease following diagnosis and treatment of a primary tumor. It is estimated, however, that up to 30% of node-negative and 70% of node-positive breast cancers eventually relapse. 3
Once breast cancer metastasizes, the goal of treatment changes from being curative to prolonging the survival of patients and preserving the quality of life.3,4 The approach to treatment for metastatic disease is often driven by the status of important markers such as hormone receptors or human epidermal growth factor receptor 2 (HER2). A recent retrospective study of women with metastatic breast cancer (MBC) found that 33% were HER2-positive and 71% were hormone receptor-positive; 19% of patients in a recent phase III trial were both hormone receptor-negative and HER2-negative, a status often referred to as triple-negative disease.5,6 Patients with HER2-positive and/or hormone receptor-positive disease have improved survival due to recent novel therapy options, whereas survival rates remain poor for patients with triple-negative MBC.5,7 As a result, there is a dire need to find novel treatments to manage patients with MBC, including those with triple-negative disease.
Treatment guidelines recommend endocrine therapy in this setting when possible, due to its lower toxicity profile compared with that for chemotherapy. For hormone receptor-negative patients and hormone-refractory disease, chemotherapy is recommended; however, there is no standard of care. 8 Combination chemotherapy is associated with higher objective response rates and longer time to progression,9–11 while single-agent chemotherapy is associated with lower toxicity and fewer dose reductions.4,10 Given that overall survival (OS) outcomes are equivalent for single-agent and combination chemotherapy regimens, guidelines from both the National Comprehensive Cancer Network 4 and the European Society for Medical Oncology) 3 recommend single-agent treatment in patients without directly life-threatening or severely symptomatic disease.
This article describes two patients with MBC who had hormone-refractory disease and who were candidates for single-agent chemotherapy. In both patients, eribulin mesylate (Halaven®, Eisai Inc), a nontaxane microtubule dynamics inhibitor, was administered.
Case 1
A woman in her 60s was diagnosed with node-positive invasive ductal breast cancer in October 2009. The tumor was hormone receptor-positive and HER2-negative. After a lumpectomy, she received adjuvant docetaxel, doxorubicin, and cyclophosphamide, followed by radiotherapy and adjuvant oral endocrine therapy with anastrozole 1 mg/day. A complete time line of the patient's treatment history is summarized in Figure 1.
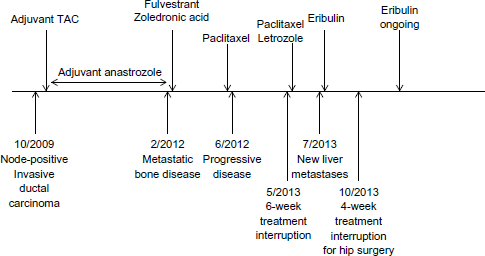
Schematic representation of time line of disease progression and treatments for Case 1.
Recurrent metastatic bone disease was discovered following a fall in 2012, and the patient was treated with fulvestrant and zoledronic acid. Upon disease progression in June 2012, she was started on weekly paclitaxel (80 mg/m2) every 3–4 weeks. This treatment continued for almost 1 year until May 2013, when therapy had to be interrupted so she could undergo surgery to address osteonecrosis of the jaw. Following surgery, paclitaxel was restarted and letrozole added. Treatment continued for 1 month, but she became cachectic and performance status declined to Eastern Cooperative Oncology Group (ECOG) grade 2; cancer antigen 15–3 (CA 15–3) had increased from 60–70 U/mL to 296.3 U/mL. Computed tomography showed that liver metastases with bilobar involvement were now present.
By July 2013, her performance status had declined further to ECOG grade 3, and the patient had alopecia, grade 2 anemia, and grade 1 elevation in serum glutamic–oxaloacetic transaminase (SGOT) and serum glutamic–pyruvic transaminase (SGPT). While still an inpatient, she was started on a trial of eribulin mesylate, dosed at 1.4 mg/m2 intravenously on Days 1 and 8 of a 21-day cycle. Eribulin therapy was chosen due to the good tolerance and efficacy previously seen in frail and elderly patients, minimal toxicities that can be managed with dose modifications, and ease of administration. She was released to rehabilitation, and in September 2013, her performance status, calcium levels, and CA 15–3 were all improving. One month later, the patient fell, again requiring surgery to the left hip and an interruption in eribulin treatment of 4–5 weeks. Following the surgery and palliative radiation, her condition worsened and she started taking hydrocodone and oral morphine for generalized bone pain.
Eribulin was restarted in November 2013 and continues to date. The patient is now independent, with eribulin continuing at full dose, despite National Cancer Institute (NCI) grade 1 neuropathy in the hands and feet. Her performance status has improved to ECOG grade 1. The patient no longer takes morphine and takes hydrocodone only intermittently for occasional hip and back pain. Alopecia and grade 2 anemia continue, her white blood cell count is normal, and there have been no changes in liver function tests. In January 2014, CA 15–3 was 162 U/mL, which further reduced to 101.7 U/mL in April.
Case 2
A woman in her 60s was diagnosed with stage IIB hormone-positive, HER2-negative invasive ductal carcinoma in March 2008. She was treated with dose-dense adjuvant doxorubicin plus cyclophosphamide and weekly paclitaxel, followed by adjuvant endocrine therapy with anastrozole. In February 2010, she presented with recurrent hormone receptor-positive/HER2-negative MBC, with metastases identified in bone and liver. She was started on fulvestrant, but after 6 months, in August 2010, she developed progressive disease in liver and bone, with additional metastatic sites in bone. At this time, the patient was switched to single-agent chemotherapy with nab-paclitaxel, but after a short interval, she again presented with progressive disease in October 2010. Figure 2 summarizes the treatment history for this patient.
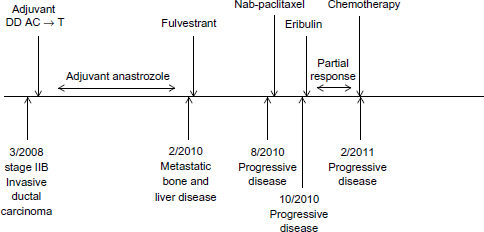
Schematic representation of time line of disease progression and treatments for Case 2.
Following disease progression on nab-paclitaxel, in October 2010, she was switched to single-agent eribulin mesylate, 1.4 mg/m2 intravenously on Days 1 and 8 of a 21-day cycle. The rationale for choosing eribulin therapy for this patient was its favorable tolerability profile and the failure of prior taxane therapy. Although she had some baseline NCI grade 1 neuropathy at the time eribulin therapy was initiated, she tolerated the drug relatively well without any nausea or significant fatigue. There was a mild increase in neuropathy with eribulin, but this did not exceed grade 1 or require dose modification. As shown in Figure 2, she experienced a partial response with eribulin that was sustained until February 2011, when she again developed progressive disease in bone and liver. She subsequently underwent two additional lines of chemotherapy with vinorelbine and capecitabine, but progressed on both and elected to pursue palliative treatment alone.
Discussion
The two patients in the cases described, both with extensive treatment experience in the metastatic setting and few new treatment options, were able to derive clinical benefit from eribulin. Both patients met the entry criteria for Eisai Metastatic Breast Cancer Study Assessing Physician's Choice Versus E3789 (EMBRACE), an open-label, randomized, controlled phase III trial comparing eribulin with treatment of physician's choice (TPC) in patients with locally recurrent or MBC who had received between two and five prior chemotherapy regimens and two or more regimens for locally recurrent or MBC. 6 Patients in EMBRACE had few viable treatment options, with 99% having received prior taxane, 99% prior anthracyclines, and 73% prior capecitabine; 84% had also received at least one prior course of hormonal therapy. 6 Most patients in the trial had metastatic disease, with 84% having metastases in two or more organs. 6 The patients in the cases presented here were therefore typical of the population included in the EMBRACE trial.
Median OS with eribulin was 13.1 months in EMBRACE, significantly longer than 10.6 months for the TPC (hazard ratio [HR] = 0.81; 95% confidence interval [CI]: 0.66, 0.91; P = 0.0 41). 6 This was analyzed with a two-sided stratified logrank test at a significance level of 0.049 and a Cox regression model to calculate the HR. The median duration of response was 4.2 months (95% CI: 3.8, 5.0) for eribulin and 6.7 months (95% CI: 6.7, 7.0) for TPC (P = 0.159). Although not reaching statistical significance, median progression-free survival (PFS) was 3.7 months vs 2.2 months by independent review for eribulin and TPC, respectively (HR = 0.76; 95% CI: 0.71, 1.05; P = 0.137). 6 Based on these data, the patients discussed in these cases appear to have had a generally typical response.
A second phase III study, conducted in less treatment-experienced patients (≤3 prior chemotherapy regimens with ≤2 for advanced disease in this study) showed that eribulin was similar to capecitabine in terms of OS (HR = 0.88; 95% CI: 0.77, 1.00; P = 0.056) and PFS (HR = 1.08; 95% CI: 0.93, 1.25; P = 0.30). 12 In this study, patients who were triple-negative (OS = 14.4 vs 9.4 months; HR = 0.70; 95% CI: 0.55, 0.91; P = 0.01), estrogen receptor-negative (OS = 14.4 vs 10.5 months; HR = 0.78; 95% CI: 0.64, 0.96; P = 0.02), or HER2-negative (OS = 15.9 vs 13.5 months; HR = 0.84; 95% CI: 0.72, 0.98; P = 0.03) also showed improved responses to eribulin compared to capecitabine treatment, respectively. 13 The two patients in the cases reported here were HER2-negative, thus their responses to eribulin are consistent with these results.
Eribulin was well tolerated in both cases discussed here. However, serious adverse events (AEs) were reported in 25% of patients on eribulin and 26% receiving the TPC in EMBRACE. 6 The most common AEs of any grade in both arms were asthenia, or fatigue, and neutropenia. 6 Neutropenia, leukopenia, and peripheral neuropathy were the most common grade 3–4 AEs seen with eribulin, and peripheral neuropathy was the most common AE leading to discontinuation, with 5% of patients stopping treatment. 6 Similar results were seen in the second phase III study, with a similar incidence of overall toxicity and serious AEs for both eribulin and capecitabine. 13
Patients should be monitored closely for signs of peripheral motor and sensory neuropathy. This was of particular importance for the patient in Case 2, because she had grade 1 neuropathy following treatment with nab-paclitaxel at the time eribulin was initiated. The patients in both cases were monitored consistent with guidelines, and grade 1 neuropathy not requiring intervention was noted. In the event that grade 3–4 peripheral neuropathy occurs, eribulin should be withheld until resolution to grade 2 or below. 14
Other AEs of concern are neutropenia and febrile neutropenia. In trials, these were more common in patients with alanine aminotransferase (SGPT) or aspartate aminotransferase (SGOT) ≥3 times the upper limit of normal (ULN) or bilirubin ≥1.5 times the ULN. Consequently, complete blood counts should be monitored prior to each dose, with increased frequency in patients who develop grade 3 or 4 cytopenias. When necessary, neutropenia, peripheral neuropathy, and other serious AEs can be managed by following the recommendations for eribulin dose delay and dose reduction listed in Table 1. 14
Eribulin dose interruption and dose reduction for the management of adverse events. 14

It is important for clinicians to become familiar with additional treatment options for patients with triple-negative or hormone-refractory MBC. It is also essential to recognize potential toxicities that could arise from eribulin therapy and how to manage them. The two cases described here build on the data from the EMBRACE study 6 by confirming the benefit of eribulin therapy in the clinical setting. These cases demonstrate the favorable tolerability profile, efficacy, and ease of administration of eribulin for triple-negative and hormone-refractory MBC. Toxicities are usually mild and can be managed through dose modifications, making this agent ideal for elderly patients who fail previous lines of therapy.
Conclusion
The two cases described here are typical of those in phase III clinical trials of eribulin, as well as in clinical practice, and highlight the role of this new agent. For management of advanced and MBC in pretreated patients, eribulin has been shown to be more effective than the TPC, a choice that equates to the current usual standard of care. Importantly, eribulin has been shown to be effective in those with triple-negative disease, few treatment options, and poor prognosis. The AE profile of eribulin is similar to that of other commonly used agents in this setting, as demonstrated by a similar rate of AEs as with the standard-of-care treatment in clinical trials.6,13 The most serious AEs seen with eribulin, namely, neutropenia and peripheral neuropathy, can be readily managed by following recommendations for dose delays and dose reductions. Eribulin therefore offers a treatment option for patients with advanced and MBC who have few alternatives.
Author Contributions
Conceived and designed the paper: SW, KM. Provided the cases and analyzed the data: SW, KM. Contributed to the writing of the manuscript: SW, KM. Agree with manuscript results and conclusions: SW, KM. Jointly developed the structure and arguments for the paper: SW, KM. Made critical revisions and approved final version: SW, KM. Both authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
The authors thank James Street, a consultant to MedVal Scientific Information Services, LLC, for providing medical writing and editorial assistance. This manuscript was prepared according to the International Society for Medical Publication Professionals’ “Good Publication Practice for Communicating Company-Sponsored Medical Research: The GPP2 Guidelines.”