
Abstract
Nurse practitioners play important roles in breast cancer prevention, early detection, therapeutic efficacy, and surveillance. Assessment of a patient's health status is part of the nine nurse practitioner core competencies updated in 2012 by the National Organization of Nurse Practitioner Faculties. Although adverse events are common in treatment for metastatic breast cancer (MBC), proactive management strategies can limit the number and/or severity of adverse events. Additionally, knowledge of common metastatic sites and clinical signs/symptoms of recurrence provides one of the first-line strategies for successful treatment. We review five case studies of women with MBC who were managed successfully with eribulin mesylate in late lines of therapy after at least two chemotherapeutic regimens for advanced breast cancer that included both an anthracycline and a taxane in either the adjuvant or metastatic setting.
Keywords
Introduction
The probability of a woman developing invasive breast cancer over her lifetime is one in eight. 1 It was estimated that there will be 232,340 new cases of invasive breast cancer in women in the United States in 2013, with almost 40,000 estimated deaths. 2 The five-year survival rate when patients are diagnosed with localized disease is 98%, which drops to 23% when diagnosed with distant metastases. 1
The liver is a common site of distant breast cancer metastases in addition to bone and lung. In a study by Tampellini et al., 3 the liver was the leading site of metastasis for up to 25% of patients with metastatic breast cancer (MBC). An analysis of tumor registry data collected by the University of Texas MD Anderson Cancer Center between 1994 and 1997 from 784 adult patients with confirmed adenocarcinoma revealed that 30% of breast cancers metastasized to the liver. 4
Treatment Options
Determining appropriate treatment requires accurate pathology reports for a full understanding of the extent and biological features of the disease. 5 Patient history, prior breast biopsies, prior irradiation to the chest, pregnancy status, microcalcifications detected through mammography, state of lymph nodes, presence of inflammatory changes or skin abnormalities, and previous treatments all need to be discussed with the pathologist. It is important to orient biopsies appropriately and to request specific biomarker statuses (estrogen receptor, progesterone receptor, human epithelial growth factor receptor 2) during these discussions.
Preferred single agents for recurrent breast cancer or MBC in the 2014 National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology (NCCN Guidelines®) are anthracyclines (doxorubicin and pegylated liposomal doxorubicin), taxanes (paclitaxel), antimetabolites (capecitabine and gemcitabine), and microtubule inhibitors (vinorelbine and eribulin). 5 The choice of therapy is often guided by treatment history of MBC to circumvent resistance. 6
Managing and monitoring therapy
Assessment of a patient's health status is part of the nine nurse practitioner core competencies updated in 2012 by the National Organization of Nurse Practitioner Faculties. 7 Health promotion, health protection, and disease prevention in previously diagnosed and undiagnosed patients may include appropriate screening activities, anticipatory guidance, and recommended environmental and/or lifestyle modifications. 8 Thus, the oncology nurse practitioner (ONP) plays an important role in managing MBC therapy to help minimize complications and maximize therapeutic potential. 8 The ONP may perform physical examinations, assess symptoms, and order laboratory tests to aid in monitoring the patient. 8 Laboratory tests may include a complete blood count (CBC), electrocardiogram, liver function tests (LFTs), a Child-Pugh score, urinalysis, kidney function tests (such as blood urea nitrogen or creatinine clearance [CrCl]), and measures of magnesium and potassium levels.
The optimal frequency for monitoring is based on experience in clinical trials. Recommendations from the prescribing information for the selected chemotherapy should be followed; however, if a sign or symptom associated with disease progression is detected, an immediate reassessment is recommended. 5 The 2014 NCCN Guidelines® for Breast Cancer provides suggested intervals of follow-up when monitoring therapy for metastatic disease (for further information, go to http://www.NCCN.org) 5 ; however, these guidelines should be modified for individual patients based on disease and treatment history.
Case Studies: Eribulin in Practice
Eribulin mesylate is among the preferred single agents currently recommended by the National Comprehensive Cancer Network® (NCCN®), 5 as mentioned above. It is a microtubule inhibitor approved for the treatment of MBC in patients who had previously been treated with at least two chemotherapeutic regimens for advanced breast cancer that included both an anthracycline and a taxane in either the adjuvant or metastatic setting. 9 Eribulin is not the only microtubule inhibitor currently available; however, it has a distinct mechanism of action inhibiting the growth phase versus the shortening phase of microtubule dynamics. 10 The unique interaction between eribulin and tubulin allows for activity against even taxane-resistant cancer. 11 In the phase 3 EMBRACE (Eisai Metastatic Breast Cancer Study Assessing Physician's Choice Versus E7389) trial, eribulin significantly increased overall survival compared with treatment of physician's choice (hazard ratio = 0.81; 95% confidence interval: 0.66–0.99; P = 0.041), with median overall survival of 13.1 and 10.6 months, respectively, and 1-year survival rates of 53.9 and 43.7%, respectively. 12 The most common adverse reactions (incidence ≥25%) were neutropenia, anemia, asthenia fatigue, alopecia, peripheral neuropathy (PN), nausea, and constipation. 9
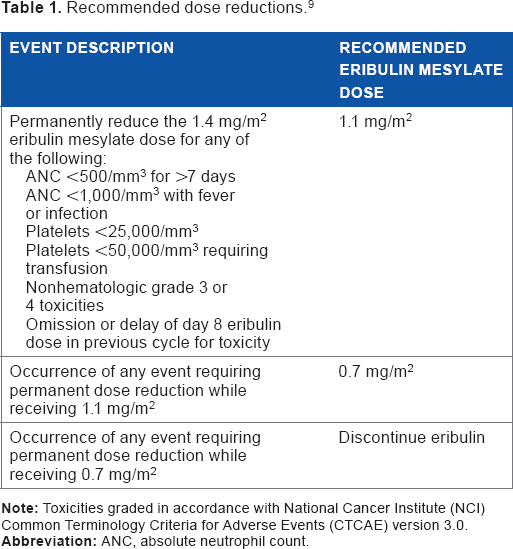
Recommended dosing for eribulin mesylate is 1.4 mg/m2, administered intravenously for more than 2–5 minutes on days 1 and 8 of a 21-day cycle. 9 Initial dose reductions are recommended for patients with hepatic or renal impairment, and the prescribing information provides guidance on appropriate dose-modification (delay or reduction) strategies for patients who experience toxicity (Table 1). 9
Recommended dose reductions. 9
Five cases of women with MBC who received eribulin after at least two chemotherapeutic regimens for advanced breast cancer are discussed below. These cases provide real-life examples from our clinical practices of the practical application of recommendations for managing eribulin treatment, including dose adjustments for patients who experience AEs (specifically, neuropathy, neutropenia, and fatigue) as well for special patient populations (specifically, patients with liver metastases and patients with renal impairment). These examples also illustrate the types of signs, symptoms, or test results that ONPs may observe during patient monitoring and should recognize as signals that treatment adjustments may be necessary. Prompt recognition by ONPs and timely implementation of necessary dose modifications or other changes in therapy may help to improve patient outcomes.
Managing Adverse Events (AEs)
PN
PN is a common AE associated with tubulin inhibitors and the most common toxicity leading to discontinuation of eribulin (5% of patients). 11 PN is often difficult to diagnose because of the variability of symptoms; a thorough neurologic examination is required, along with an extensive patient history. Patients should be monitored closely for signs of peripheral motor and sensory neuropathy, including muscle weakness, painful cramps, fasciculations, muscle loss, bone degeneration; changes in skin, hair, or nails; inability to sweat normally; heat intolerance; loss of bladder control; or fluctuations in blood pressure. 13 In the EMBRACE trial, patients treated with eribulin, who had preexisting neuropathy, were no more likely to develop severe neuropathy than those without preexisting neuropathy. 12 Thus, eribulin can be used in patients with preexisting PN, 9 which is very common in those treated previously with a taxane.
Patient 1 is a woman in her 40s with MBC. She had received multiple chemotherapeutic regimens for MBC, including paclitaxel/bevacizumab, anastrozole/goserelin, paclitaxel, and capecitabine, for more than three years. She had preexisting PN in her fingertips, which was painless and caused no impairment, when starting with 2.5 mg (ie, 1.4 mg/m2) of eribulin mesylate. The cycle 1 day 8 dose was held (because of neutropenia, discussed below), the cycle 2 day 1 dose was decreased (90% of the cycle 1 dose), and the cycle 2 day 8 dose was held (because of neutropenia); there was no significant change in PN during cycle 2. The cycle 3 day 1 eribulin dose was further reduced (90% of the cycle 2 dose, because of neutropenia). At the start of cycle 3, Patient 1 developed increased (grade 2) PN in her fingertips and feet characterized by numbness and tingling; the numbness had decreased at presentation for the cycle 3 day 8 dose. The cycle 4 dose was further reduced (75% of the cycle 2 dose, because of neutropenia). At presentation for the cycle 4 day 1 dose, the PN had moderated in Patient 1's feet; however, by day 8, the numbness had worsened to a degree that impaired her ambulation. Eribulin was discontinued because of toxicity (worsening neuropathy, neutropenia, and thrombocytopenia).
Eribulin mesylate prescribing information recommends withholding eribulin in patients experiencing grade 3 or higher PN until resolution to grade 2 or less. 9 In this case (as in the others described below), eribulin dose reductions were performed in accordance with those recommended by the manufacturer, based on the patient's neutropenia. The patient was able to undergo four cycles of eribulin treatment before her preexisting PN had worsened to the extent that her functioning was impaired.
Neutropenia
Although neutropenia is a common side effect of cytotoxic therapy, treatment-related AEs often can be managed with a proactive approach. 6 A CBC should be performed before each dose of eribulin, and the frequency of monitoring increased if the patient develops grade 3 or higher cytopenias. 9 If febrile neutropenia or grade 4 neutropenia lasts longer than seven days, delay and reduce the dose permanently. The American Society of Clinical Oncology has updated guidelines for prophylaxis in patients at high risk of febrile neutropenia. 14 Although growth factor primary prophylaxis is not recommended, growth factor secondary prophylaxis is recommended for patients in whom a dose reduction may compromise treatment outcome. 14 In the EMBRACE trial, the incidence of neutropenia grade 3 or higher was 57%, and less than 1% of patients treated with eribulin discontinued because of hematologic AEs. 12
Four of the five patients in the cases reviewed here developed neutropenia; all were managed using recommended dose modifications and thus able to continue eribulin treatment.
Patient 1 (therapeutic regimens discussed above) developed neutropenia during cycle 1 of eribulin, causing her to miss the cycle 1 day 8 dose. Neutropenia was treated with filgrastim for three days. Eribulin was resumed at a reduced dose (10% dose reduction because of neutropenia) in cycle 2; again, the day 8 dose was held for ongoing neutropenia and treated with pegfilgrastim. In cycle 3, she had another 10% eribulin dose reduction because of neutropenia, was treated with pegfilgrastim, and experienced thrombocytopenia and mild neutropenia. The cycle 4 eribulin dose was further reduced (25% dose reduction because of neutropenia), and the cycle 4 day 8 dose was held; eribulin was discontinued because of myelosuppression and ongoing PN (as described above).
Patient 2 is a woman in her late 40s with a more than 10-year history of stage IV breast cancer with multiple meta stases and had received multiple prior chemotherapeutic regimens, including doxorubicin/cyclophosphamide, docetaxel, capecitabine, zoledronic acid, bevacizumab, paclitaxel, vinorelbine, metronomic cytoxan, ABT-888, carboplatin, and gemcitabine. She began eribulin mesylate treatment (1.4 mg/m2) and received doses on days 1 and 8 of cycle 1; at day 8, her white blood cell (WBC) count was 3.6 and absolute neutrophil count (ANC) was 1.9. Because Patient 2 had a history of neutropenia associated with prior treatments, a CBC was done on day 15 of cycle 1, which showed a WBC of 1.9 and an ANC of 0.32. Filgrastim was given for three days and subsequently added to her regimen after day 8 of every cycle. After two months, Patient 2 is tolerating the regimen with no additional episodes of neutropenia.
Patient 3 is a woman in her 60s with stage IV breast cancer receiving eribulin. She started on a reduced dose of eribulin mesylate (1.1 mg/m2) because of renal impairment (discussed below). At cycle 1 day 8, she experienced neutropenia (WBC/ANC: 1.3/0.29) and was treated with filgrastim for three days. Her WBC and ANC were increased at cycle 1 day 11 (10.0 and 6.3, respectively), and she received an eribulin mesylate dose of 1.1 mg/m2. Her eribulin mesylate dose was maintained at 1.1 mg/m2 followed by filgrastim for three days after each subsequent treatment, and she completed a total of four treatment cycles. She discontinued eribulin treatment because of disease progression.
Patient 4 is a woman in her 50s having stage IV breast cancer with multiple metastases. She received five years of tamoxifen after treatment with doxorubicin, cyclophosphamide, and paclitaxel for an initial diagnosis of stage II breast cancer. After relapsing, she was treated with multiple chemotherapeutic regimens, including fulvestrant, zoledronic acid, exemestane, capecitabine, gemcitabine, paclitaxel, and ixabepilone. She began using eribulin mesylate at a reduced dose of 1.1 mg/m2 because of abnormal LFT results (discussed below). She experienced neutropenia during cycle 1 (WBC decreased from 5.6 on day 1 to 0.9 on day 8). She also experienced grade 3 mucositis and oral thrush; her day 8 dose was held, and she was treated with filgrastim for neutropenia. Six days later (cycle 2 day 1), she was retreated with a lower dose (0.7 mg/m2); at this visit, her WBC had increased to 27.9, and her mucositis and oral thrush had resolved. She continued to receive filgrastim with every eribulin cycle (two to three times per week after day 1 and day 8 treatments). Beginning at cycle 2 day 8, her eribulin mesylate dose was 1.1 mg/m2; during this time, her WBC ranged from 3.1 to 18.4. At cycle 5 day 1, her WBC/ANC was 7.8/6.6. Her dose was increased to 1.4 mg/m2 because of normalization of liver enzymes (discussed below), improvement in tumor markers, and decreases in ascites and lower extremity edema. The dose was subsequently reduced during cycle 6 to 1.1 mg/m2 because of thrombocytopenia. Eribulin was discontinued in cycle 7 because of disease progression (increased fatigue and liver enzyme abnormalities, as discussed below).
Fatigue
Asthenia/fatigue is a common eribulin-associated AE, with an incidence of 10% (≥grade 3) and 57% (all grades). ONPs can help to encourage patients to remain active, as this is important for patients to circumvent fatigue associated with eribulin.
Patient 4 (discussed above) was experiencing fatigue from a regimen that included ixabepilone and capecitabine when starting eribulin. Her energy level increased while on treatment with eribulin, and she was able to remain very active throughout. However, she began experiencing increased fatigue during later cycles because of her disease and discontinued eribulin after the cycle 7 day 1 dose because of disease progression.
Eribulin Use in Special Populations
Liver Metastases
Patients with MBC liver metastases may experience abdominal discomfort, nausea, anorexia, back pain, or weight loss. 15 Clinical signs that may be present are hepatomegaly, ascites, jaundice, increased alkaline phosphatase, or other abnormal LFT results, such as increases in aspartate transaminase (AST).15,16 Patients with MBC classified as N3 have a greater chance of liver metastases than patients with MBC classified as N1 or N2. 17 In addition to assessing the health status of the patient, the ONP may help guide screening and surveillance activities in patients with MBC. 8 Work-up and surveillance strategies for stage IV disease from the 2014 NCCN Guidelines® for Breast Cancer can be found at http://www.NCCN.org. 5 The eribulin mesylate dose may need to be reduced based on the patient's liver function. A starting dose of 1.1 and 0.7 mg/m2 for patients with mild (Child-Pugh A) or moderate (Child-Pugh B) hepatic impairment, respectively, is recommended. 9
Three of the five patients treated with eribulin also had hepatic metastases.
Patient 5 is a woman in her 40s who was diagnosed with invasive ductal carcinoma of the left breast. She was treated with dose-dense adriamycin—cyclophosphamide followed by paclitaxel. She received radiotherapy after completion of chemotherapy, and then began tamoxifen treatment, with goserelin added approximately one year later. Approximately three years after her initial diagnosis, Patient 5 developed epigastric abdominal pain and dyspnea; a chest film showed right middle lobe atelectasis, and computed tomography (CT) scan of the chest and abdomen showed a number of lung nodules in both lungs, partial collapse of the right middle lobe, and a number of hepatic metastases in the left lobe of the liver. A liver biopsy showed metastatic carcinoma consistent with her primary breast. She then was started on paclitaxel (albumin bound) and denosumab; her paclitaxel dose schedule was reduced approximately three months later because of complications. She was restaged because of a rising CA27.29 level. A CT scan showed improvement in the lung metastases and a decrease in the size of the initial lesions in the left lobe of the liver but many new small metastases in both lobes. She started eribulin mesylate (1.4 mg/m2) and had a significant fall in her CA27.29 level from a peak of 242 before starting eribulin to 34 after seven cycles of eribulin (approximately five months later).
Patient 1 (described above) is a 46-year-old woman with MBC and right upper quadrant (RUQ) pain because of liver metastasis when starting with 2.5 mg (ie, 1.4 mg/m2) of eribulin mesylate. Although the RUQ pain was only partially relieved by narcotics, it diminished after her cycle 1 day 1 dose of eribulin. A CT scan performed before the start of cycle 4 showed stable hepatic metastases. However, a subsequent scan performed after discontinuation of eribulin showed an increase in size and number of hepatic metastases.
Patient 4 (described above) had lesions of unknown origin and at the start of eribulin therapy, presented with massive hepatomegaly with liver edge down to pelvis and across midline, abdominal ascites, lower extremity edema, and dyspnea on exertion from abdominal distention. Her starting dose of eribulin mesylate was 1.1 mg/m2 because of abnormal LFT results (total bilirubin 2.7, alkaline phosphatase 531, AST/alanine transaminase [ALT] 173/112). After the first dose of eribulin, liver function improved (total bilirubin 1.4, alkaline phosphatase 379, AST/ALT 230/66), and by cycle 4, liver size showed noticeable improvement with the liver edge at umbilicus still crossing midline. By cycle 5, LFT results had normalized (total bilirubin 1.0, alkaline phosphatase 188, and AST/ALT 67/50), tumor markers had improved, and ascites and lower extremity edema had decreased. Her eribulin mesylate dose was increased to 1.4 mg/m2. Eribulin therapy was discontinued at cycle 7 (day 8) because of disease progression (indicated by increased fatigue, increased liver enzymes, and increased abdominal distention and lower extremity edema).
In these patients with hepatic metastases, eribulin therapy was associated with improvement in symptoms and tumor markers. In addition, the patient with hepatic dysfunction (ie, abnormal LFTs) was able to receive seven cycles of eribulin treatment using the recommended reduced eribulin dose.
Renal Impairment
Renal excretion of eribulin is minimal,11,18 and patients with decreased renal function can have greater systematic exposure. A starting dose of 1.1 mg/m2, therefore, is recommended for patients with moderate renal impairment (CrCl 30–50 mL/minute). 9
Patient 3 (discussed above) started eribulin for stage IV breast cancer. On day 1, her serum creatinine was 1.37 and calculated CrCl was 46.35 mL/minute; therefore, she received a reduced dose of 1.1 mg/m2. On day 8, her serum creatinine improved to 1.1 with a calculated CrCl of 57.73. Her eribulin mesylate dose was maintained at 1.1 mg/m2 (with filgrastim, as described above) for a total of four cycles. She discontinued eribulin because of disease progression.
This patient case illustrates that appropriate eribulin dose reduction can be used to manage treatment in a patient with moderate renal impairment, without increased toxicity.
Summary
Patients often experience more than one AE during the course of treatment for MBC, and ONPs are instrumental in providing support for the safe and effective use of chemotherapy, especially eribulin. Proper management of AEs and proper dosing in the presence of decreased liver and/or renal function is only one part of successful therapy; ONPs provide key surveillance strategies not only for the prevention but also for the early recognition of AEs, recurrence, or metastatic disease. The longer a patient can stay on therapy, the greater the chance for effective treatment. Proactive management of AEs and appropriate patient education may help to achieve treatment goals.
Author Contributions
DD, LU, UH, SK, and LM contributed to the conception and design of the manuscript, provided content for the manuscript, and made critical revisions. SDJ developed first draft based on content provided by authors. All authors reviewed and approved the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgments
We thank Sherri D. Jones, PharmD, of MedVal Scientific Information Services, LLC, for providing medical writing and editorial assistance. This manuscript was prepared according to the International Society for Medical Publication Professionals’ “Good Publication Practice for Communicating Company-Sponsored Medical Research: The GPP2 Guidelines.”