
Abstract
Background
Balloon valvuloplasty was established as an alternative to surgery for treatment of aortic valve stenosis in childhood. Acute complications after balloon dilatation including aortic insufficiency or early death were described.
Aim of Work
To analyze early outcome and midterm results of balloon aortic valvuloplasty (BAV) in Children's Hospital, Mansoura University, Egypt.
Subjects and Methods
Between April 2005–June 2008, all consecutive patients of age <18 years treated for aortic valve stenosis (AVS) with BAV were analyzed retrospectively. The study included 21 patients; 17 males, and 4 females. Their age ranged from the neonatal period to 10 years (mean age 5.6 ± 3.7 years). Patients with gradient ≥50 mmHg and aortic valve insufficiency (AI) up to grade I were included. All patients had isolated aortic valve stenosis except 3 patients (14.3%) had associated aortic coarctation. Six patients (28.6%) had bicuspid aortic valve. All patients had normal myocardial function except one (4.8%) had FS 15%. The duration of follow up was (mean ± SD: 18.5 ± 11.7 months).
Results
Femoral artery approach was used in 20 patients (95.2%) and carotid artery in one neonate (4.8%). Balloon/annulus ratio was 0.83 ± 0.04. Significant reduction in pressure gradient was achieved (mean 66.7 ± 9.8 mmHg to 20.65 ± 2.99 mmHg) (P < 0.001). Nine patients (42.8%) developed grade I AI, 2 patients (9.5%) developed grade II AI and 1 patient (4.8%) developed grade III AI. Two early deaths (9.5%); one died due to heart failure caused by grade IV AI and a neonate died because of severely compromised LV function. One patient (4.8%) had femoral artery occlusion necessitating anticoagulation. Patients remained free from re-intervention during follow up.
Conclusion
Balloon valvuloplasty of aortic valve stenosis significantly reduces gradient with low morbidity and mortality in children.
Introduction
Aortic valve stenosis (AVS) represents 3%-7% of all congenital heart diseases. 1 There is consensus in the management of mild and severe forms of AVS but there is a tendency for balloon aortic valvuloplasty (BAV) except in the presence of dysplastic aortic valve or associated moderate to severe aortic insufficiency. 2 So, BAV has been established as an alternative to surgery for therapy of AVS in childhood3,4 and has proven to be an effective method for decreasing gradient between the left ventricle and the aorta.5,6 BAV in congenital AVS provides palliation that is comparable to that achieved by surgical aortic valvotomy, but without the risks and morbidity of surgery.6,7 Acute complications after BAV leading to early death (<30 days) have been described 8 as well as the development of aortic insufficiency as a long term complication during follow up.9,10 The clinical status, aortic valve morphology, myocardial function at time of intervention and age of the patient are possible risk factors determining the outcome of BAV.11,12
The aim of this study was to analyze the early and intermediate term follow up results of BAV of AVS in childhood and to present our own experience in this issue.
Material and Methods
Patients
All consecutive patients younger than 18 years who underwent BAV for congenital AVS in Children's Hospital, Mansoura University, Egypt were analyzed retrospectively in the period from April 2005 to June 2008 as regarding their demographic, clinical, echocardiographic, hemodynamic and angiographic data. Written informed consent was obtained from all parents of the children included in the study. The Institutional Ethical Review Board of the Children's Hospital had approved the study.
All patients had isolated congenital AVS except 3 patients who had associated discrete juxtaductal aortic coarctation (COA). Patients were subjected to clinical examination including symptoms as dyspnea and signs of congestive heart failure or ductal dependency in neonates. Echocardiography was performed to all patients by expert pediatric cardiologists, using the SONOS-5500 device (Hewlett-Packard, Andover, MA) and an 8-MHz probe, and their data were analyzed as regard aortic valve morphology, left ventricular (LV) function, transvalvular gradient (peak and mean), annulus diameter, grade of aortic insufficiency (AI) (if any) and associated anomalies. Aortic valve morphology was determined from a parasternal short-axis view and classified as tricuspid and bicuspid. A semi-quantitative estimate of severity of AI was made by using color-flow and pulsed-wave Doppler echocardiography. The degree of AI was graded and defined as none, trivial, mild, moderate, or severe (or 0-IV).13–15
Continuous Wave Doppler (CWD) tracing to the aortic valve was done to measure the peak instantaneous gradient through the valve by measuring the maximal systolic velocity from either apical or suprasternal view and calculating a pressure gradient using the modified Bernoulli equation (pressure gradient = 4 × [maximal velocity]2) and time velocity integral of Doppler curve to calculate the mean pressure gradient. Echocardiographic examination was done at time of diagnosis, one day after intervention, and repeatedly during follow up.
Patients with a Doppler peak instantaneous gradient ≥ 50 mmHg, and those with associated mild aortic insufficiency (AI) were included in the study. Patients with moderate to severe AI, associated congenital heart disease need surgical intervention, or those with associated supravalvular stenosis were excluded. The outcome was either successful BAV, failure or reintervention either by further balloon or by surgery and procedure related complications as rhythm disturbances, aortic valve insufficiency by different grades, vascular complications, recurrence during follow up necessitating re-intervention or death.
BAV Technique
BAV was indicated when peak instantaneous pressure gradient across the valve ≥50 mmHg in patients with normal myocardial systolic function (FS ≥ 28%) and with lower peak instantaneous pressure gradient in patients with an impaired myocardial systolic function (FS < 28%). BAV was performed under general anesthesia using Sephoflourane and under biplane fluoroscopic guidance. Heparin was administered during the procedure in a dose of 100 IU/Kg. The catheterization technique was performed through femoral artery access in all patients and retrograde aortic approach to the aortic valve as described by Mullins 16 except one neonate where carotid artery approach was used. Left ventriculography was done and aortic valve annulus was measured during systole in 2 angiographic planes. An open-tip catheter was inserted and the peak-to- peak pressure gradient in the coarctation segment was estimated in the three patients with associated coarctation. The catheter was advanced through the stenotic aortic valve into the left ventricle using soft tip guide-wire and the peak-to- peak pressure gradient across the aortic valve was estimated. Tayshak-II® or mini-Tayshak® (NuMed Canada, Inc.) balloons for valvuloplasty were used and their sizes were selected according to the aortic annulus diameter with balloon annulus ratio ≤1. The appropriate length of the balloon was selected according to the size of the patient. The balloon was advanced over the guide-wire and inflated at the level of valve orifice. In the three patients with associated COA, the balloon was withdrawn and a different-sized balloon was introduced and inflated at the coarctation segment. The size of the balloon was selected according to the narrowest native diameter by balloon/annulus ratio not exceeding 1. Heart rate slowing was achieved by intravenous bolus adenosine with dose 0.3 mg/kg. Intravenous adenosine was injected rapidly, followed by a saline flush; this often resulted in a short period of sinus bradycardia followed by asystole. After dilatation, peak-to-peak pressure gradient was remeasured across the valve (and the coarctation segment in the three patients with associated COA) to evaluate any residual gradient. Aortic root angiography was performed to detect aortic insufficiency.
After BAV, a satisfactory result was defined as a reduction of the peak-to-peak pressure gradient of at least 50% or a residual gradient of less than 25 mmHg. If satisfactory reduction was not achieved, redilatation using larger balloon and using adenosine to repeat procedure by the same previous dose followed by angiography after each change in balloon size to detect aortic valve insufficiency. No further intervention was performed in any case, if a moderate aortic valve insufficiency was detected in the following angiography or reach balloon/annulus ratio 1.
Statistical Methods
Data were expressed as mean ± SD. Student t-test was used to compare variables. Paired t-test was used to compare the same patient before and after BAV. Statistical significance was identified as P < 0.05. Pearson's correlation coefficient was used to assess the relationship between balloon annulus ratio and the degree of aortic insufficiency post intervention. Analysis was done using SpSS soft ware (version 16.0; SpSS, Chicago, IL, USA).
Results
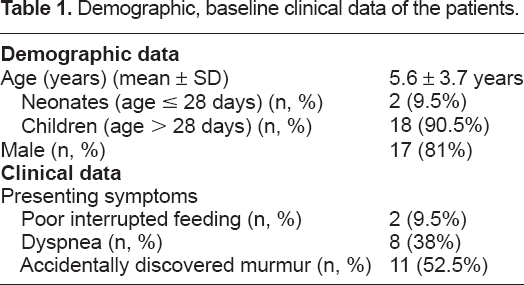
21 patients underwent BAV for congenital aortic valve stenosis, 17 males (81%), 4 females (19%). Demographic data of all patients are summarized in (Table 1). Two patients (9.5%) were presented during neonatal period by poor interrupted feeding, 8 patients (38%) were presented during infancy by dyspnea and 11 patients (52.5%) were presented by accidentally discovered murmur.
Demographic, baseline clinical data of the patients.
Echocardiographic data before intervention were as follows: 15 patients (71.5%) had tricuspid aortic valve, 6 patients (28.5%) had bicuspid aortic valve. Among those with bicuspid aortic valve, 3 patients (14.3%) had associated discrete juxtaductal aortic coarctation. All patients had severe AS; peak instantaneous pressure gradient across the valve was 77.95 ± 5.9 mmHg. Seventeen patients (81%) had no AI, 3 patients (14.3%) had grade I AI and 1 patient (4.8%) had grade II AI. All patients had normal myocardial systolic function (FS > 28%) except one who had affected myocardial systolic function (FS 15%).
We performed balloon angioplasty to the three patients with associated aortic coarctation at the same time of BAV with satisfactory results (Table 2).
Basal echocardiographic data of the patients.

Immediate Outcome
Table 3 shows early follow up results. During catheterization, we found significant reduction in peak-to-peak pressure gradient across the aortic valve after BAV from 66.7 ± 9.8 mmHg to 20.65 ± 2.99 mmHg (P < 0.001) in all patients regardless the aortic valve anatomy. Left ventricular pressure decreased immediately from 145.4 ± 13.8 mmHg to 103.25 ± 3.6 mmHg (P < 0.001). In the 3 patients with associated COA, there were a reduction in peak-peak pressure gradient across COA after balloon angioplasty from 58.6 ± 11.9 mmHg to 14.4 ± 0.54 mmHg (P < 0.001).
Early and intermediate term results.
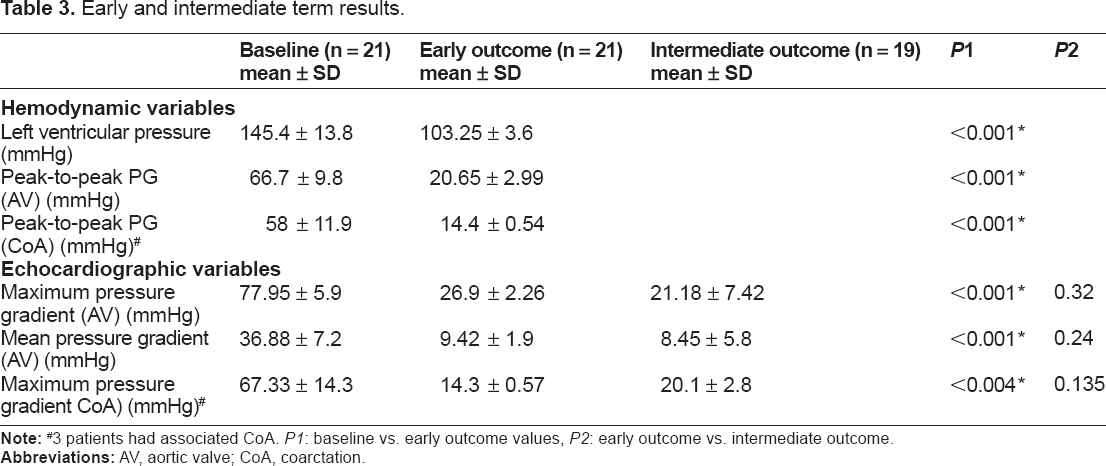
3 patients had associated CoA. P1: baseline vs. early outcome values, P2: early outcome vs. intermediate outcome.
Abbreviations: AV, aortic valve; CoA, coarctation.
Furthermore, we detected significant reduction in maximum pressure gradient across AV [from 77.95 ± 5.9 mmHg to 26.9 ± 2.26 mmHg (P < 0.001)] and COA [from 67.33 ± 14.3 mmHg to 14.3 ± 0.57 mmHg (P < 0.001)] one day after the procedure by CWD echocardiography. We had two deaths; one patient with bicuspid aortic valve was complicated post intervention by severe aortic insufficiency (AI) which was not correctable and died with intractable heart failure about 48 hours after the procedure. The other one was a neonate who had severely compromised LV systolic function (15%) and died in the same day of the procedure.
One patient (4.8%) developed bradycardia during BAV which was reversible at the end of the procedure; another patient (4.8%) developed ventricular fibrillation during the procedure necessitating cardioversion. One patient (4.8%) (with associated aortic coarctation) was complicated immediately after intervention with impalpable femoral artery pulsation due to thrombus necessitating anticoagulation with low molecular weight heparin to resume arterial patency (Table 4).
Procedure details and complications.

Eight patients (38%) did not develop aortic insufficiency (AI), 9 patients (42.8%) had grade I AI, 2 patients (9.5%) had grade II AI, 1 patient (4.8%) had grade III AI and only one patient (4.8%) had grade IV AI and died after the procedure (Table 4). The degree of AI was positively correlated to the balloon/annulus ratio used (r = 0.72, P < 0.001) but not correlated to the valve morphology (r = 0.23, P = 0.133). Comparison between patients with tricuspid aortic valve and those with bicuspid AV as regard the degree of AI after BAV showed no significant difference (P = 0.10). The balloon/annulus ratio used was 0.83 ± 0.04 (range from 0.8 to 1). All patients, except the two deaths and the patient, who required anticoagulation, were discharged home within 24 hours after the procedure.
Intermediate-term results
Nineteen patients were followed up post-intervention. The duration of follow up ranges from 6-38 months (mean ± SD 18.5 ± 11.7 months). The patients were followed up clinically and by echocardiography every three months for recurrence of symptoms, development of AI or increase in its grade, restenosis of the aortic valve and myocardial function. Concerning maximum pressure gradient across the AV measured by CWD echocardiography, we found no statistically significant difference between values of immediate and those of intermediate term results (26.9 ± 2.26 mmHg and 21.18 ± 7.42 mmHg respectively, P = 0.32). Moreover, mean pressure gradient across AV was not differed significantly (9.42 ±1.9 mmHg and 8.45 ± 5.8 mmHg respectively, P = 0.24). With follow up of patients who had CoA, peak instantaneous pressure gradient across the site of CoA showed no significant increase compared to immediate results (14.3 ± 0.57 mmHg and 20.1 ± 2.8 mmHg respectively, P = 0.135) (Table 3). The grade of AI did not increase in all patients during follow up.
Discussion
Intervention for AVS in pediatrics with trans-catheter balloon dilatation and surgical valvotomy have, in the past, been associated with high mortality rates. 8 Risk factors for poor outcome have been attributed to young age at presentation,17,18 small left heart dimensions,8,19 and endocardial fibroelastosis. 20 With improvement of catheterization technology, 21 the survival rates with BAV have improved. 22 The effectiveness of BAV in pressure reduction of the LV has been reported by several authors.23–25
In this study, we found that BAV provided immediate and intermediate-term gradient reduction in children with congenital AVS. We observed that peak-to-peak pressure gradient decreased in all patients regardless the aortic valve morphology. Many previous studies had supported these results.23,26,27
Aortic incompetence (AI) has been previously identified as the main indication for aortic valve surgery after BAV. 28 In our study, AI was absent in 38% of patients, grade I in 42.8%, grade II in 9.5%, grade III in 4.8% and IV in 4.8% of cases. Degree of AI was not related to the valve morphology but showed significant correlation with the balloon/annulus ratio. Reich and coworkers showed that functionally bicuspid aortic valve morphology is an independent risk factor for AI after BAV. 24 However, in our patients, the usage of smaller balloon/annulus ratio could explain the significant low incidence of AI. In agreement with Knirch et al 29 who concluded that aortic valve morphology is not a risk factor for early outcome in BAV in children.
The in-hospital mortality was detected in 2 patients (9.5%). The low mortality and low acute postoperative complications in our study can be explained by small number of neonates, small number of patients with reduced myocardial function before intervention and again, due to low balloon/annulus ratio; known risk factors to increase acute complications. 29
One patient died due to intractable heart failure as a result of severe (grade IV) AI after BAV despite using balloon/annulus ratio <1. The most unpredictable, frustrating and probably, the most common complication of BAV is the creation of significant AI. Significant AI occurs in approximately 10% of all BAV. This number is comparable to its occurrence following surgical aortic valvotomy. It appears that over-sizing of the balloon for aortic valve annulus is one predictor for the creation of AI, however AI is created even when using a precisely measured balloon/annulus ratio <1. The wire and then the balloon passage through a valve leaflet rather than through the commissures/orifice of the valve results in significant AI. 30
The other patient was a neonate who had pre-intervention affected LV myocardial systolic function (FS 15%). He died within 24 hours after the procedure by heart failure. Neonate aortic stenosis is a fatal disease that associated with myocardial dysfunction due to subendocardial ischemia or endocardial fibroelastosis. 31 Myocardial dysfunction is one of the main variables in the prognosis of patients with aortic stenosis in neonate period. Myocardial dysfunction due to abnormal myocardial perfusion disables the LV preventing it from maintaining normal cardiac output. 32
The femoral approach is used routinely in most centers 33 and it was used in most of our patients. One patient (4.8%) was complicated by femoral artery occlusion post-operatively and was managed by low molecular weight heparin infusion with regained arterial patency.
Carotid artery approach was performed in one patient. This approached was considered when there are problems in femoral or umbilical catheterization approach. 34 Many previous studies had demonstrated the use of carotid artery approach to BAV.35,36
Adenosine is a powerful drug that creates arterial hypotension and leads to transient cardiac stand-still after bolus injection. 37 It was used in our patients to slow heart rate and hence stabilize the balloon. Balloon stability during the BAV procedure is crucial for a successful outcome and is likely to reduce complications. RV pacing was not used in our patients as it is used in older age groups and needs an additional venous access. 38
In our study, 3 patients (14.3%) had associated discrete coarctation and underwent balloon angioplasty in the same catheterization setting. Coexistence of AVS and CoA is relatively uncommon, but the exact prevalence is unknown.39–41 With balloon angioplasty, we found a significant reduction in peak-to-peak gradient across the coarcted segment. Balloon angioplasty of native CoA gained more acceptance in children. 42 Tokel and his colleagues 43 studied the sequential balloon dilatation for combined AVS and CoA in children and found results to ours.
None of our patients was complicated by aneurysm at the coarcted segment. On follow up, no recurrence of pressure gradient across CoA segment in these patients. Similar findings were observed by many authors.44,45
Conclusion
Balloon valvuloplasty of aortic valve stenosis significantly reduces gradient with low morbidity and mortality in children.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.