
Abstract
Atrioventricular nodal re-entry tachycardia is a common supraventricular arrhythmia. The rate of recurrence is relatively high, and accordingly ablative therapy became the first-line suggested therapy. In this review, we highlight the electrocardiographic clues to the diagnosis of atrioventricular nodal re-entry tachycardia, also we present the electrophysiological data and maneuvers that enable the ruling out of other supraventricular tachycardias and ensure an accurate and specific diagnosis of atrioventricular nodal reentrant tachycardia.
Background
The current concept of atrioventricular nodal re-entrant tachycardia (AVNRT) implies an arrhythmia that involves a highly complex atrioventricular junctional area.1,2 Accordingly, it is essential for electrophysiologists to be aware of this complex anatomic and electrophysiologic entity to ensure an optimal approach to its treatment. AVNRT is the most common form of sustained regular narrow complex tachycardia. It is caused by the presence of a dual atrioventricular nodal anatomy and physiology, with a fast and a slow pathway forming a substrate for re-entry. The fast pathway has a higher conduction velocity and a longer refractory period than the slow pathway. 3 The typical and most common form of AVNRT known as “slow-fast” occurs when the antegrade limb of the re-entrant circuit utilizes the slow pathway and the retrograde limb utilizes the fast pathway. Other less common forms are the “fast-slow” (antegrade fast, retrograde slow) and the “slow-slow” variants, and two or more of these variants can coexist in the same patient.
The presence and function of a slow pathway in subjects who never experience an episode of AVNRT is debated, although the slow pathway in normal subjects probably has a role in maintaining conduction in circumstances of autonomic imbalance with extreme hypervagal tone. 4
Clinical manifestations of AVNRT consist mainly of palpitations, although syncope due to poor ventricular filling and reduced cerebral circulation may occur in patients with a rapid ventricular rate and/or prolonged tachycardia. 1 Acute termination of tachycardia can be achieved using vagal maneuvers and/or atrioventricular node suppressing agents.
The concept of upper and lower common pathways is not unanimously accepted inAVNRT. There has been considerable evidence against the presence of these common pathways as distinct entities, the anatomic presence and functional relevance of these pathways remain speculative. 5 Left-sided AVNRT is rare, 6 it involves slow potentials located on the septal aspect of the left atrium, and a trans-septal approach is required for ablative therapy.
Electrocardiographic Diagnosis
Electrocardiographic diagnosis of typical AVNRT is suggested by the presence of retrograde P' waves during a supraventricular tachycardia. This is visible as pseudo R' waves in V1 and pseudo S waves in the inferior leads with an RP interval ≤ 90 msec 7 when P waves are visible (Fig. 1). In contrast, QRS alternans and ST segment alterations during supraventricular tachycardia are rather markers of orthodromic reciprocal tachycardia. 7 Moreover, the absence of ST segment depression during supraventricular tachycardia in the left precordial leads (V4–V6) is highly suggestive of AVNRT, 8 and the authors propose inclusion of this criterion in electrocardiographic algorithms for the differential diagnosis of supraventricular tachycardia.

Upper strip in sinus rhythm, lower strip in tachycardia (atrioventricular Nodal re-entrant tachycardia), encircled is the (R′) wave in V1 lead.
Braunschweig et al 9 found that a transesophageal ventriculoatrial interval ≤ 80 msec is highly suggestive of AVNRT. Oh et al 10 found that differences in RP' intervals (dRP′) between V1 and the inferior leads in the slow/slow variant have significant predictive value for AVNRT (versus orthodromic reciprocal tachycardia with a posteroseptal accessory pathway). The same study showed significantly longer RP' intervals in V1 in AVNRT with consequently longer dRP′ [V1-II] (>25 msec), dRP′ [V1-III] (>23 msec) and dRP′ [V1–aVF] (>30 msec). Finally, Di Toro et al 11 showed that the presence of a notch in the aVL lead is a sensitive marker of AVNRT versus other supraventricular tachycardias; the notch consists of a positive deflection at the end of the QRS complex during tachycardia and it is absent during sinus rhythm.
Belhassen et al 12 described the adenosine triphosphate test for noninvasive diagnosis of dual atrioventricular nodal physiology. Adenosine triphosphate is injected at progressive doses of 10-60 mg (in 10 mg increments) during sinus rhythm until electrocardiographic signs of dual atrioventricular nodal physiology occur (50 msec or more increase in the PR interval in two consecutive beats), or occurrence of atrioventricular nodal echo beat. Dual atrioventricular node physiology was encountered using this method in 75% of patients, and disappeared in 96% of patients who underwent slow pathway ablation. Consequently, the authors concluded that adenosine triphosphate test enables noninvasive diagnosis of AVNRT in a high percentage of cases and can be used reliably to assess the result of catheter ablation.
The presence of 2:1 atrioventricular block is a rare finding in AVNRT, and is related more to a fast re-entrant circuit with functional block rather than to impaired underlying conduction in the atrioventricular node or infranodal area, and therefore slow pathway ablation is safe in this group of patients. 13 Moreover, another study 14 showed that rate irregularity during AVNRT is attributable to a short tachycardia cycle length giving rise to Wenckebach block in the lower “common” pathway. 14 A ventriculoatrial block during AVNRT is a rare phenomenon, the mechanisms are Wenckebach His-atrial block and/or 2:1 His-atrial block. 15
Electrophysiologic Approach
The presence of slow pathway (Jackman) potentials in AVNRT is frequently underestimated, so recording of these potentials in Koch's triangle should not be missed or ignored, 16 and can help to guide the ablation procedure (Fig. 2). During a typical AVNRT, there is a short ventriculoatrial interval (<60 msec at the His catheter), due to retrograde atrial activation during tachycardia, classically called “concentric atrial activation” (Fig. 3).
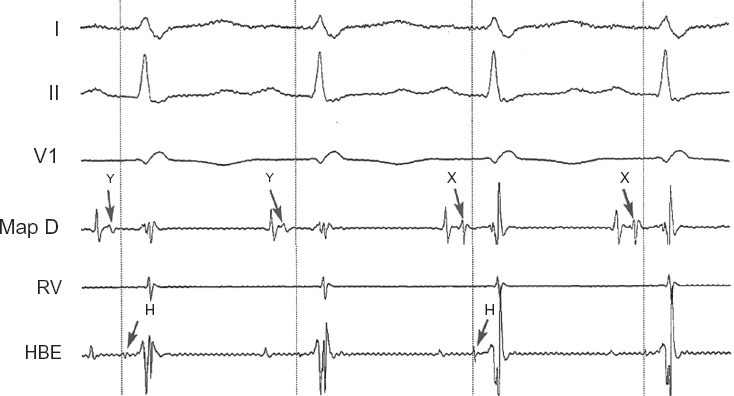
Slow (Jackman) potentials shown in two different sites in the transitional atrioventricular junction region: Y is a proximal site, × is a more distal site (closer to His bundle deflection).
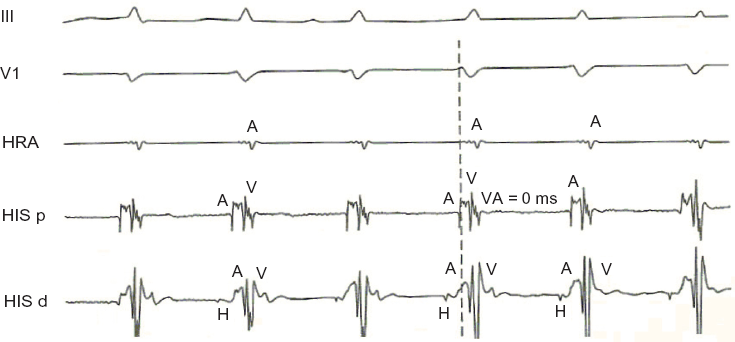
Concentric atrial activation as demonstrated by a ventriculoatrial interval = 0 on the His proximal catheter.
Anatomically, the re-entrant circuit involves the atrioventricular node and the surrounding perinodal tissue with the presence of at least two pathways. Typically, the presence of dual atrioventricular node physiology is demonstrated when a sudden A-H prolongation (≥50 msec) occurs during decremental atrial pacing or shortening of the extrastimulus coupling interval by 10 msec. Electrophysiologically, when a supraventricular tachycardia is present, the main differential diagnosis is orthodromic reciprocal tachycardia and atrial tachycardia.
Atrial tachycardia is the least common etiologic cause of supraventricular tachycardia, and the circuit or focus is located entirely within the atria, with no antegrade or retrograde limb through the atrioventricular node. Therefore, variable atrioventricular and ventriculoatrial intervals are typically observed (Fig. 4) and ventricular overdrive pacing does not result in entrainment. Nevertheless, if it accelerates the atria (overdrive mechanism), a post-pacing A-A-V response pattern is suggestive of atrial tachycardia, and when it fails to accelerate the atria, a diagnosis of atrial tachycardia is most likely. 17
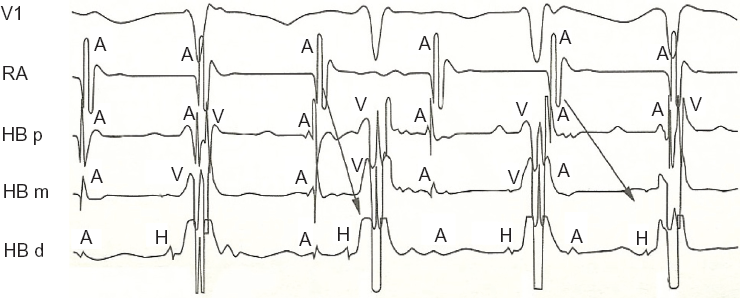
Variable atrioventricular and ventriculoatrial intervals demonstrated with intracardiac recordings of atrial tachycardia.
Focal junctional tachycardia versus AVNRT
A premature atrial complex timed with His refractoriness during tachycardia that leads to a change in the subsequent His timing indicates that antegrade slow pathway conduction is present and functional; AVNRT is also the most probable diagnosis if the premature atrial complex terminates the tachycardia. Conversely, a premature atrial complex that advances the His potential immediately afterwards without terminating the supraventricular tachycardia indicates that a retrograde fast pathway is not a part of the circuit and this favors the diagnosis of junctional focal tachycardia.18,19
Differentiating AVNRT from Orthodromic Reciprocal Tachycardia
Entrainment in Supraventricular Tachycardia
Entrainment is defined as the continual or repeated resetting of a re-entrant tachycardia by a series of consecutive beats of a pacing train. 17 Fusion is likely during entrainment (ie, manifest entrainment) of orthodromic reciprocal tachycardia with right ventricular stimulation if the accessory pathway is septally located, and this phenomenon can help to differentiate orthodromic reciprocal tachycardia from AVNRT 20 (Fig. 5). QRS fusion is absent during entrainment of AVNRT (concealed entrainment) 17 and this is due to collision of an orthodromic wavefront (from paced beat) and an antidromic wavefront (from spontaneous beat) inside the atrioventricular nodal tissue.

Manifest fusion demonstrated in the first two QRS complexes, favoring the diagnosis of orthodromic reciprocal tachycardia.
Differential entrainment using the SA-VA
The SA (sinoatrial) interval is the interval between the ventricular stimulus and the earliest atrial electrogram during entrainment, and the VA (ventriculoatrial) interval is the interval between the RV electrogram (apex and base) and the earliest atrial electrogram during tachycardia; Δ[SA-VA] is measured as [SA-VA] base – [SA-VA]apex. Δ[SA-VA] is positive in AVNRT and negative in orthodromic reciprocal tachycardia with septal accessory pathways. 21
Differential entrainment using cPPI-TCL and VA
c[PPI-TCL] and VA intervals are significantly longer in AVNRT when entrainment is performed at the right ventricular base compared with the apex; these two intervals show no significant difference when there is an orthodromic reciprocal tachycardia; a differential cPPI-TCL > 30 msec and/or a differential VA interval of >20 msec reliably predicts AVNRT. 22 Note that PPI = post pacing interval; TCL = tachycardia cycle length; c [PPI-TCL] = corrected [PPI-TCL] = [(PPI-TCL) – (post AH-pre AH)];[post AH] is the AH interval measured on the return cycle; [pre AH] is the AH recorded during tachycardia prior to pacing.
Entrainment using ΔHA method
The His bundle and atria are activated sequentially during entrainment of AVNRT from the right ventricle and almost simultaneously during typical AVNRT; in contrast, they are activated simultaneously during entrainment of orthodromic reciprocal tachycardia and sequentially during the tachycardia. A ΔHA [HA(entrainment) – HA(tachycardia)] cutoff value of 0 reliably differentiates AVNRT from orthodromic reciprocal tachycardia, having a positive value in AVNRT and a negative value in orthodromic reciprocal tachycardia. 23
Entrainment from right ventricular apex using return cycle method
A cPPI-TCL > 110 msec is a reliable marker of AVNRT 24 (>95 msec in children) 25 whereas a value < 110 msec favors the diagnosis of orthodromic reciprocal tachycardia using a septal accessory pathway without patent pre-excitation.
Para-Hisian pacing
Using a standard quadripolar catheter placed at the His position, this technique consists of pacing at low output for right ventricular capture and at high output for both right ventricular and His capture. Retrograde activation time and pattern are compared during capture and loss of capture of the His bundle while pacing from a para-Hisian position. 26 The SA interval (interval from stimulus to earliest retrograde atrial activation) and VA interval (interval from local ventriculogram to earliest retrograde atrial activation) were compared during His capture and His/right ventricular capture. ΔSA> 40 msec has been found to be specific for AVNRT, 27 also it enables ruling out of a “bystander” accessory pathway that is not necessary operative during the studied tachycardia.
Entrainment applied to the para-Hisian region
SA-VA and PPI-TCL parameters during entrainment from the right ventricle allow distinction between AVNRT and orthodromic reciprocal tachycardia;21,22 this also applies when entrainment is performed from the para-Hisian region, the authors of this study 28 used only two right-sided diagnostic catheters, entrainment was performed with and without His bundle capture (a paced QRS widening of 40 msec or more during entrainment compared with QRS width during tachycardia identified the absence of His-bundle capture). SA-VA and PPI-TCL with and without His capture were compared and accordingly, a SA-VA > 75 msec and a PPI-TCL > 100 msec were found to be specific for AVNRT.
Ventricular Extrastimulation
A premature ventricular complex timed with “His” refractoriness during supraventricular tachycardia that causes a change in subsequent atrial timing indicates that accessory pathway conduction is present and functional, and orthodromic reciprocal tachycardia is the most probable diagnosis 29 (Fig. 6). The VHA (V = local ventricular electrogram, H = “His” and A = atrial electrogram) criterion has been used to differentiate atypical AVNRT (fast/slow) from orthodromic reciprocal tachycardia utilizing a posteroseptal accessory pathway. 30 During ventricular extrastimulation, a “His” bundle potential follows a ventricular potential and is followed by atrial potential when the pathway is via the normal conduction system, whereas a “His” potential may be synchronous or even follow an atrial potential when conduction is via an accessory pathway.

His refractory premature ventricular complex that advances the subsequent atria of 30 msec, demonstrating the presence of a retrograde conducting accessory pathway.
Conclusion
AVNRT is a relatively common supraventricular arrhythmia, and an accurate diagnosis is essential before proceeding with ablative therapy. Along with specific electrocardiographic clues, specific electrophysiological techniques enable accurate diagnosis of AVNRT. Para-Hisian pacing, “His” refractory extrasystole and entrainment techniques are crucial to differentiate AVNRT from other supraventricular tachycardias, especially orthodromic reciprocal tachycardia with a concealed septal accessory pathway.
Author Contributions
Conceived and designed the experiments: AK. Analysed the data: AK. Wrote the first draft of the manuscript: AK, MZ. Contributed to the writing of the manuscript: AK, MZ. Agree with manuscript results and conclusions: AK, MZ. Jointly developed the structure and arguments for the paper: AK, MZ. Made critical revisions and approved final version: AK, MZ. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.