
Abstract
Some epidemiological evidence shows a link between abnormality of lipid profiles and variations in serum calcium. However, it is unknown whether this association resulted from confounding factors. The present study was designed to investigate the relationship between serum lipids and calcium. Serum calcium was corrected for albumin. Major confounding factors including age, gender, medications, menopause, parathyroid hormone (PTH) and 25-OH-vitamin D status were controlled in analyses. A total of 1907 adult subjects from the province of Newfoundland and Labrador (NL), Canada participated in the study. Significant positive correlations were detected between serum total cholesterol and high density lipoprotein-cholesterol (HDL-c) with variations of serum Ca++ in both genders (p < 0.05–0.0001). Significant positive correlations were additionally detected between triglycerides (TG) and low density lipoprotein-cholesterol (LDL-c) with Ca++ in women only (p < 0.0001) in partial correlation analyses. Similar significant results were detected in both females and males not taking any medication. Analyses were performed based on menopausal status as well. Significant correlations were seen in both pre- and post-menopausal women but higher correlation coefficients were observed in pre-menopausal women as compared to post-menopausal women. Subjects with low calcium levels had the lowest concentration of total cholesterol, TG, HDL-c and LDL-c, while subjects with high calcium levels had the highest concentration of all four markers in women. The significant associations between cholesterol, TG and LDL-c and serum Ca++ remained after calcium was adjusted for 25-OH-vitamin D and PTH. Our results indicate that the abnormality of serum lipid profiles are significantly correlated with altered serum Ca++ levels independent of age, obesity status, medication, phosphorus, magnesium, 25-OH-vitamin D and PTH.
Introduction
An abnormal lipid profile or dyslipidemia is defined by an elevation of plasma cholesterol, LDL-cholesterol (LDL-c) and/or TGs or a low HDL-cholesterol (HDL-c) level. Primary dyslipidemia can be found in several monogenic disorders that lead to different types of dyslipidemias.1–3 In many cases the etiology is polygenic. Primary dylipidemia affect plasma lipoprotein levels by overproduction of lipoproteins and/or decreased clearance.1–3 Secondary dyslipidemia can be caused by many medical conditions which are associated with mild or even severe dyslipidemia even in the absence of an underlying genetic disorder. These conditions include, butarenot limited to, diabetes mellitus (DM), obesity, alcohol overuse, chronic renal insufficiency and/or failure, hypothyroidism, liver diseases, rheumatoid arthritis, pregnancy and the use of drugs such as thiazides, β-blockers, retinoids and sex hormones.4–9 Cholesterol and other lipids can come from the diet as well as from endogenous synthesis. Triglycerides are synthesized from fatty acids or from glucose.
It has been observed that a cluster of diseases and syndromes including hypertension, insulin resistance, type 2 DM and atherosclerosis clinically often coexist or overlap.10–14 Lind et al found that blood pressure and serum glucose and cholesterol concentrations were all positively related to each other in a large adult population. 15 The specific biochemical pathways that are dysregulated in dyslipidemia and the molecular mechanisms that lead to the dysfunction in the general population, except for those caused by clear genetic and secondary conditions, remain unclear. Calcium is a versatile intracellular messenger that is involved throughout the life cycle of an organism to control diverse biological processes. 16 It has been suggested that diabetes and cardiovascular disease are linked by a common defect of divalent cation metabolism, including calcium. 17 Insulin resistance, a state in which increased concentrations of insulin are required to produce a given biological response, has been the focus of attention for a common link between several clinical disorders with dyslipidemia as one group of the clinical manifestation.18–20 Our previous study has shown that altered serum calcium homeostasis is at least partially responsible for insulin resistance in the general population. 21 Data from a Swedish group supported our findings. 22 These data strengthen the theory that calcium might be the central link between dyslipidemia, insulin resistance in hypertension, diabetes and atherosclerosis. Some preliminary association at the population level has been reported in previous studies, including the Framingham Heart Study, 23 where relationships between calcium and general biological markers, 24 and metabolic syndrome 15 were found. However, the general association was not further discussed and left many questions unanswered because of the complicated nature of lipid abnormality and serum calcium variation. Variations of lipids and serum calcium can be potentially influenced by many factors including age, gender, obesity status, medication use, physical activity level and other diseases such as diabetes.4–9
The present study was designed to further investigate the relationship between lipids and serum calcium by controlling for major confounding factors including medications, disease status, menopause, parathyroid hormone (PTH) and 25-OH-vitamin D status in addition to the common confounding factors of age and gender, in a large adult population from the Canadian province of Newfoundland and Labrador (NL).
Research Design and Methods
Research volunteers
A total of 1907 adults were recruited from an ongoing large-scale nutritional genetics study of human complex diseases called the CODING (Complex Diseases in the Newfoundland population: Environment and Genetics) study. 25 The CODING study is being performed in the province of NL, Canada. The volunteers were recruited for the study of genetic and lifestyle factors including genetic variations, nutrition, physical activity, and the interactions of genetics and lifestyle in the development of obesity, diabetes and osteoporosis. This is a study with a cross-sectional design and is being developed into a longitudinal study with the funding support by the Canadian Institute of Health Research (CIHR). Information regarding study design, criteria for participation, and body composition measurements can be found in our previously published papers.21,25,26 Potential participants gave written consent and completed a screening questionnaire to provide general personal information and general lifestyle characteristics. Eligible participants were 19 years of age and older, born in NL in a family who lived in NL for at least three generations, and healthy without serious metabolic, cardiovascular or endocrine diseases. Body mass index (BMI) was calculated as body weight (kg) divided by height (m) squared. Subjects who self-reported having DM or who had fasting glucose levels ≥7.0 mmol/L were designated as having DM. The study received ethics approval from the Human Investigations Committee of the Faculty of Medicine at Memorial University of Newfoundland.
Biochemical measurements
Blood samples were obtained from all subjects after they had fasted for 12 h. Serum concentrations of total calcium, phosphorus, magnesium, triglycerides, total cholesterol, and HDL-c were measured. Additionally, glucose and albumin were measured using Synchron reagents performed on an LX20 clinical chemistry analyzer (Beckman Coulter, Fullerton, CA). Serum total calcium concentration was corrected by serum albumin [calcium + 0.1 × (40–-albumin)/6]. 21 LDL-c was calculated by using the following formula: cholesterol–-HDL-c–-(triglycerides/2.2). The LDL-c calculation is reliable in the absence of severe hyperlipidemia. Serum parathyroid hormone (PTH) and insulin were measured on an Immulite immunoassay analyzer using the IMMULITE 1000 Intact PTH kit (Diagnostic Products Corporation, Los Angeles, CA). 25-OH-vitamin D was measured using a 25-Hydroxyvitamin D 125 I RIA Kit (DiaSorin, Stillwater, MN). Homeostasis model assessment was used to estimate insulin resistance and β-cell function. 27
Measurement of body composition
Total body fat [percentage body fat (%BF)] and trunk fat percentage were measured by using dual-energy X-ray absorptiometry (Lunar Prodigy; GE Medical Systems, Madison, WI). Measurements were performed on subjects after the removal of all metal accessories and while the subjects were in a supine position, as previously described. 28 ENCORE 2002 software version 6.70 was used for analysis.
Statistical analysis
Data are presented as means ± SD. The analyses consist of the following parts. First, partial correlation analyses were performed between the levels of serum calcium and the levels of total cholesterol, TG, HDL-c and LDL-c within sex after controlling for the confounding variables. Second, partial correlations were repeated according to medication use and menopausal status (pre- and post-menopausal women), i.e. within group with or without medication use, and within group of pre- or post-menopausal women. Third, in one-way ANOVA analyses, adjustments for the effects of covariates on serum calcium, cholesterol, TG, HDL-c and LDL-c were carried out using a linear regression procedure. The covariates for serum calcium and lipids were age, phosphorus, and magnesium; percent trunk fat was also included as a covariate in the analyses for serum lipids. The results from one-way ANOVA were corrected by the TUKEY method. Fourth, to account for the influences of vitamin D and PTH, subjects from the “medication-free” group were ranked according to serum calcium concentration; 100 women (top 50 and bottom 50) were selected, and the serum concentrations of 25-OH vitamin D and PTH were measured. Total serum calcium levels were adjusted for the concentrations of 25-OH vitamin D and PTH using a linear regression model before analysis. The levels of total cholesterol, TG, HDL-c and LDL-c were then compared between the low and high calcium groups using a student t test. All analyses were performed using the SPSS software for Windows, version 15.0.
Confounding factors
In addition to serum calcium, evidences from both human and animal experiments show that magnesium may exert influence on lipid metabolism.29–32 The use of medications is probably the biggest factor that modifies the lipids either primarily by treating dyslipidemia or secondarily through other medical processes such as hormone replacement therapy in women. Obesity status is the most prominent risk factor contributing to metabolic syndrome and lipid abnormalities, especially central obesity.4,33 Trunk fat percentage was found to be more significantly associated with lipids in our primary analysis using Pearson correlation than total body fat percentage. Therefore, we chose trunk fat percentage as the covariate representing body composition.
Results
The physical characteristics and biochemical measurements of the adult population studied are shown in Table 1. There are significant differences in all physical characteristics and biochemical markers except for total serum calcium concentration corrected for serum albumin (serum Ca++-C), Mg++ and LDL-c, in the comparison between women and men.
Physical characteristics and biochemical measurements of subjects.

Data are means ± SD;
p value < 0.05–0.001 for all variables, except for serum Ca++-C, Mg++ and LDL-cholesterol, in the comparison between women and men using Student's t-test;
Calcium-C means total serum calcium corrected by albumin (Ca + 0.1 × (40-albumin)/6).
The results of the partial correlations between serum Ca++-C and lipid markers based on gender are shown in Table 2. Significant positive correlations of serum total cholesterol, TG, HDL-c and LDL-c with serum Ca++-C were found in women (r = 0.26, r = 0.16, r = 0.11 and r = 0.19, respectively; p < 0.0001 for all variables). Significant correlations between serum Ca++-C and serum total cholesterol, HDL-c and LDL-c were also observed for men (r = 0.13, r = 0.12 and r = 0.10, respectively; p = 0.05 to 0.009).
Partial correlations between serum Ca++-C concentration and lipids.

Confounding factors including age, trunk fat percentage, phosphorus and magnesium were correspondingly controlled in analyses where applicable.
Women and men not taking any medication were analyzed using partial correlation, controlling for age, trunk fat, phosphorus and magnesium (Table 3). The significant positive correlations remained between serum Ca++-C and lipids in women, but the significant HDL-c correlation was lost in men.
Partial correlations between serum Ca++-C concentration and lipids in subjects without taking any medication.

Confounding factors including age, trunk fat percentage, phosphorus and magnesium were correspondingly controlled in analyses where applicable.
Women were further categorized into pre- and post-menopausal groups for analyses in Table 4. The significant positive correlations between serum Ca++-C and all four lipid markers remained in both pre- and post-menopausal women groups.
Partial correlations between serum Ca++-C concentration and lipids in pre- and post-menopausal women.

Confounding factors including age, trunk fat percentage, phosphorus and magnesium were correspondingly controlled in analyses where applicable.
Table 5 shows the results of levels of serum lipids in female and male subjects according to the concentrations of serum Ca++-C. In women, those in the low serum Ca++-C group had the lowest fasting total cholesterol, HDL-c and LDL-c levels, those in the medium serum Ca++-C group had an intermediate total cholesterol, HDL-c and LDL-c levels, and those in the high calcium group had the highest total cholesterol, TG, HDL-c and LDL-c levels, (P < 0.0001 for all four variables). The only significant difference between calcium groups found in men was with HDL-c.
Levels of serum cholesterol, TG, HDL-c and LDL-c among low, medium and high serum Ca++-C groups.
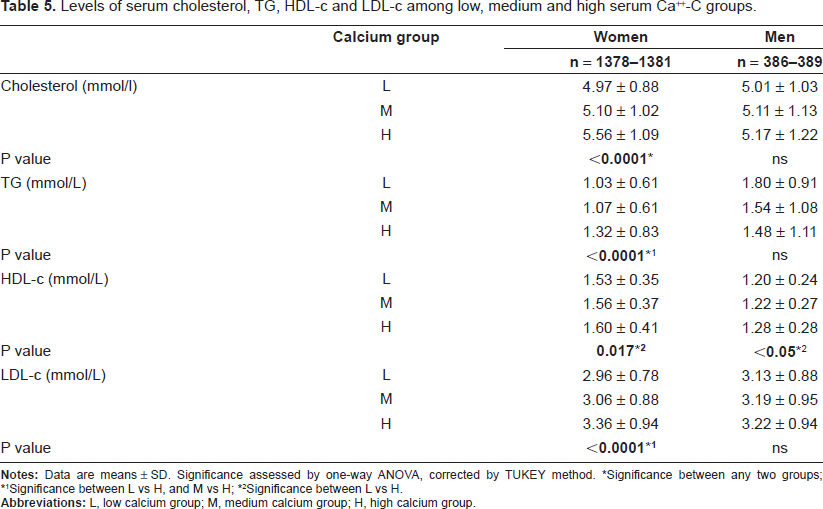
Significance between any two groups;
Significance between L vs H, and M vs H;
Significance between L vs H.
Moreover, the effects of 25-OH vitamin D and PTH were adjusted in a selected group of 100 women (Table 6). Subjects with low serum Ca++-C concentrations had a significantly lower level of fasting total cholesterol, TG and LDL-c compared with subjects with high calcium concentration (P < 0.0001, = 0.015 and = 0.004, respectively).
Comparisons of lipids between low and high calcium groups adjusted for 25-OH vitamin D and PTH.

Student t-test. Values are shown in mean ± SE of raw values. Before analysis, total serum calcium was adjusted for 25-OH vitamin D and PTH, serum cholesterol, TG, HDL-c and LDL-c for age and %trunk fat using linear regression analysis.
Discussion
The regulation of serum calcium and the metabolism of lipids involve many hormonal and physiological factors. Factors such as age, gender, physical activity level, and body composition are contributors to the variations of major lipids in the general population.34,35 Consequently, when attempting to reveal true associations between total serum calcium and any variable of lipids, it is critical to exclude or control as many confounding factors as possible. Age is usually a constant non-modifiable risk factor for dyslipidemia.36,37 Total serum cholesterol, LDL-c and TG levels increase with age, while HDL-c levels decrease with age. 37 In the present study, age was controlled in all analytical processes.
Gender is a constant factor that affects most physiological and pathophysiological conditions. 38 For example, liver is an important organ for lipid metabolism and significant sex differences in hepatic gene expression were seen in mice. 39 These differences contribute to sex differences in physiology, homeostasis, and steroid and foreign compound metabolism. Sex-related differences in gene expression are common across organisms including humans.40,41 Although most findings in our present study show similar results between men and women, sex difference in the relationship between serum calcium and TG are evident. The positive associations were strong in women in every aspect of the analyses. However, the relatively weak associations in men might be due in part to the small sample size compared with women.
During menopause there are physiological changes that occur and the metabolism in pre- and post menopausal women can be very different. This difference can be partly due to the significant change in female hormone levels and the increase of body fat. It is usually seen that menopause is associated with potentially adverse changes in lipids and lipoproteins. 42 In this present study we found that the positive associations between serum Ca++ and abnormalities of lipids were stronger in pre- than in post- menopausal women.
The association between some lipids and serum calcium in humans was reported in a number of cross-sectional and longitudinal studies.15,24 These results were documented as part of a wide range of epidemiological studies targeting general risk factors. De Bacquer and colleagues was the first group to specifically design a study to investigate the link of serum calcium with total cholesterol and HDL-c. 43 Although age, sex and BMI were considered in the analyses, other potent confounding factors, with potentially important roles in influencing either serum calcium or lipid profiles including medication use, smoking, magnesium, percent body fat and menopausal status in women, were not studied.
There is a close association between dyslipidemia and obesity, especially central obesity. 44 Central obesity is a major factor for dyslipidemia.38,45,46 Proper control and exclusion of the factors which influence obesity status would be critical to identifying the association between the two variables that we are interested in. A very recent study showed that dual-energy x-ray absorptiometry (DXA) derived abdominal-fat mass was the best predictor of blood lipid profiles. 47
The central fat percentage measured by DXA was controlled in all analyses in our study. Control of this variable strengthened our findings, leading to the conclusion that the associations of calcium status with lipids are independent of the influences of age, gender, menopausal status and body fat.
Sedentary life style in western countries is a risk factor for dyslipidemia.46,48 Physical activity is therefore a potent factor affecting circulating levels of lipids. The physical activity levels were taken into consideration in our data analyses as well.
Importantly, the significant associations between serum calcium and lipids largely hold even after the control of physical activity levels.
The use of various medications including multivitamin supplements was found in nearly 50% of the study participants. This is typical of adult subjects, including the young, middle aged, and elderly, recruited from the general population. Due to the diversity and different mixes of medications used it is difficult to classify subjects based on the types of pharmaceutical effect. Medication can affect serum lipids through many mechanisms. Endogenous synthesis of cholesterol in the liver is controlled through modification of microsomal enzyme 3-hydroxy-3-methylglutaryl- CoA (HMG-CoA) reductase activity, the rate limiting step. Medications targeting HMG-CoA reductase such as statins can effectively lower cholesterol levels and is widely used in patients with dyslipidemia. 49 Other medications including fibric acids and nicotinic acid also have powerful lipid lowering effects and are widely used in patients with metabolic syndrome and type 2 DM. 50 Other drugs that are not primarily targeting lipids may change lipids as well. Moreover oral contraceptives are commonly used in women of reproductive age. Oral contraceptives can cause hypertriglyceridemia in some women. 51 It is essential to exclude both the primary and the secondary influence of all types of medication on the variation of serum lipids. Analyses according to medication status were therefore performed. Equally significant associations were observed in non-medication users although the number of subjects was reduced by about half compared to the total group. This may indicate that the positive association between serum calcium and lipid profile becomes clearer when not confounded by the influence of medications.
Serum calcium levels are regulated by the action of PTH. PTH acts to increase the concentration of calcium in the blood. 52 PTH regulates serum calcium levels through its effects on bone, kidney and intestines. Moreover, PTH increases the activity of 1-α-hydroxylase enzyme, which converts 25-hydroxycholecalciferol to 1, 25-dihydroxycholecalciferol, the active form of vitamin D. Vitamin D regulates serum calcium levels by promoting calcium absorption from food in the intestines. Blood calcium status is also augmented by re-absorption of calcium in the kidneys as well. PTH and vitamin D are the two hormones primarily involved in the regulation of serum calcium. The potential influence of these two hormones on the associations between serum calcium and lipids were excluded in the present study. Moreover the interactions between serum calcium, magnesium and phosphorus may potentially modify the concentration of these cations. Hence the influence of magnesium and phosphorus was controlled in analyses in the present study. The positive correlation was simultaneously observed between Ca++ and good and bad cholesterols: LDL-c, TG and HDL-c. It seems confusing if we hypothesize that raised level of serum Ca++ is the molecular basis of high LDL-c and TG. Because this is an observational study, the nature of the study does not allow us to address this ‘contradictory result’. This seemingly contradictive positive correlation with Ca++ could potentially be caused by numerous reasons. One of the explanations might be that our body tries to offset the rising LDL-c and TG by increasing the good cholesterol, HDL-c, simultaneously. Obviously this issue warrants further study in the future. To our knowledge, this is the first study designed to investigate the relationship between the variations of lipids and serum calcium in a large population with a comprehensive control of major confounding factors. Owing to the nature of association studies, positive associations like that described in the present study, can not establish a causeeffect relationship. However, the carefully controlled study design and the strong association revealed in the analyses provide strong support for the need for downstream studies to examine if there is a molecular basis for the association between abnormalities of serum lipids and calcium variation.
In summary, the current study analyzed the relationship between the abnormalities of serum lipids and serum calcium. A positive association was found between serum Ca++-C and total cholesterol, TG, HDL-c and LDL-c in women from the general Newfoundland population. A similar trend was found in men. Demonstrating a relationship between calcium and serum lipids in spite of comprehensive control of major confounding factors makes this study unique and further strengthens the possibility of a direct relationship.
Disclosure
The authors report no conflicts of interest.