
Abstract
Objectives
We retrospectively assessed both blood pressure response to management in a specialist Hypertension Clinic and the predictors of response.
Design
Retrospective data audit.
Setting
Hypertension Clinic at Guy’s and St Thomas’ Hospitals, London, UK.
Participants
One hundred and twenty-two sequential patients attending the clinic between January 2017 and October 2018. Patients were excluded if they had previously been seen in the clinic, failed to attend their initial appointment or did not return after their initial appointment.
Outcome measure
Change in blood pressure readings between first and last recorded appointments.
Results
Systolic blood pressure decreased from 149 ± 20 mmHg to 140 ± 17 mmHg, and diastolic blood pressure from 92 ± 13 to 86 ± 1 mmHg, between the first and last recorded appointments (P < 0.05 for each). Those patients who reached target blood pressure were significantly younger than those who did not (age 45 ± 14 versus 52 ± 17 years, P = 0.0171); however, the degree of blood pressure reduction was independent of age, and younger subjects had a baseline blood pressure significantly lower than older subjects. Sex, body mass index and lifestyle interventions had an important effect on blood pressure reduction; however, these were not associated with attainment of target blood pressure.
Conclusion
Specialist hypertension input is effective in helping patients to achieve target blood pressure, especially so in younger as compared to older hypertensive patients, but this appears to be related to the fact that blood pressure in younger patients is already closer to target at baseline. Blood pressure reduction is greater in women, those with higher body mass index and those who receive lifestyle interventions.
Introduction
Hypertension is defined within the National Institute of Health and Care Excellence (NICE) guidance 1 as blood pressure (BP) exceeding 140 mmHg systolic blood pressure (SBP) and/or 90 mmHg diastolic blood pressure (DBP), or being on anti-hypertensive treatment, and is an important preventable risk factor for cardiovascular disease. Stroke and ischaemic heart disease are increased by 10% and 7%, respectively, with each 2 mmHg increase in SBP, and hypertension is the leading cause of premature death and disability after smoking; 2 25% of adults in the UK are diagnosed with hypertension, and this figure rises to 50% in the over 65 age group. 3 Due to the ageing population, the prevalence of hypertension is on the rise. 3 However, hypertension is asymptomatic, and it is estimated that one-third of hypertensives are unaware of their condition; 4 therefore, the true prevalence is most likely higher than available statistics show.
Risk factors for developing hypertension can be classified according to whether they are non-modifiable or modifiable. Non-modifiable risk factors include age, ethnicity, sex and genetic predisposition, whilst modifiable factors include diet, exercise, weight, salt intake, alcohol consumption and stress. 5 Its management usually involves addressing the modifiable lifestyle factors, with the addition of anti-hypertensive drug therapy where lifestyle measures alone do not suffice in attaining target BP.
The principal goal of hypertension treatment according to NICE guidance is to reduce BP to <140/90 mmHg, with the aim of preventing cardiovascular morbidity and mortality. A relatively small reduction in SBP is needed to show reduced cardiovascular disease risk: it is estimated that a 5 mmHg SBP reduction can lead to 7% decrease in all-cause mortality, with a 14% and 9% decrease in mortality from stroke and coronary heart disease, respectively. 6
Hypertension is managed primarily in a primary care setting in the UK. If BP is not reduced to target, NICE recommends referral to a specialist Hypertension Clinic. Additionally, there are other specific criteria for specialist referral, namely patient age <40 years, hypertension during pregnancy, accelerated hypertension and suspicion of secondary hypertension.
The population of hypertensive patients attending a specialist clinic is therefore a highly selected one, whose response to BP treatment is expected to be more limited than that seen in general practice. The primary objective of the present study was to assess the degree of reduction in BP that was attained by patients referred to a specialist Hypertension Clinic, namely that at Guy’s and St Thomas’ Hospitals, London, UK. The secondary objective was to determine which patient-specific factors, if any, were useful in predicting response versus non-response in this population.
Methods
We retrospectively audited data from 122 sequential patients who attended the Guy’s and St Thomas’ Hypertension Clinic between 1 January 2017 and 31 October 2018. Patients were excluded if they had previously been seen in the clinic, if they had documented white-coat hypertension (as assessed by either ambulatory or home BP monitoring), if they failed to attend their initial appointment or if they did not return after their initial appointment. In line with NICE guidance, 1 the majority of (but not all) patients referred to the clinic were those with resistant hypertension, age < 40 years, evidence of target organ damage or those with suspected secondary hypertension.
Data collected consisted of the following:
Age Sex Ethnicity First and final recorded BP readings Body mass index (BMI) Anti-hypertensive medications at baseline Implementation or non-implementation of lifestyle measures for BP reduction.
At each clinic visit, BP was measured seated in a chair, following at least 5 minutes’ rest, on three occasions, according to British & Irish Hypertension Society criteria (https://bihsoc.org/resources/bp-measurement/measure-blood-pressure/), using an automated monitor (Omron M10-IT), except where the patient had an irregular pulse when the BP was measured manually instead. BP readings were averaged at each appointment, and response was determined from the change in mean BP readings between their first and last recorded appointments.
Data were collated using Microsoft Excel and analysis was performed on GraphPad Prism version 8. Covariates examined consisted of age, sex, BMI, ethnicity and number of anti-hypertensives at baseline.
Data are presented as mean ± standard deviation. Statistical analysis for continuous variables was by paired or unpaired Student’s t test, or by correlation analysis, as appropriate; and by Chi squared analysis for categorical variables. In all cases, P < 0.05 (two-tailed) was taken as indicating statistical significance.
Results
The mean BP of patients at their initial appointment in the clinic was a systolic of 149 ± 20 mmHg and a diastolic of 92 ± 13 mmHg. At their last recorded appointment, mean BP had fallen to a systolic of 140 ± 17 mmHg and a diastolic of 86 ± 11 mmHg (P < 0.0001 for each), as shown in Figure 1. Overall, 53% of patients had reached target BP (SBP < 140 mmHg and DBP < 90 mmHg) at their last appointment, whereas only 35% of patients were at target at the time of their initial appointment. Moreover, we found that age was a predictor of likelihood of reaching target BP, in that those who reached target BP were younger than those who did not (age 45 ± 14 versus 52 ± 17 years, P = 0.0171), as demonstrated in Figure 2(a).

Systolic (a) and diastolic (b) blood pressure of patients at their first and last recorded appointments.

Effect of different parameters on likelihood of attaining target BP. (a) Age of patients who achieved target SBP <140 mmHg compared to those that did not. (b) Number of anti-hypertensive medications at baseline in patients that achieved target SBP <140 mmHg and those that did not. (c) Percentage of patients, broken down by ethnicity, who achieved target SBP <140 mmHg compared to those that did not. (d) Percentage of men and women that achieved target SBP < 140 mmHg compared to those that did not. (e) BMI of patients who achieved target SBP < 140 mmHg compared to those that did not. (f) Percentage of patients who did or did not receive lifestyle intervention, who achieved target SBP < 140 mmHg compared to those that did not.
Tables 1 and 2 display the patients’ medications at first and last appointments, respectively; and Table 3 shows the changes in anti-hypertensive medications instituted in the interval between first and last appointments. The only clear difference seen was that patients who reached target BP were more likely to be on thiazide-like diuretics at their last appointment. Both at baseline and at last appointment, patients not reaching target BP were marginally more likely to be on other vasodilator drugs, though this was of borderline significance. Patients in the group who did not reach target were more likely to have had angiotensin receptor blockers, beta blockers, organic nitrates or potassium-sparing diuretics added in to their therapy, but despite these additions they remained above target BP.
Classes of anti-hypertensive medications taken at first appointment, in patients that reached target SBP (<140 mmHg) compared to those that did not.

Values in table are absolute numbers of patients, with percentages given in brackets.
Classes of anti-hypertensive medications taken at last recorded appointment, in patients that reached target SBP (<140 mmHg) compared to those that did not.

Values in table are absolute numbers of patients, with percentages given in brackets.
Changes in classes of anti-hypertensive medications between first and last recorded appointment, in patients that reached target SBP (<140 mmHg) compared to those that did not.
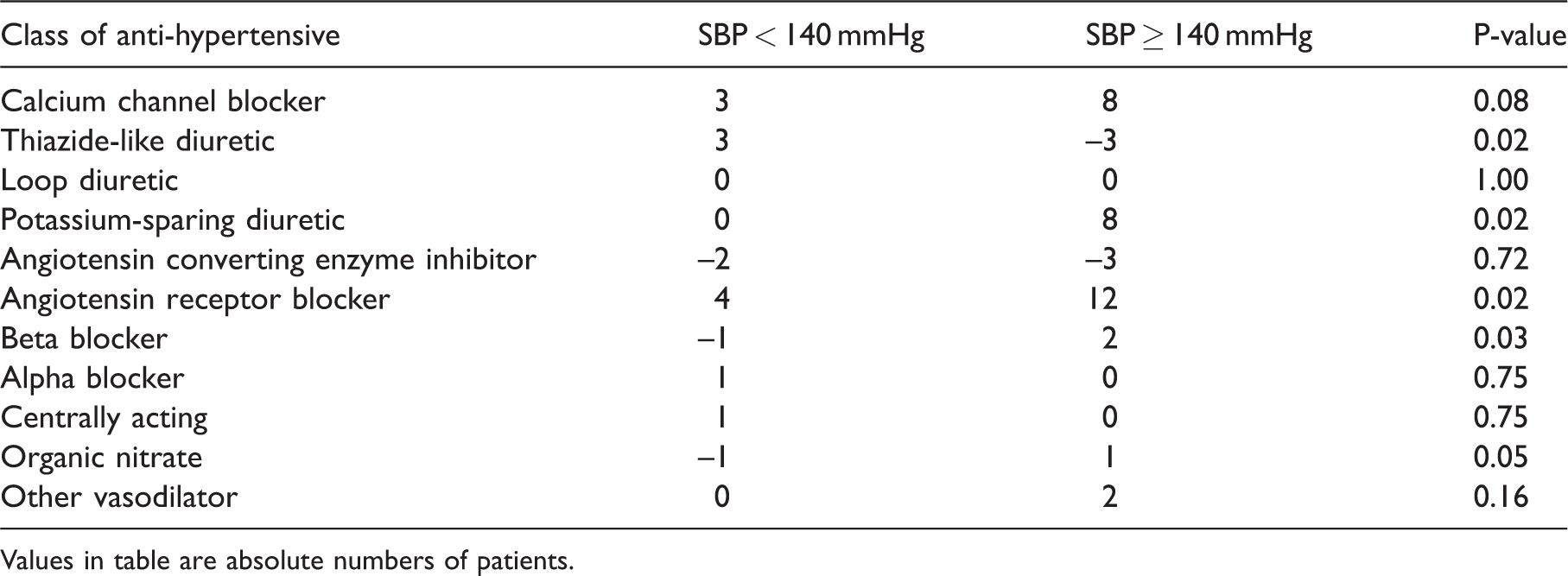
Values in table are absolute numbers of patients.
As would be predicted, baseline BPs differed according to age, with SBP increasing progressively with increasing age (P = 0.0002), as shown in Figure 3(a). Moreover, we found that the degree of reduction in both SBP and DBP was independent of age (Figure 3(b) and (c)).
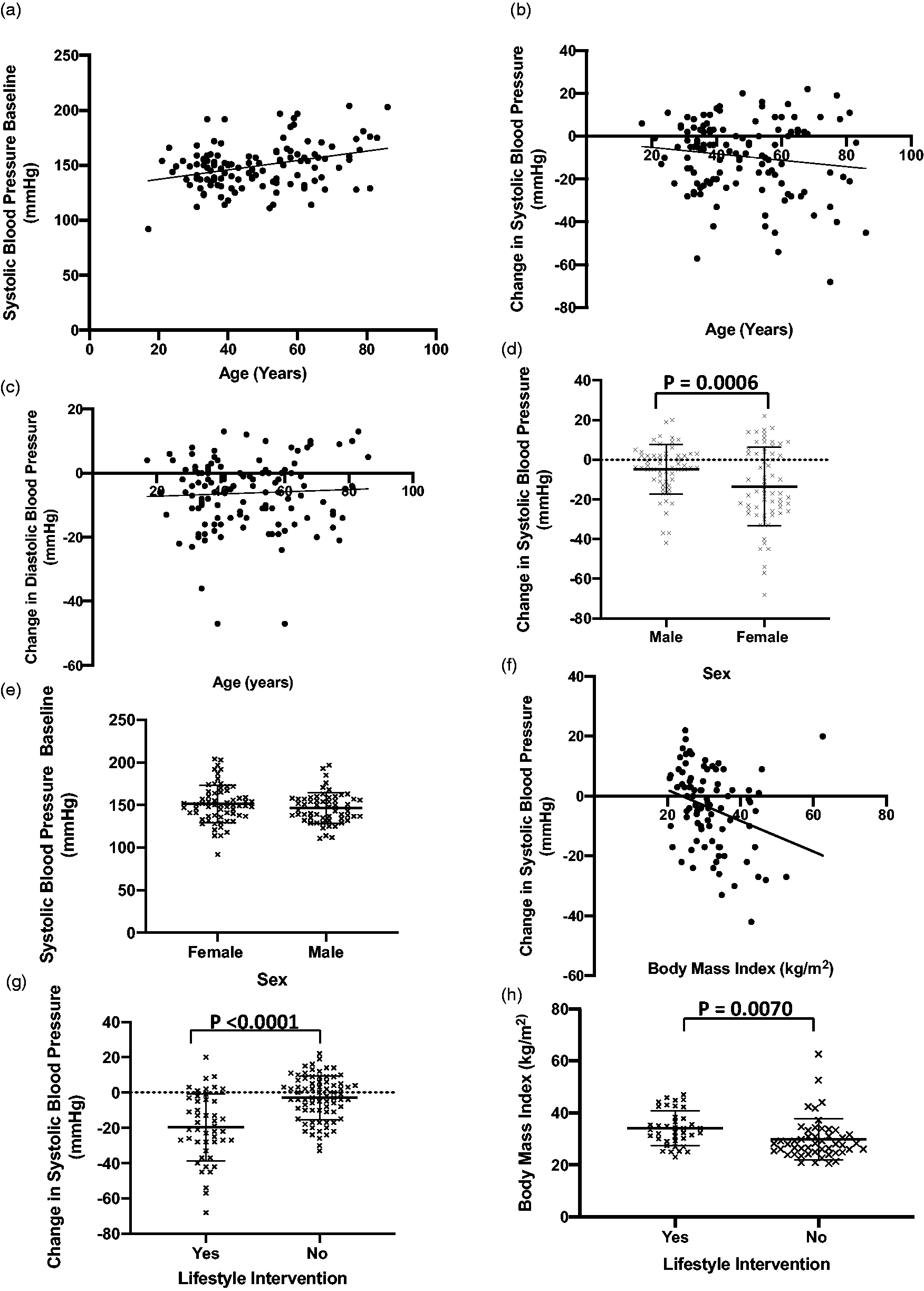
Effect of different parameters on degree of reduction in SBP. (a) Baseline SBP as a function of age (r = 0.3320, P = 0.0002). (b) Change in SBP between first and last appointment as a function of age (r = −0.1363, P = 0.1343). (c) Change in DBP between first and last appointment as a function of age (r = 0.05175, P = 0.5713). (d) Change in SBP in female compared to male patients. (e) Baseline SBP in female compared to male patients. (f) Change in SBP as a function of BMI (r = −0.2941, P = 0.0054). (g) Change in SBP in patients that received lifestyle intervention and those that did not. (h) BMI in those that received lifestyle interventions and those that did not.
We also explored other factors which may determine response to treatment (Figures 2 and 3). Specifically, we examined the possible relationship between BP reduction and BMI, number of anti-hypertensive agents prescribed at baseline, ethnicity (white British, black African or black Caribbean), sex and the implementation of lifestyle interventions for BP management. Sex, BMI and lifestyle intervention were all predictors of degree of reduction in BP (Figure 3(d), (f) and (g)). Female patients exhibited a significant reduction in SBP compared to males (females 14 ± 18 versus males 5 ± 13 mmHg, P = 0.0006), despite no difference in baseline SBP between the sexes (Figure 3(e)). Increasing BMI was associated with a greater reduction in SBP (P = 0.0054 by correlation analysis). Patients receiving lifestyle intervention had a significantly greater SBP reduction compared to those who did not (20 ± 19 versus 3 ± 12 mmHg, P < 0.0001). Of note, those patients who received lifestyle intervention had higher BMI that those who did not (34 ± 7 versus 30 ± 8 kg/m2, P= 0.0070), as shown in Figure 3(h). Ethnicity and number of anti-hypertensives at baseline showed no relationship with degree of reduction in SBP. Furthermore, none of these factors were predictive of attainment of target BP (Figure 2(b) to (f)).
Discussion
In this study, the primary aim was to ascertain the effectiveness of BP lowering in patients attending a specialist Hypertension Clinic. This cohort differs from the general hypertensive population, in that they have been referred by their primary care physicians due to one or more of a number of problems in reducing BP according to standard guidelines. We found that, in this unselected cohort of patients, both SBP and DBP were significantly reduced, from a mean of 149/92 mmHg at their first appointment to 140/86 mmHg at their last recorded appointment. Indeed, 53% of patients reached target BP, defined as SBP < 140 mmHg and DBP < 90 mmHg, whereas only 35% were at target at the time of their initial appointment. Literature on the effectiveness of hypertension clinics within the UK is sparse. However, studies from around the world show similar efficacy. An audit on hypertension clinics in Hong Kong concluded that 53% of patients reached target BP < 140/90 mmHg; 7 and an American study found 52% patients reached target at their final recording, whilst 18% of patients were at goal BP at their initial appointment. 8 On the other hand, another study in a nurse-led hypertension clinic, where patients were seen every three weeks for four years, reported that 95% of patients attained target BP of <140/90 mmHg. 9
It has previously been shown that reduction of SBP by as little as 5 mmHg can lead to 7% decrease in all-cause mortality, with decreases of 14% and of 9% in stroke and coronary heart disease mortality, respectively. 6 The reductions observed in our patient cohort are likely therefore to translate to important benefit in terms of cardiovascular outcomes. However, failure of BP to fall to target can occur for many reasons, including suboptimal treatment, disease progression, non-adherence, antagonising substances (for example caffeine, cocaine, non-steroidal anti-inflammatory drugs) and co-morbidities (such as anxiety disorders, chronic pain, sleep apnoea and obesity). 10 It is estimated that between 50 and 80% of patients on anti-hypertensive drugs do not take their medications as prescribed. 11 Studies have shown that resistant hypertension has a 10–20% population prevalence and will be higher in patients referred to a specialist Hypertension Clinic. 12 Therefore, it is unsurprising that over 40% of our patients did not attain target. However, of note, 35% of patients that were referred to our clinic had BPs below target already; this is in large part attributable to the fact that many patients were put on medication by their general practitioners prior to referral to our clinic for investigation of possible secondary causes of hypertension. On the other hand, the majority of our patients were referred because of refractory hypertension, intolerance to multiple anti-hypertensive medications, young age of onset or pregnancy-associated hypertension. Overall, the reductions observed in this study are likely to translate to reduced cardiovascular events over the long term.
Although the current BP target according to NICE guidance is < 140/90, there is increasing scrutiny over this arbitrary cut-off point. For example, the American College of Cardiology have lowered their target to 130 mmHg systolic. 13 There is emerging evidence that tighter control of BP, aiming for a target as low as 120 mmHg, reduces cardiovascular complications and premature mortality even further. 14 Additionally, the recent joint guidelines for management of arterial hypertension by the European Society of Cardiology and the European Society of Hypertension 15 suggest that SBP exceeding 115 mmHg increases risk of developing heart disease. However, they still generally advocate treatment at a SBP ≥ 140 mmHg, as this appears to be the point above which the benefits of treatment outweigh the risks of medication. Target BP in management of hypertension remains a subject of much controversy and may indeed vary not only between guidelines but between patients depending on a multitude of factors including co-morbidities and presence of other risk factors.
We also wished to determine which, if any, of a number of covariates (age, sex, BMI, number of anti-hypertensives prescribed at baseline, implementation or non-implementation of lifestyle interventions in the clinic) had any influence on BP reduction or attainment of BP target, defined as reaching a target SBP < 140 mmHg. The only one of these factors which predicted attainment of target BP in our study was age. The mean ages in those that reached target and those that did not were 45 and 52 years, respectively. Nevertheless, the degree of BP reduction did not correlate directly with age, and baseline SBP was lower in younger patients, suggesting that greater achievement of target BP in younger patients was likely explained by the fact that their BP was already closer to target at baseline.
Although sex, ethnicity, number of anti-hypertensives at baseline, implementation of lifestyle interventions and BMI were not different in patients that reached target BP compared to those who did not, our study demonstrates that nevertheless sex, BMI and lifestyle intervention all have important effects on degree of BP lowering. Female patients exhibited a greater SBP decrease than did male patients, despite no difference between men and women in baseline SBP. Moreover, patients with higher BMI were likely to exhibit a greater reduction on SBP, as were those who were given lifestyle interventions. Additionally, we found that lifestyle interventions were more likely to be given in those patients with higher BMI. It was not possible, from this limited dataset, to examine whether BMI and lifestyle interventions were independent predictors of response. This needs to be explored in future studies.
Our study also shows that patients reaching target BP were more likely to have had thiazide-like diuretics added in to their therapy. In those not reaching target BP, patients were more likely to have had angiotensin receptor blockers, beta blockers, organic nitrates or potassium-sparing diuretics added in, but despite such additions target BP was not achieved.
In conclusion, this study shows that referral to a specialist Hypertension Clinic is effective in reducing BP, but BP remains above target in almost half of patients despite this. Younger patients being more likely to attain target BP than older patients, but this is explained by their lower BP levels at baseline. Sex, BMI and lifestyle intervention have important effects on degree of BP reduction, but none of these were associated with likelihood of attainment of target BP in this study. Our study reveals important determinants of BP response in patients referred to a specialist Hypertension Clinic.
Footnotes
Acknowledgements
Contributorship
All authors collected and analysed the data, and wrote the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
None.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantors
All the authors act as guarantors for this article.