
Abstract
Background
Diabetic nephropathy is a progressive disease that leads to renal failure and end stage renal disease. A frequent and early manifestation of diabetic nephropathy is hyaline arteriolosclerosis. The noninvasive method for estimating the severity of arteriolosclerosis is measurement of the renal resistive index (RI). In this study, we determined whether or not normal blood glucose control, classified as an HbA1c < 5.8%, was a sufficiently low level to prevent arteriolosclerosis in patients with essential hypertension.
Methods
The study subjects were 93 patients with essential hypertension with HbA1c levels <5.8%. Patients with a history of medication for diabetes mellitus were excluded. Blood flow velocity of the renal interlobar arteries was assessed by a Doppler ultrasonography and the RI calculated.
Results
RI correlated positively with age, body mass index, pulse pressure, pulse rate and HbA1c, and negatively with diastolic blood pressure. A multivariate analysis identified age, pulse pressure and HbA1c as significant independent determinants of RI. Our data show that RI correlates with HbA1c independent of other variables, even in normoglycemic patients with HbA1c levels <5.8%.
Conclusions
The results of this cross-sectional study suggest that blood glucose levels should be kept as low as possible in order to prevent arteriolosclerosis in the kidney in hypertensive patients.
Introduction
Diabetic nephropathy is a progressive disease that leads to renal failure, with the incidence of end stage renal disease attributable to the disorder having increased dramatically in recent times [1]. In addition to end stage renal disease, patients with diabetic nephropathy also have increased morbidity and mortality as a result of cardiovascular events [2]. Detection of the early changes of diabetic nephropathy has therefore been a subject of great interest, in order that measures can be initiated to prevent progression of the disease. A frequent and early manifestation of diabetic nephropathy is hyaline arteriolosclerosis, characterized by hyaline deposition in arterioles [3]. As arteriolosclerosis in the kidney is a histological change, a renal biopsy is needed for its detection. This procedure is associated with a risk of complications such as renal hemorrhage and therefore as an alternative, measurement of the resistive index (RI) may be used as a noninvasive method for estimating the severity of arteriolosclerosis. The RI is calculated from blood flow velocities in vessels during the cardiac cycle measured by pulsed-wave Doppler ultrasound [4] and has been shown in several studies to be a reliable marker of vascular resistance [5]–[7]. RI measured in renal interlobar arteries has been shown to correlate positively with arteriolosclerosis [8], [9] and there is also evidence that RI correlates with the rate of decline in reciprocal serum creatinine [10]. The index is therefore useful for predicting deterioration in renal function. Patients with diabetic nephropathy have a higher RI compared to other renal diseases [11], [12]. However, previous reports have shown no significant correlation between intrarenal RI and blood glucose control level estimated by HbA1c levels [13], [14]. The reason for this lack of correlation may be attributable to differences in diabetes medications given to the patients in the studies.
Coexistent of hypertension and diabetes mellitus increases the risk for adverse cardiovascular and renal outcomes. In patients with essential hypertension, RI measured at the level of the interlobar arteries is related to the severity and duration of hypertension. In these patients, RI also correlated with age, pulse pressure and intima-media thickness in the common carotid artery [15].
In the present study, we assessed renal RI in hypertensive patients with normal HbA1c levels (<5.8%) and no history of diabetes medication. We found there was a significant relationship between HbA1c level and renal arteriolosclerosis estimated by Doppler ultrasonography.
Methods
Subjects
The study subjects were 93 patients diagnosed with essential hypertension at Ehime University Hospital. Hypertension was defined as a systolic blood pressure (SBP) ≥140 mmHg, and/or a diastolic blood pressure (DBP) ≥90 mmHg, measured three times in the sitting position using a brachial sphygmomanometer, or patients treated with antihypertensive drugs. Exclusion criteria were as follows: current treatment with an angiotensin converting enzyme inhibitor or angiotensin II receptor blocker; a history of treatment with insulin or oral antihyperglycemic agents such as sulfonylureas, metformin or thiazolidinediones; previous myocardial infarction; atrial fibrillation; glomerulonephritis; HbA1c ≥5.8% and serum creatinine concentration ≥1.5 mg/dl. The study was approved by the ethical committee of Ehime University Hospital, and informed consent was obtained from each patient prior to enrollment in the study.
Blood and Urine sampling
Measurement of creatinine (Cr), total cholesterol, HDL-cholesterol and triglyceride concentrations was carried out using an automated analyzer (model TBA-200FR; Toshiba Inc., Tokyo, Japan). Estimated glomerular filtration rate (GFR) was calculated by using a Modification of Diet in Renal Disease (MDRD) study equation with standardized serum creatinine (four-variable equation) [16].
Blood glucose concentration was measured by the glucose oxidase immobilized membrane-hydrogen peroxide electrode peak acceleration method using an automated analyzer (ADAMS-Glucose GA-1170, Arkray, Inc., Kyoto, Japan). HbA1c was analyzed on the ADAMS-A1c HA-8160 (ARKRAY, Inc.,) based on a high performance liquid chromatography assay. Urinary albumin and Cr levels were determined using an automated analyzer (ARCHITECT c8000, Toshiba Inc.,) and the albumin to Cr ratio (uAlb/uCr) calculated to evaluate urinary albumin excretion.
Duplex Doppler ultrasonography
Doppler ultrasonography of the kidney was performed to evaluate renal hemodynamics using an SSD-4000 (Aloka Co., Tokyo, Japan), with a 3.5-MHz convex probe equipped with a Doppler system, as described previously [15]. Renal Doppler flow was obtained from the interlobar arteries at three different positions (superior, mid and inferior) in both kidneys, guided by color flow mapping. We then determined peak systolic velocity (PSV) and end-diastolic velocity (EDV). Mean RI was calculated by the following formula:
RI = (PSV-EDV)/PSV
We have previously analyzed the reproducibility of these parameters in 25 patients with essential hypertension and showed that the coefficient of variation for RI measurements by the same observer on different days was 2.22%.
Statistical analysis
Statistical analysis was carried out using the SPSS 11.0J system designed for Windows (SPSS Japan Inc., Tokyo, Japan). Logarithmic transformation of uAlb/uCr was performed to improve normality. All values in the text and tables are expressed as means (±SD). Univariate analysis was performed to determine the correlation between RI and the following independent variables: age, body mass index, SBP, DBP, pulse pressure, pulse rate, total cholesterol, triglyceride, HDL-cholesterol, glucose, HbA1c, serum Cr, estimated GFR (eGFR) and natural logarithm of uAlb/uCr (ln uAlb/uCr). Multivariate analysis was used to identify determinate factors of RI, using age, body mass index, pulse pressure, pulse rate and HbA1c as the independent variables. A p value <0.05 was considered statistically significant.
Results
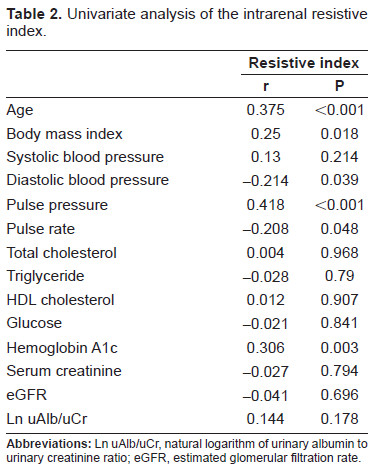
The clinical characteristics of the subjects are shown in Table 1. Table 2 lists the correlation coefficients between RI and the clinical parameters. RI correlated positively with age, body mass index, pulse pressure, pulse rate and HbA1c (Fig. 1), and negatively with DBP. In contrast, there was no correlation between RI and serum Cr, eGFR or ln uAlb/uCr. Multivariate analysis showed that age, pulse pressure and HbA1c were significant independent variables for RI (Table 3). Since beta blockers and diuretics have the possibility to deteriorate glucose tolerance, we also evaluate the correlation between RI and HbA1c in patients who did not have beta blockers or diuretics. Even in these population, there was a significant correlation between RI and HbA1c in univariate (r = 0.323; P = 0.003) and multivariate analysis (β = 0.288; P = 0.005).
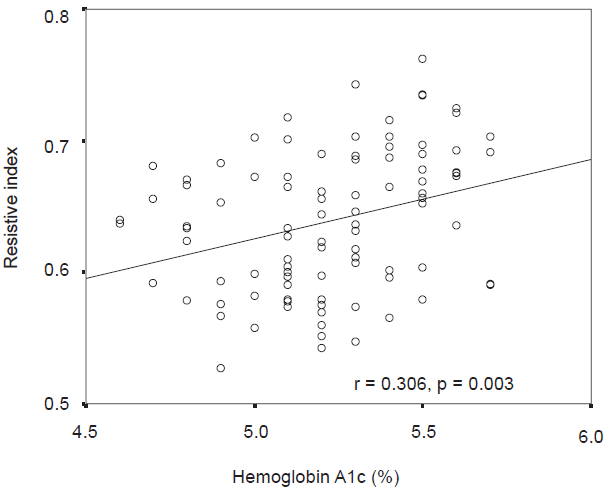
Correlation between intrarenal resistive index and hemoglobin A1c.
Clinical characteristics of the subjects in the study.

Univariate analysis of the intrarenal resistive index.
Multivariate analysis of the intrarenal resistive index.

Discussion
The main objective of the present study was to determine whether RI, a marker of peripheral arterial resistance, was independently associated with age, blood pressure, or normoglycemic levels of HbA1c, defined as values less than 5.8%.
The RI was introduced by Pourcelot in 1974 for the purpose of detecting peripheral vascular disease [17]. An increase in RI is associated with a greater difference in velocity between the systolic and diastolic phases. This difference in flow velocities reflects downstream resistance, which may, at least in part, depend on the degree of peripheral arterial stiffness. Mostbeck et al. measured renal RI and performed renal biopsy in patients with a range of renal parenchymal diseases including glomerulonephritis, interstitial nephritis, glomerular minimal change disease, nephroangiosclerosis due to hemolytic uremic syndrome and malignant hypertension, and acute tubular necrosis. The correlation between RI and histopathological changes was then examined and showed a significant positive correlation existed between RI and glomerular sclerosis, arteriosclerosis and arteriolosclerosis, edema and focal fibrosis [8]. Ikee et al. also analyzed the relationship between renal RI and histopathological changes estimated by renal biopsies and reported that arteriolosclerosis was the only independent risk factor for increased RI in primary glomerular disease [9]. These results suggested that the main determinant of RI in primary renal disease was arteriolosclerosis. In patients with type 2 diabetes with nephropathy or hypertensive patients, renal RI is significantly higher than in normal subjects. In both these patient groups, renal RI was shown to be related closely with intima media thickness in the carotid arteries, suggesting that renal RI values in diabetic and hypertensive patients are strongly affected by the degree of arteriosclerosis. In patients with diabetic nephropathy, renal RI may be more elevated than in other kidney diseases. Matsumoto et al. reported that intrarenal arterial resistance estimated by RI was increased significantly in chronic renal failure patients with type 2 diabetes compared to similar patients without diabetes [11]. Ohta et al. also compared renal RI in patients with either diabetic nephropathy, chronic glomerulonephritis or nephrosclerosis, and demonstrated RI was significantly higher in patients with diabetic nephropathy than in the other two groups, even after adjustment for creatinine clearance values [12]. This finding suggested that factors other than renal function may also contribute to the increase in RI in diabetes. In the present study, multivariate analysis showed that even in patients with normal HbA1c levels there was a significant relationship between intrarenal RI and HbA1c levels. Our data indicate the sclerotic process may progress in hypertensive patients without DM even with small increases in blood glucose levels corresponding to HbA1c levels <5.8%. Pelliccia et al. reported recently that renal RI was elevated in children with diabetes without any evidence of renal dysfunction or microalbuminuria and therefore represented an early change in renal hemodynamics [18]. Early diabetic nephropathy is characterized by glomerular hypertrophy and inappropriate dilatation of afferent arterioles, changes that lead to glomerular hyperfiltration. This hyperfiltration is characterized by a disproportionate decrease in afferent arteriolar resistance, resulting in increased RI. It is therefore possible that hyperfiltration is another mechanism contributing to the relationship seen between HbA1c and RI elevation. In our study, we found uAlb/uCr did not correlate with RI. Although albuminuria is a well-known risk factor for renal disease in patients with DM [19], intrarenal RI is thought to be a more sensitive measurement for evaluating glucose-induced renal damage than urinary albumin excretion in these patients. In order to prevent arteriolosclerosis or hyperfiltration, blood glucose levels should therefore be maintained as low as possible by lifestyle modification or pharmacological intervention.
The kidney has a mechanism for maintaining a relatively constant renal blood flow and glomerular filtration rate, over a wide range of mean arterial pressure levels between 80-160 mm Hg. If this autoregulation is impaired, the kidney becomes sensitive to high blood pressure due to an increase in glomerular capillary pressure [20]. The patients in our study were all hypertensive and there is evidence that arteriolosclerosis due to hypertension is associated with impaired renal autoregulation [21]. In this regard, the correlation we observed between RI and HbA1c suggests that renal autoregulation function may be easily impaired in hypertensive patients with HbA1c levels in the upper limit of the normal range. For that reason, blood pressure in these patients should be strictly controlled in order to protect renal function. While the effects of different antihypertensive drugs on RI were not analyzed in this study, it is well known that blockade of the renin-angiotensin axis in patients with diabetes mellitus has renoprotective effects, independent of changes in blood pressure [22]–[24]. In patients with essential hypertension, we have reported previously that valsartan treatment significantly decreased intrarenal RI during 3 months of follow-up [25]. Leoncini et al. compared a calcium channel blocker (nifedipine) with an ACE inhibitor (lisinopril) in patients with essential hypertension. During 24 months of treatment, despite similar blood pressure reduction, lisinopril was associated with a significant decrease in renal RI, whereas the nifedipine gastrointestinal therapeutic system did not influence RI significantly [26]. In a further study on non-diabetic hypertensive patients with increased RI (>0.68), Caruso reported that 12 months of treatment with either losartan 50mg/day or chlorthalidone 25mg/day caused a normalization of RI in 97.5% of patients treated with losartan compared to only 25.8% in those treated with chlorthalidone, despite there being no difference in blood pressure control with the two agents [27]. These findings indicate that blockade of the renin-angiotensin axis has the potential to decrease RI and improve arteriolosclerosis in hypertensive patients with elevated HbA1c levels in the upper limit of the normal range, as well as in patients with diabetes mellitus. In summary, the results of this cross-sectional study suggest that blood glucose levels should be kept as low as possible in order to prevent arteriolosclerosis in the kidney in hypertensive patients, even in patients with HbA1c levels in the normal range.
Footnotes
None declared.