
Abstract
The incidence of anal cancer is increasing. In the UK, the incidence is estimated at approximately 1.5 per 100,000. Most of this increase is attributed to certain at-risk populations. Persons who are human immunodeficiency virus (HIV)–positive and men who have sex with men (MSM), Organ transplant recipients, women with a history of cervical cancer, human papilloma virus (HPV), or cervical intraepithelial neoplasia (CIN) are known to have a greater risk for anal cancer. This paper will focus on HPV as a risk factor for anal intraepithelial neoplasia (AIN) and discusses the etiology, anatomy, pathogenesis, management of squamous cell carcinoma (SCC) of the anus.
Introduction
The incidence of anal cancer is increasing. In the UK, the incidence is estimated at approximately 1.5 per 100,000.1,2 Most of this increase is attributed to certain at-risk populations. Persons who are human immunodeficiency virus (HIV)–positive and men who have sex with men (MSM) are at increased risk of anal cancer. Organ transplant recipients and women with a history of cervical cancer, human papilloma virus (HPV), or cervical intraepithelial neoplasia (CIN) are also known to have a greater risk for anal cancer.3–5 This paper will focus on HPV as a risk factor for anal intraepithelial neoplasia (AIN) and discusses the etiology, anatomy, pathogenesis, management and preventing its development into squamous cell carcinoma (SCC) of the anus.
Etiology
The most important risk factors for HPV and SCC are behaviors that predispose individuals to HPV infection or immunosuppression. Epidemiological studies have shown that approximately 85% of anal cancers are associated with HPV infection, predominately HPV types 16 (HPV-16) and 18 (HPV-18). HPV-16 and –18 are common in Europe, but in South America and other parts of the world, other HPV sub-types may be more prevalent. AIN, the potential precursor lesion of anal cancer, is common among HIV-positive men who have sexual intercourse with men and is considered analogous to CIN. Recent literature has demonstrated a significant increase in AIN, but the actual overall incidence in the general population is unknown. AIN may be subdivided into low-grade AIN (LGAIN) and high-grade AIN (HGAIN). LGAIN reflects active HPV replication, is not considered precancerous, and includes condyloma and AIN 1. HGAIN comprises AIN 2 and AIN 3; AIN 3 is considered precancerous. 4 Two recent papers reported HPV prevalence of AIN 1 (91.5%) and AIN 2/3 (93.9 %), respectively, among 671 (AIN 1) and 609 (AIN 2/3) patients with AIN.3,6 Anal intercourse is among the presumed mechanisms by which HPV is introduced into the anal canal. Men with HIV are also at increased risk for anal cancer.7,8
Studies have shown that HPV infection of the anal region in both heterosexual men and non–HIV-infected men is also becoming common. Studies have shown that the prevalence of HPV DNA, detected in 222 heterosexual men, was 16.6% for the anal canal and 21.3% for the perianal area. Of the patients with anal HPV infection, fully 33.3% had an oncogenic high-risk HR-HPV type.9,10 In comparing only HIV-negative men (1305 heterosexual versus 176 homosexual), they found anal canal HPV prevalence of 12.2% and 47.2% in these groups, respectively. Two previous studies examining heterosexual men have reported anal HPV DNA prevalence of 8% and 35%, respectively.11,12 With regards to HIV-negative women, anal HPV infection data three studies have reported a prevalence of 27% anal HPV infection and after average follow-up period of 1.3 years, 70% of women developed incident anal HPV infection and abnormal cytology of 66.7% and 42%, respectively, HPV infection having been detected via anal cytology.13,14
Other risk factors include an increasing number of sexual partners, a history of anogenital warts, 8 previous lower genital tract dysplasia or carcinoma, and a history of smoking. 15 In addition to HIV infection, immunosuppression in solid organ transplant 16 and immune disorders have also been shown to be risk factors.
Anatomy
The anatomy of the anal canal is important in understanding SCC of the anus. There are three distinct entities of the anus, namely the rectum, anus, and anal margin. The surgical anal canal (Fig. 1) extends cephalocaudally from the level of the pelvic floor (the anorectal ring or the junction of the puborectalis portion of the levator ani muscle with the external anal sphincter) to the proximal margin of the anal verge. Thus defined, the anal canal corresponds to the segment that is invested by the internal anal sphincter and is about 4.0 cm in length. The dentate (pectinate) line is located approximately two-thirds of the distance proximally from the anal margin. Tumors involving the anorectal junction should be classified as rectal cancers if the epicenter is 2 cm or more proximal to the dentate line (Fig. 2).

The demarcation of the anatomical and surgical canal.
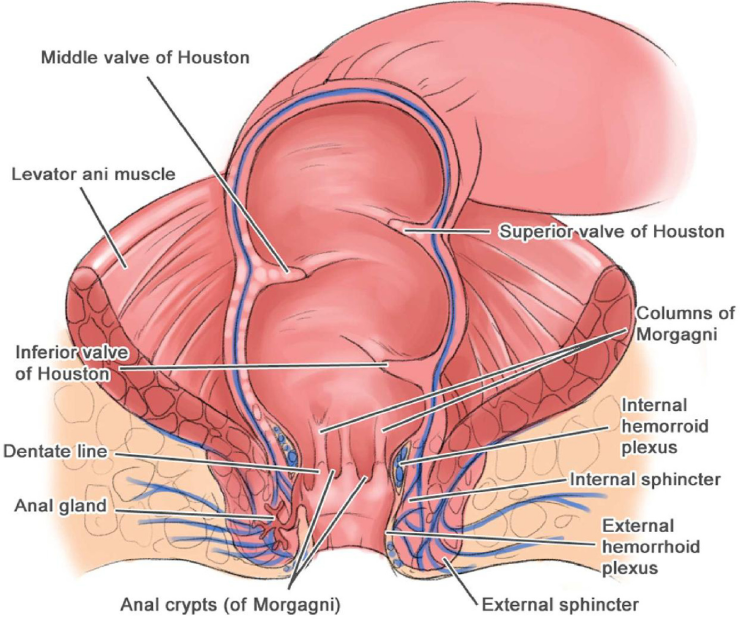
A schematic diagram of the anal canal.
The blood supply comprises branches of the superior rectal artery, the inferior rectal branch of the pudendal artery, and branches of the median sacral artery. The venous drainage is divided into two, whereby above the dentate line, the terminal branches of the superior rectal vein drain into the inferior mesenteric vein and portal system, and below the dentate line, they drain via the inferior rectal vein into the pudendal vein, passing to the internal iliac vein. 17
The lymphatic drainage of the anal canal is dependent primarily on the location of the tumor in relation to the dentate line. In the normal, ie, non-HIV population, squamous cell cancers extending above the dentate line are relatively rare. Hence, SCC of the rectum is not a common entity. Below the dentate line, drainage to the inguinal and femoral nodes occurs, while above the dentate line, there is drainage to the perirectal and paravertebral lymph nodes. Therefore, proximal anal cancers located in the anal canal may drain to the lymph nodes along the inferior mesenteric artery. Meanwhile, distal anal canal and anal margin lesions will metastasize to the inguinal lymph nodes.17,18
Clinical Presentation
Symptoms of AIN are similar to common benign anorectal diseases, and therefore, all patients should be properly assessed to avoid delays in diagnosis. The following signs and symptoms are common in anal cancers:
Bleeding: Bleeding from the anal area occurs in more than half of the patients with anal cancer, and it is usually the first sign of the disease.
Mass: Patients may present with a perianal swelling which may be wart-like or ulcerative.
Pruritis: Itching around the anus is more common in people with AIN than anal cancer. However, pruritis ani can be a symptom of anal cancer.
Pain: About one-third of people with anal cancer feel pain. This may be post-defecation as with an anal fissure or due to invasion into the anoderm and the sphincter complex.
Change in bowel habit: Patients may experience tenesmus or, if there is sphincter involvement, patients may develop incontinence.
Localized inguinal lymphadenopathy: A localized inguinal lymphadenopathy may also be present with symptoms of metastatic disease.3,4,6
Diagnosis
Physical Examination
Upon examination, the anus should be inspected to look for masses, fissures, hemorrhoids, anal warts, or fistulas. A digital examination, a proctoscope, and a flexible or rigid proctosigmoidoscope should help to visualize a carcinoma, although distal lesions can be missed on endoscopy.
Histopathology
The distribution of the histological types of anal cancer is as follows: Squamous cell carcinoma 47%, Transitional (cloacogenic or synonymously known as basaloid) carcinoma 27%, Adenocarcinoma 15%, Carcinoma, NOS 3%, Papillary villous (adeno) carcinoma 3%, Mucinous adenocarcinoma 2%, Melanoma 1%, Other 2%. 17
Squamous cell carcinoma
The World Health Organization classification recommends that the term “squamous carcinoma” can be used to cover all histological types of SCC of the anal canal. However, due to the appearances being variable, a number of variants exist. The common variants observed include small cystic foci lines by mucin-producing cells. Some areas of the tumor can also be pleomorphic.18,19
Basaloid Carcinoma
This tumor may be entirely sub-mucosal and surround the anal canal and lower rectum, or occasionally is seen as a penetrating ulcer at the level of the dentate line. While it arises from cells of the anal transition alone, it is best considered as a variant of SCC for means of treatment and prognosis. It can arise from any of the different epithelial cells of the anal transition zone. Well-differentiated varieties may resemble basal cell carcinomas of skin or transitional cell carcinoma of the bladder. Mixed types also occur, and poorly differentiated ones can be difficult to distinguish from squamous carcinoma. 20
The histology consists of a proliferation of palisading tumor cells. Small foci of necrosis can be present at areas of large cells, and basaloid appearances can also be seen in the same tumour. 21
Staging and prognosis
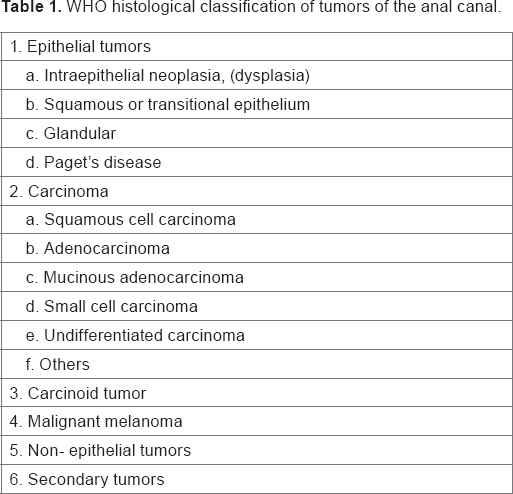
The staging system that is internationally used is the classification by the American Joint Committee on Cancer, 7th edition, 2010 (Table 1). 22 After diagnosis is confirmed, staging investigations should be undertaken, including computed tomography (CT) scan of chest, abdomen, and pelvis for assessment of the primary tumor and for signs of metastastic disease, 22 as well as magnetic resonance imaging (MRI) of the pelvis for more accurate local staging of primary tumor. MRI can show the extent of tumor invasion into the external sphincter and perirectal tissues. MRI is advantageous over CT as it has the ability to differentiate between soft tissues and define structures more clearly. 23
WHO histological classification of tumors of the anal canal.
Positron emission tomography CT is believed to help in determining the nature of any suspicious lymphadenopathy or other possible metastatic lesions. 24
Centers outside the UK also use transrectal or three-dimensional ultrasound for staging and for follow-up, which also gives good anatomical detail, especially for small tumors.25,26
Grading
Anal cell carcinoma is graded histologically based on the degree of differentiation of the tumor, as described in Table 2. 27 If there is any variation within the tumor, the highest grade is recorded as the final grade. 28 However, it is debatable whether the highest grade of histology or the grading is believed to have any significance on prognosis due to the subjectivity and imprecision in grading.
Staging and grading of anal cancers.

Management
There has been a paradigm shift in the treatment of anal cancer over the last 30 years from radical surgery to primary chemoradiotherapy, resulting in reduced permanent colostomy rates. For all four stages of anal SCC except for small T1 tumors of the anal margin, concurrent chemotherapy and radiotherapy are recommended over radiotherapy alone. Otherwise, radical surgery is recommended to improve local control.
Chemoradiotherapy
Radiotherapy is given to the tumor and inguinal nodes. Radiation therapy alone may lead to a 5-year survival rate in excess of 70%. Several retrospective series have previously reported excellent outcomes for patients with T1, N0, and M0 disease with radiation alone.
Following the publication of the results of the national anal cancer ACT II trial, 29 radiotherapy accompanied by administration of mitomycin and 5-fluorouracil (5-FU) and is now regarded as the standard treatment for anal cancer. The most commonly used regimen is described in the ACT II study: 50.4 Gy in 28 fractions in two phases compared with American and European centers, where the prescription dose can range from 54 to 59 Gy in varying schedules.30,31 Mitomycin is a potent DNA crosslinker. A single crosslink per genome has been shown to be effective in killing bacteria. This is achieved by reductive activation followed by two N-alkylation's thus preventing the formation of DNA and leading to cell death. 31 5-FU is a thymidylate synthase inhibitor, which interrupts the action of this enzyme and blocks the synthesis of the pyrimidine thymidine, which is a nucleoside required for DNA replication. 32
There is accumulating retrospective data from recent studies showing the effectiveness of chemotherapy concurrent with intense modulated radiotherapy that have shown actuarial colostomy-free survival with local control rates of 83.7% and 83.9%, as well as a favorable toxicity profile. 33
Early and late chemoradiation toxicities
Complications of chemoradiation therapy for SCC of the anus can be categorized into early and late toxicity. About 60–90% of sphincter preservation preserves quality of life (QOL), although this is not well addressed in the literature. Acute grade 3–4 toxicities occur, mainly consisting of skin reactions, diarrhea, and those that are caused by chemotherapy, ie, nausea, vomiting, mucositis, neutropenia, and infection. Late complications are not insignificant and can greatly impinge upon patient QOL. These symptoms include chronic diarrhea, dysuria, chronic pelvic pain, fractures, and sexual dysfunction. Overall, complications of anal canal occur in 15–13% of patients and include anal ulcers, anal stenosis and necrosis, fistulae, and anal incontinence. 34
Surgery
The indications for surgery are listed below:
Persisting tumor after chemoradiotherapy,
Recurrent tumor after previous radiotherapy, and
Small T1 anal margin tumors without sphincter involvement.
The standard salvage therapy for these former two groups of patients, following chemoradiotherapy, has been abdominoperineal resection (APR). This originally was described by Miles as the resection of the rectum and anus including the sphincter complex. It involves the five abdominal mobilizations of the rectum before the dissection is completed via a perineal approach. This replicates the “modern” extended extra levator approach, which achieves wider excision and removes more tissue around low rectal tumors, including the ischiorectal fat, resulting in a significant improvement in clear margins. The vagina may need to be excised en bloc when involved, and a plastic surgeon will be required to close large defects in flaps such as the vertical rectus abdominis myocutaneous and the inferior gluteal artery perforator. 35 APR can achieve local control in 50–60% of patients, provided that a curative resection can be obtained. In cases involving inguinal lymph nodes, a radical groin dissection should be considered. The European Society of Medical Oncology suggests that local excision can be considered for small well-differentiated carcinomas of the anal margin; ie, <2 cm in diameter, without any evidence of nodal spread.4,36 Studies have described preoperative mapping before excision; however, this may not prevent recurrence. The API is different from the APR for low rectal cancers and sometimes necessitates en block resection of adjacent organs; ie, sometimes a posterior or total pelvic extenuation is required.
Surgery for T1 lesions remains uncertain primarily because of the inability to achieve ideal characteristics in all patients. Specifically, the relatively high degree of failure in achieving appropriate clear margins is disappointing and may account for a significant number of local failures. However, local excision seems to be a viable option in well-selected patients (ie, those with well-differentiated or moderately well-differentiated T1 cancers involving <40% of the circumference, without lymphovascular invasion), particularly when the only other option is APR.34,36,37
Other local treatments
Local treatments, mainly used for the treatment of premalignant lesions such as AIN and Bowen's disease, have been described for invasive anal cancer for small lesions (<1 cm2) in the perianal or intra-anal regions, including imiquimod 5% cream an immune modulator, which can result in pathological resolution of AIN in HIV-positive MSM on highly active antiretroviral therapy (HAART).38–40 Local application of bichloroacetic or trichloroacetic acid may also be considered, and it is believed to show a response rate of approximately 70%.40,41 Data also suggest that a course of topical 5-FU, photodynamic therapy, 42 and CO2 laser therapy may be effective. 43 However, larger trials need to be conducted in this area to validate their effectiveness.
Lesions that are too large may also undergo high-resolution anoscopy and can be used to visually define areas of involvement for electrocautery ablation.44,45 Limited data are available comparing different treatment modalities in men with high-grade squamous cell intraepithelial neoplasia. There is one randomized trial that studied 156 men who were randomly assigned to imiquimod, topical 5-FU, or electrocautery. All grades of AIN were included; high-grade intraepithelial neoplasia was present in 57% of cases. Patients with perianal AIN included 17% of the study. 45 Among the 148 patients actually treated (modified intent to treat), the complete response rates with imiquimod, 5-FU, and electrocautery were 24%, 17%, and 39%, respectively.
Screening and detection
At present, there are no national guidelines for routine screening for anal cancer. As the risk factors for anal cancers are known, screening patients for AIN using anal swabs and Papanicolaou test at least in high-risk groups may be a potential screening method. Some centers in the US have started screening for AIN in HIV cohorts using anal cytology (EXPLORE study). At present, this is probably only appropriate as part of a trial in high-risk groups in the UK, and further studies are warranted to explore its effectiveness. 37 The pathophysiological characteristics of anal cancer are similar to those of other intraepithelial neoplasms found on the cervix, penis, oral tissue, and vulva.
As for the grading and results of anal pap tests, the Bethesda 2001 system 46 categorizes cervical disease in increasing order of severity. As anal cytologic findings demonstrate similar histologic changes, they are graded the same way:
Negative: negative for intraepithelial lesion or malignancy
AIN: anal intraepithelial neoplasia, as seen in histology
ASCUS: atypical squamous cells of undetermined significance
ASC-H: atypical squamous cells suspicious for HSIL
LSIL: low-grade squamous intraepithelial lesion
HSIL: high-grade squamous intraepithelial lesion
SCC: squamous cell carcinoma
High-resolution anoscopy is a procedure using a high-resolution magnifying instrument called an anoscope to identify abnormal cells. If the Pap test shows abnormal findings, ASCUS, LSIL, or HSIL, the patient should be further evaluated with HRA and biopsy 46
If AIN 1 (LSIL) is found at biopsy, routine follow-up should be performed every 6–12 months.
For patients with AIN 2 or 3 (HSIL), therapy is recommended. Observation with repeated evaluation is an option for patients with AIN 1 (LSIL).
Methods of detection of the HPV on cytology smears and tissue samples include
Nucleic acids hybridization assays, eg, Southern blot;
Signal amplification assays, eg, Hybrid capture 2
Nucleic acids amplification assays, eg, genome sequencing, microarray, and polymerase chain reaction. 47
Prevention
Encouraging good behavioral interventions, such as cigarette smoke and limiting sexual partners, would likely affect HPV transmission. Practicing safer sex, such as by increased condom use, may also be effective in reducing HPV transmission. 48 Male circumcision has also been effective at reducing the risk of transmission of HPV and cervical cancer. 49
There have also been phase II/III trials of therapeutic vaccinations against HPV infection. A fusion vaccine of the HPV-16 protein and the M. bovis protein has been associated with clearance of HPV at 48 weeks. 50 Moreover, the introduction of HPV vaccines has demonstrated the quadrivalent vaccine to be effective in preventing AIN in males. 51 Research into this field continues.
Future
The future remains optimistic for anal cancer management. As metastatic disease is less responsive to combined chemotherapy and radiation treatment, novel techniques have been studied to improve survival. There is currently a debate as to whether mitomycin should replace cisplatin for chemoradiation of anal cancers. The ACT II trial has shown mitomycin and 5-FU to be the gold standard treatment. 51 Targeted therapies utilizing biomarkers have also been studied for their potential to personalize treatment for responses to chemoradiation for patients with anal cancer. These include, for example, targeting of the highly expressed epithelial growth factor receptor (EGFR) receptor by the monoclonal antibody cetuximab (Erbitux), by cisplatin, or by 5-FU, as well as radiation and VEGF in anal carcinoma. These processes employ humanized anti-VEGF monoclonal antibodies, which are already well-established in the treatment of metastatic breast, colorectal, renal, and non–small-cell lung carcinoma. However, their effect on prognosis remains undetermined and are of only limited benefit in colorectal cancer. A recent trial showed anti-EGFR (Cetuximab) combined with chemoradiotherapy to be too toxic to deliver. 52 In terms of treatment stratification, p16INK4a is also strongly associated with relapse in SCC of the anus and suggests targeting the EGFR in poor risk/recurrent anal cancer.52–54 Long-term follow-up of these techniques is warranted.
Conclusion
Incidence of anal cancer is increasing, and the diagnosis and management is still challenging to the modern physician/surgeon, especially as symptoms of anal neoplasia are similar to common benign anorectal diseases. In addition, there may be reluctance by patients to see their doctor regarding anorectal problems, thus leading to a delay in diagnosis or even a misdiagnosis. Obtaining a concomitant history, thorough examination, and appropriately directed management can lead to better outcomes in many patients. Every anal lesion should be examined with care and reviewed at an interval or referred to a specialist with multidisciplinary team input. Establishing a screening program in the UK for detecting AIN for high-risk groups, and subsequently introducing a HPV vaccination program, remains debatable, but should be considered if the incidence of AIN in this population continues to increase.
Author Contributions
Conceived the concept: BG. Analyzed the data: BG. Wrote the first draft of the manuscript: BG, PZ. Made critical revisions: PZ, FK. All authors reviewed and approved of the final manuscript.