
Abstract
Objective
Examine pulmonary artery systolic pressure (PASP) response to exercise in isolated borderline and mild to moderate pulmonary arterial hypertension (PAH).
Methods
Doppler stress echocardiography was performed in 32 healthy volunteers with resting PASP of 29 mm Hg or less, 39 with resting PASP between 30 and 40 mm Hg, and 7 with resting PASP between 41 and less than 60 mm Hg. All subjects had otherwise normal echocardiograms.
Results
Rate of increase in PASP with exercise was positively associated with resting PASP (P < 0.001), increased age (P < 0.001), and estrogen use among women (P = 0.001). On multivariate analysis, PASP slope was independently related (P = 0.03) to resting PASP and inversely associated with exercise time (P < 0.001).
Conclusions
Patients with borderline and mild to moderate resting PAH have an exaggerated PASP response to exercise. PASP slope is a strong independent predictor of exercise time. Outcome studies are needed to determine the prognostic significance of this finding.
Introduction
Dyspnea on exertion and exercise intolerance are common presenting symptoms among patients with various cardiovascular and pulmonary diseases, including pulmonary arterial hypertension (PAH). As a result, patients presenting with these symptoms frequently undergo selected diagnostic testing, including a comprehensive echocardiographic examination, primarily to assess ventricular and valvular function (1). The current assessment of pulmonary hemodynamics and diastolic filling with Doppler echocardiography is predominantly performed in the resting condition, although patients experience their symptoms during exertion. The functional data that could be provided by examination of the cardiopulmonary response to exercise may clarify the cause of dyspnea and have a substantial impact on patient management. Patients with severe PAH and low exercise functional capacity, for example, are poor responders to vasodilator therapy and have a worse prognosis after cardiac catheterization (2).
Stress Doppler echocardiography has been used in patients with ischemic and valvular heart diseases, among others, to assess exertional symptoms and to look for substantially abnormal hemodynamics not noted on resting echocardiography (3-7). To date, little is known about the dynamic pulmonary artery systolic pressure (PASP) response during exercise in subjects with borderline or mild to moderate pulmonary hypertension (PASP 30 to <60 mm Hg). Indeed, the cutoff point between clinically significant resting increases of pulmonary arterial pressure is ambiguous. Patients with PASP at or minimally above the upper limit of normal may be predisposed to development of more severe PAH at a later stage.
The primary objective of our study was to assess, with supine dynamic ergometer testing, the exercise capacity and pulmonary hemodynamics in patients with normal PASP, arbitrarily set at 30 mm Hg in our study, and different levels of mild to moderate PAH at rest in an otherwise structurally normal heart and in the absence of any known cause for secondary PAH. The secondary objective was to investigate the relationship between PASP at peak exercise and PASP at rest and its impact on exercise tolerance.
Methods
The study population consisted of 3 groups of patients, older than 18 years, who were prospectively enrolled in the study after they had undergone clinically indicated echocardiography in the Echocardiographic Laboratory at Mayo Clinic, Rochester, Minnesota: group 1 included control patients whose echocardiogram, ordered for reasons other than dyspnea, was completely normal, including a normal Doppler-derived PASP (arbitrarily set in our study at <30 mm Hg); group 2 consisted of patients whose echocardiogram was normal except for a PASP between 30 and 40 mm Hg; and group 3 consisted of patients who had a normal echocardiogram except for a PASP mildly to moderately more than the upper limit of normal (between 41 and 59 mm Hg). A very conservative definition of the upper limit of normal PASP was selected to ensure inclusion of patients with a marginal or equivocal degree of PAH. Exclusion criteria included 1) structural heart anomalies, including known coronary artery (>70% luminal diameter stenosis) or valvular disease (any degree of stenosis or moderate or more extensive valvular regurgitation), left atrial enlargement, left ventricular systolic or diastolic dysfunction, right ventricular dysfunction, congenital heart disease, or pericardial constriction; 2) untreated systolic hypertension; 3) history of abnormal thyroid function, anemia, parenchymal pulmonary disease, chronic obstructive lung disease, pulmonary embolism, or chronic liver disease; 4) abnormal chest radiographic finding (such as emphysematous changes, parenchymal pulmonary disease, mediastinal disease); 5) history of mediastinal tumor, fibrosis, or radiation; 6) serologic or clinical evidence of connective tissue disease; and 7) history of intake of chemotherapeutic agents such as cyclosporin, bleomycin, or anorexic medications. All patients were fully informed about the specific details of this study and its goal. Verbal consent was obtained and documented in the medical records as recommended by the Mayo Clinic Institutional Review Board. The study was approved by the Mayo Clinic Institutional Review Board.
The following medical information was obtained at enrollment: history of dyspnea or fatigue, prior pregnancies, and history of smoking. None of the study subjects had a family history of PAH.
Exercise Echocardiography Protocol
All study patients performed a symptom-limited supine dynamic bicycle exercise test after insertion of an intravenous catheter to use saline contrast, if needed, to optimize the continuous-wave Doppler signal of tricuspid regurgitation. The exercise protocol started at 25 W and increased by 25 W at 3-minute intervals until reaching limiting symptoms of dyspnea, chest pain, or fatigue or a maximal load of 200 W or the patient requested that the test be discontinued. The workload was kept constant with the onset of symptoms to ensure that the patient continued to exercise until ultrasound scanning was completed. Continuous electrocardiographic monitoring was used during exercise. Heart rate, cuff blood pressure (by automated machines), and oxygen saturation (finger oximetry) were monitored at 3-minute intervals. Cardiac output was measured from the stroke volume across the aortic valve multiplied by the heart rate. All subjects had structurally normal hearts, including normal inferior vena cava and pulmonary valve. Therefore, PASP was measured with the modified Bernoulli equation (PASP = 4V2 + RAP), where V is the peak tricuspid regurgitation velocity, and RAP is an assumed right atrial pressure of 5 mm Hg. These measurements were obtained at 3-minute intervals. If the tricuspid regurgitation velocity signal was incomplete, agitated saline contrast was used to optimize the signal. To allow for intersubject differences in duration of exercise, we determined a time slope of PASP, defined as the rate of increase of PASP with exercise in mm Hg per minute. This slope was calculated using simple linear regression of PASP versus minute of exercise (defined as the number of minutes corresponding to the stage at which each PASP was measured, i.e. 3, 6, and so on), determined separately for each subject (Fig. 1).
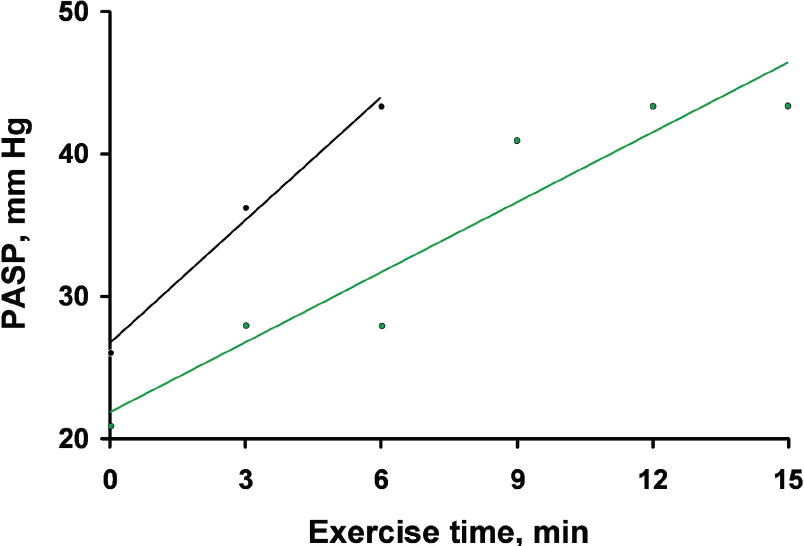
Calculation of the slope of the pulmonary artery systolic pressure (PASP) in 2 patients. This slope was calculated using simple linear regression of PASP versus minutes of exercise (defined as the number of minutes corresponding to the stage at which each PASP was measured), determined separately for each patient. The solid lines are the linear regression lines, calculated separately for each patient.
Statistics
Summary data are presented as mean ± SD or frequency counts. Two-group comparisons are based on the rank sum test or binomial χ2 test. Correlation of variables was investigated with Spearman correlation coefficient. Simple and multiple linear regression were used to determine univariate and multivariate predictors of PASP slope, change in PASP, or exercise duration. Simple and multiple ordinal logistic regression were used to assess the univariate and multivariate predictors of resting PASP group. A 2-sided 0.05 level of significance was used.
Results
Comparison of the 3 groups
Seventy-eight patients were enrolled into the study. Table 1 summarizes the pertinent demographic, clinical, and resting echocardiographic characteristics of the study population. Age and proportion of patients reporting a history of dyspnea increased with resting PASP. There was no statistical difference among the 3 groups with respect to sex, body mass index, treated hypertension, intake of birth control pills (among women), and left ventricular ejection fraction. Twenty-one patients had treated hypertension, 19 of whom had treatment with β-adrenergic blockers, calcium channel blockers, angiotensin-converting enzyme inhibitors, or receptor blockers. The intake of these medications was not statistically different among the 3 groups (P = 0.07). In addition, 22 patients had a history of smoking (28%), predominantly former smokers; the median number of years of smoking was 18 for group 1 and 20 for groups 2 and 3. There was no statistical difference among the 3 groups in terms of a history of smoking (P = 0.38). Interestingly, there was a statistically significant difference between groups in terms of prior pregnancies; a larger proportion of the women in the borderline and mild to moderate PAH groups reported pregnancies compared with the women in the normal resting PASP group (normal 55%, borderline 74%, mild 100%; P = 0.03). The number of pregnancies was not associated with a higher PASP at rest (P = 0.10). However, an additional pregnancy was associated with an increase in PASP at peak exercise of 2.6 mm Hg (P = 0.04). Table 2 summarizes the stress pulmonary hemodynamic findings in all study patients. There was no statistically significant difference among the 3 groups in terms of peak heart rate and systolic blood pressure. The cardiac index was slightly higher in groups 2 and 3 than in group 1, although the mean stroke volume was lower (95 mL for group 1, 88 for group 2, and 78 for group 3). This difference in cardiac index could be reflective of a slightly faster heart rate in group 3 than in groups 1 and 2, and of a difference in body surface area. In a multiple regression model, increased change in PASP with exercise was associated with increased change in cardiac index (P = 0.01), and there was an independent statistically significant trend upward from normal to mild pulmonary hypertension (P = 0.03, Fig. 2). Patients in the higher PASP groups (2 and 3) had a statistically significant higher peak PASP (group 1 46 ± 11 mm Hg, group 2 57 ± 11, group 3 73 ± 8; P < 0.001) and a shorter duration of exercise (group 1 13 ± 2 minutes, group 2 11 ± 3, group 3 8 ± 3; P < 0.001) (Fig. 3). The peak PASP correlated well with the resting PASP. The Pearson correlation coefficient was r = 0.71 (P < 0.001) (Fig. 4). Oxygen saturation at peak exercise negatively correlated with resting PASP (P = 0.007, r = −0.31) and less so with peak PASP (P = 0.07, r = −0.21).
Baseline demographic, clinical, and echocardiographic characteristics.

PASP, pulmonary artery systolic pressure.
Control patients older than 18 years with normal echocardiographic results, PASP 29 mm Hg or less.
Patients older than 18 years, borderline pulmonary hypertension, PASP 30 to 40 mm Hg.
Patients older than 18 years, mild to moderate pulmonary hypertension, PASP 41 to 59 mm Hg.
Cardiopulmonary stress exercise hemodynamic findings.

PASP, pulmonary artery systolic pressure.
Control patients older than 18 years with normal echocardiographic results, PASP 29 mm Hg or less.
Patients older than 18 years, borderline pulmonary hypertension, PASP 30 to 40 mm Hg.
Patients older than 18 years, mild to moderate hypertension, PASP 41 to 59 mm Hg.
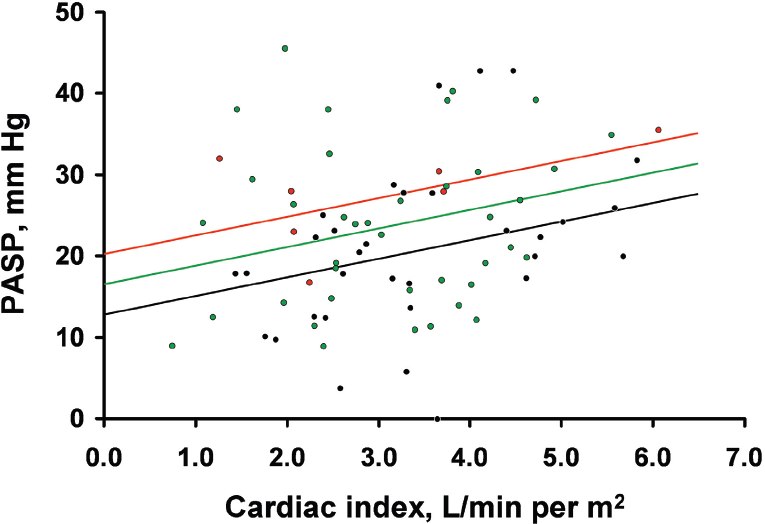
Change in pulmonary artery systolic pressure (PASP) and change in cardiac index with exercise, by resting PASP group. Black circles, group 1, normal echocardiographic results, PASP 29 mm Hg or less; green circles, group 2, borderline hypertension, PASP 30 to 40 mm Hg; red circles, group 3, mild to moderate pulmonary hypertension, PASP 41 to 59 mm Hg. The solid lines are the linear regression lines, showing the linear relationship between change in PASP and change in cardiac index for each of the 3 resting PASP groups.
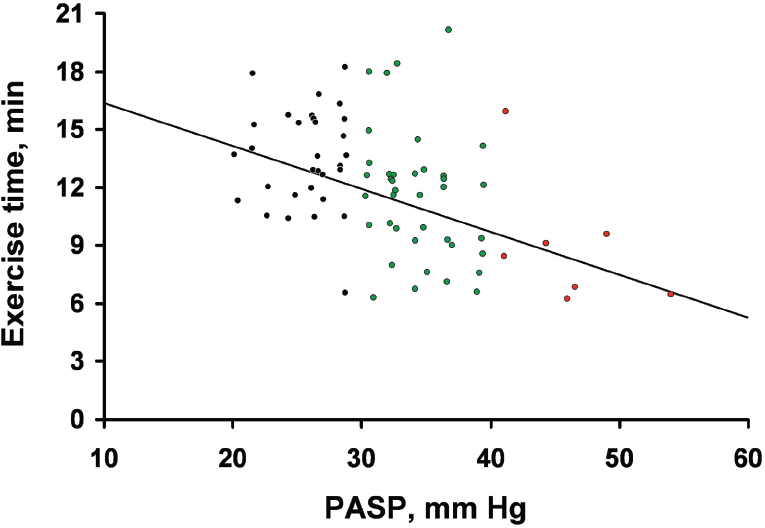
Resting pulmonary artery systolic pressure (PASP) and exercise time, by resting PASP group. Black circles, group 1, normal echocardiographic results, PASP 29 mm Hg or less; green circles, group 2, borderline hypertension, PASP 30 to 40 mm Hg; red circles, group 3, mild to moderate pulmonary hypertension, PASP 41 to 59 mm Hg. The solid line is the linear regression line showing the linear relationship between PASP at rest and exercise time.
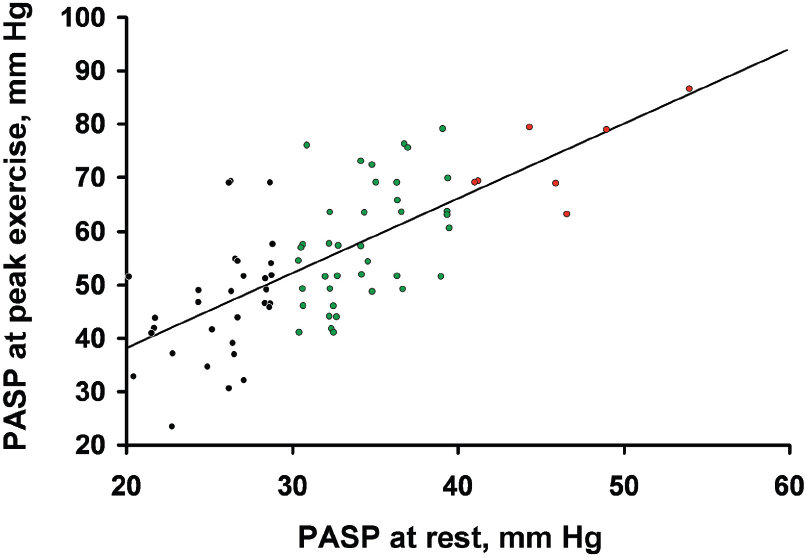
Correlation between peak and rest pulmonary artery systolic pressure (PASP). Black circles, group 1, normal echocardiographic results, PASP 29 mm Hg or less; green circles, group 2, borderline hypertension, PASP 30 to 40 mm Hg; red circles, group 3, mild to moderate pulmonary hypertension, PASP 41 to 59 mm Hg. The solid line is the linear regression line, showing the linear relationship between PASP at rest and at peak exercise.
Predictors of exercise PASP
On univariate analysis, the slope of PASP was positively associated with the PASP at rest (P < 0.001, Fig. 5), female sex (P = 07), increased age (P < 0.001), and intake of estrogen among women (P = 0.001) and negatively associated with oxygen saturation at peak exercise (P = 0.05). Prior pregnancy in women was associated non-significantly with higher PASP slope (0.2 mm Hg/min, P = 0.10). For every 10 mm Hg that PASP was higher at rest, the PASP slope increased by 0.9 mm Hg/min. On multivariate analysis, after adjustment for age, sex, systolic blood pressure, and presence of dyspnea, PASP slope was still independently related (P = 0.03) to resting PASP. Interestingly, the PASP slope was inversely associated with exercise time (P < 0.001) (Fig. 6). An increase in PASP slope of 1 mm Hg per minute was associated with a reduction in exercise time of 0.9 minute.

Change in pulmonary artery systolic pressure (PASP) with exercise and resting PASP pressure. Black circles, group 1, normal echocardiographic results, PASP 29 mm Hg or less; green circles, group 2, borderline hypertension, PASP 30 to 40 mm Hg; red circles, group 3, mild to moderate pulmonary hypertension, PASP 41 to 59 mm Hg. The solid line is the linear regression line, showing the linear relationship between PASP at rest and change in PASP (peak-resting).

Correlation between slope of pulmonary artery systolic pressure (PASP) and exercise duration. Black circles, group 1, normal echocardiographic results, PASP 29 mm Hg or less; green circles, group 2, borderline hypertension, PASP 30 to 40 mm Hg; red circles, group 3, mild to moderate pulmonary hypertension, PASP 41 to 59 mm Hg. The solid line is the linear regression line, showing the linear relationship between exercise time and PASP slope.
Discussion
The national prospective study of primary pulmonary hypertension (now referred to as idiopathic PAH) (8) showed not only that dyspnea on exertion is by far the most common initial complaint but also that the median time from onset of first symptom until the diagnosis of PAH is 1.27 years (mean, 2.03 years) and that it is not until 3 years that more than 90% of patients have their illness finally diagnosed. This long interval from initial symptoms to diagnosis and the poor outcome of these patients emphasize the need to develop strategies for earlier diagnosis. Whether unexplained borderline or mild to moderate pulmonary hypertension that worsens with exercise represents an earlier stage of the disease is unknown.
The current noninvasive assessment of PASP is limited to Doppler echocardiography with use of the tricuspid regurgitant velocity, with or without agitated saline, and modification of the Bernoulli principle (6,9). A borderline to moderately increased PASP at rest, until now, has had no known prognostic implications. However, in a manner similar to stress testing for myocardial ischemia and valvular heart disease or chronic lung disease, noninvasive assessment of PASP under dynamic conditions may disclose more substantial subclinical PAH and may provide prognostically pertinent data. Himelman et al. (6) showed that saline-enhanced Doppler evaluation of tricuspid insufficiency was a valuable noninvasive method of determining the exercise response in patients with chronic pulmonary disease and latent pulmonary hypertension not found at rest. The correlation with catheter measurements of PASP was excellent (0.98). The short-term administration of oxygen in these patients blunted the increase in the Doppler-derived PASP during exercise. Himelman et al. (7) also showed that the same technique can be used for continued evaluation after medical or surgical therapeutic interventions in a patient with pulmonary thromboembolism.
The pulmonary artery pressure response to exercise in healthy subjects has already been studied. Laskey et al. (10) showed, by invasive technique, that the PASP after maximal exercise in a control group ranged from 23 to 45 mm Hg (mean ± SD, 28 ± 8) and cardiac output ranged from 8 to 16.4 L/min (mean ± SD, 12.4 ± 2.5). Himelman et al. (6) found, with saline-enhanced Doppler echocardiography, that systolic PASP after exercise ranged from 25 to 45 mm Hg (mean ± SD, 31 ± 7), a mean increment of 11 mm Hg from resting measurements and an average increase in systolic blood pressure of 66 mm Hg. The average peak PASP in our control group was, indeed, 46 mm Hg, similar to that in the aforementioned reports. However, 1 patient in the control group had a peak PASP of 69 mm Hg, which might indicate subclinical pulmonary disease that was not evident at rest but became evident with exercise. Highly conditioned athletes, however, have been shown to have a peak PASP as high as 60 mm Hg after exercise (11). The dynamic response of PASP to exertion in these healthy subjects is thought to be related to a large increase in pulmonary blood flow, accommodated by a decrease in pulmonary vascular resistance. This normal dynamic functional response to exercise might be disturbed in patients with pulmonary vascular disease and associated pulmonary hypertension (2). Nootens et al. (12) found that when these patients exercise, the right ventricular stroke volume and ejection fraction decrease and the extent of tricuspid regurgitation increases, all of which limit the normal increase in cardiac output.
Laskey et al. (10) reported on exercise hemodynamics measured at cardiac catheterization in patients with PAH and noted a considerable increase in PASP. Our study showed similar findings in subjects with only borderline or mild to moderate pulmonary hypertension, findings that have not been demonstrated previously. Subjects with a higher resting Doppler-derived PASP had a significantly greater rate of increase in PASP with exercise (P = 0.003) and a significantly greater peak PASP (P < 0.001).
Grunig et al. (13) reported an abnormal PASP response to exercise in asymptomatic carriers of a gene mutation predisposing to the development of PAH, suggesting that stress Doppler echocardiography may be a useful tool to identify persons at risk of PAH even when PASP is normal at rest. Our findings and that of Grunig et al. raise a very important question about the validity and importance of stress echocardiography in the assessment of patients with borderline or mild to moderate pulmonary hypertension that is either unexplained, or more commonly, due to cardiac, pulmonary, or connective tissue diseases such as scleroderma. Our study also found that subjects with a higher resting Doppler-derived PASP in conjunction with this higher PASP slope had a significantly lower exercise time (P < 0.001) and lower oxygen saturation at peak exercise (P < 0.001). Rhodes et al. (2) noted an average functional capacity of 40% ± 36% (of that predicted for age, sex, and height) in 16 patients with PAH. Patients who were unable to exercise tended to have more severe hemodynamic derangements. Our findings and that of Rhodes et al. suggest that, in patients presenting for evaluation of dyspnea on exertion, hemodynamic stress Doppler echocardiography might provide useful information not only about the presence or absence of structural heart disease but also about the response of PASP with exercise and the degree of functional impairment that could explain the symptoms of dyspnea.
Whether such an accelerated response of the PASP in patients with borderline or mild to moderate pulmonary hypertension, especially in those with exertional dyspnea, is an early sign of progressive pulmonary vascular disease and subsequently more severe pulmonary hypertension will be answered only by a larger prospective study with long-term follow-up. Our study has some limitations that should be acknowledged. Follow-up serial echocardiography to assess changes of resting PASP over time was not done. The right atrial pressure was assumed to be 5 mm Hg in all patients, and no attempt was made to estimate it according to the inferior vena cava size and collapsibility or Doppler profile of the hepatic veins. However, in the presence of a structurally normal heart and in absence of severe PAH, it seems unlikely that the right atrial pressure would be significantly increased in most of our study patients. Minor differences in right atrial pressure would be unlikely to affect our results significantly. The pulmonary vascular resistance was not calculated. However, there were no statistically significant differences in cardiac index in the 3 groups studied with exercise (P = 0.64), and the observed relationship of PASP slope and exercise time may be a useful variable regardless of the cardiac index response. If such accelerated response of PASP in patients with borderline or mild to moderate PAH is indeed a prelude to more severe PAH, early recognition of this response of PASP to exercise and treatment might actually improve outcome.
Conclusion
Hemodynamic supine bicycle exercise echocardiography in patients with unexplained borderline or mild to moderate increase in PASP can be used to objectively assess the PASP response to exercise and the degree of functional impairment and could help explain the presence of dyspnea on exertion. This type of noninvasive assessment of pulmonary physiology in patients with borderline or mild PAH might have the potential for early detection of more severe pulmonary disease in patients with primary or secondary PAH, such as users of appetite suppressants, smokers, or patients with rheumatic heart disease or chronic thromboembolic disease. PASP slope, a new Doppler-derived hemodynamic variable, is inversely related to exercise duration and directly related to resting PASP. Hemodynamic exercise testing with Doppler echocardiography could have a substantial impact on the assessment and timing of different therapies and on outcome in patients with primary and secondary pulmonary hypertension.
Footnotes
Acknowledgment
Becky J. Hendrickson provided typing and secretarial assistance. Supported in part by Mayo Foundation.