
Abstract
Objective
To present a case of spontaneous, bilateral hemotympanum secondary to chemotherapy-induced thrombocytopenia.
Methods
Case report and review of the literature.
Results
Bilateral spontaneous hemotympanum is an exceedingly rare event. We present the first case of nontraumatic bilateral hemotympanum secondary to chemotherapy-induced thrombocytopenia in a patient with acute myelogenous leukemia. The patient presented with a 7-day history of progressive bilateral hearing loss and a platelet count of 10 × 109/L after receiving his first dose of induction chemotherapy. A small, left-sided subdural hematoma was present in this patient though no extra-aural sources of bleeding to explain the bilateral hemotympanum were identified.
Conclusion
Full resolution of symptoms was achieved with conservative management.
Keywords
Introduction
Hemotympanum is typically caused by blunt head trauma, epistaxis, or chronic middle ear effusions. Spontaneous hemotympanum, particularly bilateral, on the other hand, is an extremely rare event. We report a case of spontaneous bilateral hemotympanum in a patient with acute myelogenous leukemia.
Case Report
The patient is a septuagenarian with acute myelogenous leukemia. After receiving induction chemotherapy with Azacitidine or 5-azacytidine the patient was admitted to hospital with progressive weakness and confusion. Tumor lysis syndrome was ruled out based on normal renal functions, absence of hyperurecemia, and other metabolic derangements. While in hospital, the patient developed progressive bilateral hearing loss over the course of 7 days. The hearing loss was accompanied by symptoms of tinnitus, vertigo, and left-sided otalgia.
The physical examination showed that bone conduction was better than air conduction in both ears (negative Rinne test). Otoscopy revealed dark middle ear effusions bilaterally and the cone of light was absent in the left ear. The cranial nerve and the remainder of the head and neck exam were unremarkable.
Laboratory investigations demonstrated pancytopenia with platelets as low as 10 × 109/L (N = 140–450 × 109/L). The patient was anemic with a hemoglobin level of 93 g/L (N = 135–175 g/L). The International Normalized Ratio and Partial Thromboplastin Time were normal. INR was 1.0 (N = 0.8–1.2) and the PTT was 33 seconds (N = 27–39 seconds) using the clot-based detection reagin method.
Microscopy of the ear revealed the presence of bilateral hemotympanum (Fig. 1). The tympanic membranes were intact bilaterally.
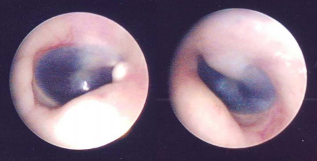
Otoscopic views of right and left tympanic membranes showing bilateral hemotympanum.
Noncontrast computed tomography (CT) scan was obtained prior to the otolaryngology consultation and revealed a small left-sided subdural hematoma. High Resolution CT of temporal bones revealed completely opacified middle ear cavities and mastoid air cells bilaterally (Fig. 2). No other bony abnormalities were seen.
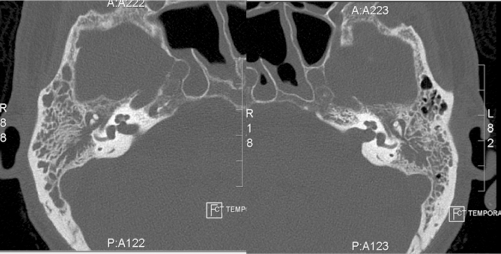
Axial CT scans of the temporal bone of the patient demonstrating bilateral middle ear effusions with no signs of bony erosion.
An audiogram was obtained showing bilateral moderately severe mixed hearing loss (Fig. 3). Tympanometry revealed flat Type B tympanograms bilaterally.
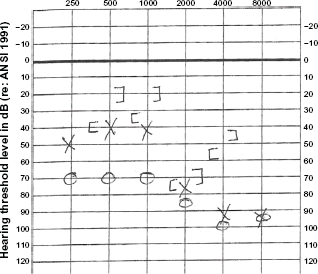
Audiogram of the patient demonstrating bilateral mixed hearing loss.
Treatment of the bilateral hemotympanum in this patient was conservative. Follow-up 2 weeks after the initial consultation revealed normal and mobile tympanic membranes bilaterally with resolution of symptoms. Unfortunately, the patient died due to complications related to acute myelogenous leukemia.
Discussion
Hemotympanum is described as the presence of blood in the middle ear cavity in the setting of an intact tympanic membrane. In hemotympanum, the involved tympanic membrane may appear red or dark blue to near black in color depending on the age of the blood.1–3 The presence of blood in the tympanic cavity can lead to conductive or mixed pattern of hearing loss.4,5 Patients will typically complain of an acute onset decreased ability to hear in the affected ear. They may also complain of aural fullness and, on occasions, otalgia. 6
Traumatic basilar skull fractures are the most commonly reported causes of hemotympanum.1,2 Other known causes of hemotympanum include therapeutic nasal packing, epistaxis, chronic otitis media with effusion, blood dyscrasias, and anticoagulation.1–5 Spontaneous bilateral hemotympanum is a rarely reported event in the literature. Presently, there are only 3 cases in the literature describing spontaneous bilateral hemotympanum–-both involving children with idiopathic thrombocytopenic purpura (ITP). In one report, an abrupt increase in middle ear pressure from coughing or sneezing was hypothesized to be the cause of bilateral hemotympanum in the setting of ITP. 7 Both patients had platelet counts of less than 5 × 109/L.7,8 The third case 3 received anticoagulant therapy and his INR levels were between 3.4 and 4.0.
Eustachian tube dysfunction has been implicated in the formation of spontaneous bilateral hemotympanum in the setting of epistaxis. 4 Therapeutic nasal packing may cause eustachian tube dysfunction by promoting perilymphatic stasis. In addition, a patulous eustachian tube is also thought to play a role by allowing retrograde flow of blood into the eustachian tube during an episode of epistaxis. 4
In this patient, complications that can lead to bleeding, such as tumor lysis syndrome, were not confirmed. Myelodysplastic syndrome was also included in the differential diagnosis based on the presence of anemia (hemoglobin = 98 g/L and red blood cellss = 3.05 [N = 4.3–6.00 1012/L]). However, the absence of neutropenia (neutrophils = 8.4 [N = 1.8–7.5] 109/L), in addition to the absence of abnormal granulocytes were not in support of the diagnosis. Fibrinogen was normal (3.2 g/L), and laboratory normal values ranged between 1.9–4.1 g/L. Therefore, disseminated intravascular coagulation was also excluded.
This is the first report in the literature of spontaneous bilateral hemotympanum secondary to chemotherapy-induced thrombocytopenia. Patients receiving induction chemotherapy for acute leukemia experience prolonged thrombocytopenia due to the cytotoxic effects of therapy. 9 However, the risk of spontaneous bleeding is not always accurately predicted by the degree of thrombocytopenia. Rebulla et al found that patients with platelet counts between 5 × 109/L and 20 × 109/L are at a significantly increased risk of bleeding depending on the presence of certain risk factors. 10 Our patient had a platelet count of 10 × 109/L, a count that is within this range. With no history of trauma, the lack of other sources of bleeding in the head, no ototoxic medications, and spontaneous hematuria, the observed bilateral hemotympanum is most likely due to direct hemorrhage into the middle ear or as a result of severe thrombocytopenia. The presence of a small isolated subdural hematoma in this patient, a rare occurrence in acute bleeding, represents another locus of spontaneous bleeding and lends further support to this hypothesis. 11
The treatment of hemotympanum is predominantly conservative, as its course is self-limit-ing.1–3,5,8 Patients may be prescribed antibiotics prophylactically for a 10- to 14-day course or until the hemotympanum has resolved, which should occur within 1 month of initial presentation.1,3,7 The overall prognosis for conservative management is good. Hearing is restored to normal or acceptable limits after blood in the middle ear cavity has been resorbed.4,8 In patients with conductive hearing loss after head trauma, Grant et al have reported air-bone gaps closing from 23.1 ± 11.0 to 10.0 ± 8.0 decibels on average without any need for procedural interventions. 5
In patients who are unwell with Co morbities and serious diagnoses such as our patient, it is important to reassure patients that their hemotympanum is a self-limiting condition and that their hearing loss will probably resolve conservatively without any need for surgical intervention. Attending physicians armed with the outcomes reported of this condition can very confidently adopt a watchful conservative approach without risk of being accused of being too reluctant to intervene surgically. However, some authors suggest myringotomy and insertion of tympanostomy tubes for hearing loss that persists for greater than 1 month.1,2
Author Contributions
Wrote first draft of manuscript: PW, CX. Principal investigator: AH. Organized the references: PW, CX. Contributed to writing and reviewing manuscript: NG, AH. Made the reviewers' changes: NG. Completed proofreading: AH, NG. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.