
Abstract
Coronary spasm plays an important role in the pathogenesis of variant angina as well as ischaemic heart diseases. Treatment with vasodilators such as long-acting calcium channel blockers and long-acting nitrates is generally effective in preventing coronary spasm; however, in some patients coronary spasm is refractory to standard therapy. Because of endothelial dysfunction, hyper-reactivity of coronary smooth muscle cells and other triggering factors involved in the pathogen-esis of coronary spasm, drugs capable of improving these conditions may be effective in preventing medically refractory coronary spasm. In addition, a spasm provocation test is frequently performed when diagnosing coronary spasms. Although intracoronary administration of nitroglycerin generally relieves the coronary spasm that results from this test, we have encountered patients who suffered haemodynamic instability during the test. Drugs that stabilize haemodynamics and dilate the coronary artery are effective in such situations. We review treatment options for coronary spasm that are refractory to the standard oral medications and to intracoronary infusion of nitroglycerin during the spasm provocation test.
Introduction
Coronary spasm is defined as a dynamic, transient reduction in the luminal diameter of epicardial coronary arteries due to increased vasomotor tone, leading to myocardial ischaemia. It is widely accepted that coronary spasm plays an important role in the pathogenesis of not only variant angina but also of ischaemic heart diseases, including other forms of angina, acute myocardial infarction and ischaemic sudden death (1). Coronary spasm was first reported as a variant angina by Prinzmetal et al. (2), who showed reversible myocardial ischaemia accompanied by ST segment elevation on the electrocardiogram (ECG). In fact, ST segment elevation on the ECG is frequently observed during coronary spasm, although ST segment depression is sometimes seen when the coronary artery is not completely occluded because of coronary spasm. Therefore, clinical syndromes caused by coronary spasm, including variant angina, are collectively known as coronary spastic angina (CSA).
Long-acting calcium channel blockers (CCBs) are widely used in patients with CSA, and it has been shown that long-acting CCBs are effective in preventing coronary spasm (3-5). However, some patients with CSA exhibit symptoms despite being treated with vasodilators such as long-acting CCBs and/or long-acting nitrates. In general, the pathogenesis of coronary spasm is thought to involve several mechanisms, such as endothelial dysfunction (6-9), hyper-reactivity of coronary smooth muscle cells (10, 11) and other triggering factors, such as activation of the parasympathetic nervous system and alpha-adrenergic receptors (12, 13). Therefore, drugs that can improve these abnormalities may be effective in preventing medically refractory coronary spasm.
The spasm provocation test is frequently performed to diagnose CSA. Intracoronary infusion of acetylcholine and/or ergometrine maleate for the spasm provocation test is effective in producing coronary spasm with few major complications (14, 15). If coronary spasm is induced by intracoronary infusion of one or the other of these provocating drugs, intracoronary administration of nitroglycerin can relieve the coronary spasm immediately in most patients who have undergone the spasm provocation test. However, we have encountered a few patients with CSA who became haemodynamically unstable because of severe and prolonged coronary spasm during the test. Furthermore, intracoronary infusion of nitroglycerin worsens haemodynamic instability under such conditions. In such cases, intracoronary or intravenous infusion of drugs that not only dilate the coronary artery but also improve haemodynamics may be effective in relieving severe coronary spasm.
Here, we review treatments for coronary spasm that is refractory to the standard therapy with oral vasodilators, and describe countermeasures for severe coronary spasm accompanied by haemodynamic instability during the spasm provocation test.
Conventional Therapy for Coronary Spasm
The first step in treating coronary spasm is to prohibit cigarette smoking. This is important because smoking is one of the major risk factors for coronary spasm (16). Treatment with long-acting CCBs is the first-line therapy, and additional long-acting nitrates and/or nicorandil are also considered effective. The use of long-acting CCBs has been shown to decrease the frequency of angina attacks and to prevent coronary spasm (3-5, 17). Nicorandil, which has the vasodilatory effect of both nitroglycerin and potassium channel openers, has been shown to be effective in patients with CSA (18, 19). However, there are chances of potential coronary spasm in future (20, 21), and therefore, patients should be advised to consult a cardiologist before discontinuing the vasodilators even if they have been symptom-free for a long time. Abrupt cessation of vasodilator therapy sometimes causes severe rebound attacks of angina. Monotherapy with β-blockers should be avoided because it can worsen coronary spasm as a result of a relative increase in ≈-adrenergic activity (22). Nevertheless, when patients experience symptoms sublingual nitrates should be used without hesitation.
Pharmacological Treatment for Medically Refractory Coronary Spasm
In most patients with CSA, conventional vasodilator therapy is effective in preventing coronary spasm. However, some patients do not respond to such conventional therapy. In patients with medically refractory CSA, various drugs have been tried, some of which have proved effective in preventing medically refractory coronary spasm. The pathogenesis of coronary spasm may be multifactorial (Fig. 1) (1, 6-13, 23-35), and drugs that are effective against these multiple factors may have potential for preventing medically refractory coronary spasm.
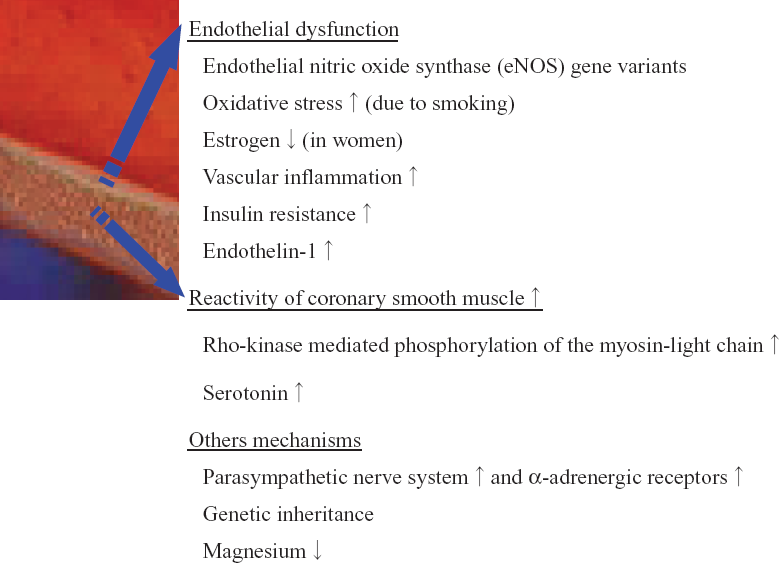
Possible pathogenesis of coronary spasm.
Endothelial Dysfunction
Oxidative stress-induced endothelial dysfunction is reportedly involved in the pathogenesis of coronary spasm (24, 26, 29, 30). Oxidative stress is increased and endothelial function is impaired in patients with CSA, and administration of vitamin C (24, 29, 30) or vitamin E (26) has been shown to improve oxidative stress and endothelial dysfunction. Furthermore, Miwa et al. (23) showed that vitamin E was reduced in patients with active CSA, and oral vitamin E reduced the frequency of angina attacks in such patients. In addition, Miyamoto et al. (33) also showed that the level of vitamin E was reduced in patients with CSA, and vitamin E supplementation improved fibrinolytic activity and decreased the frequency of angina attacks in such patients. Therefore, antioxidant vitamin C and/or vitamin E may be effective in treating medically refractory coronary spasm. In postmenopausal women with CSA, estradiol supplementation improved endothelial function and decreased the degree of hyperventilation-induced coronary spasm attacks (36). At present, estrogen supplementation is not recommended for the prevention of cardiovascular disease because of its adverse effects (37, 38). Estrogen therapy is best limited to postmenopausal women with severe CSA and no other treatment option. Low-grade inflammation is assessed based on the C-reactive protein levels, which is a highly sensitive test and has been associated with the presence of coronary spasm (35). Vascular inflammation causes endothelial dysfunction (39); thus, vascular inflammation may be one of the mechanisms of endothelial dysfunction in patients with CSA. Drugs such as statins, which have the ability to reduce vascular inflammation (40), may be effective in the treatment of medically refractory CSA. Regarding inflammation, there have been reports of patients with medically refractory CSA complicated by bronchial asthma (41). Corticosteroid is effective in preventing coronary spasm in such patients (41). Corticosteroid may be one of the options for treating medically refractory CSA. Furthermore, it has been shown recently that a high concentration of low-density lipoprotein cholesterol causes progression of coronary atherosclerosis in patients with CSA (42). This finding appears to support the effect of statins on the coronary vasculature in patients with CSA, an effect that leads to suppression of medically refractory coronary spasm. Insulin resistance may also be involved in the mechanism responsible for endothelial dysfunction in patients with CSA (27, 29). Murakami et al. (27) reported that administration of a thiazolidinedione improved endothelial function and reduced the frequency of angina attacks in patients with CSA. Thus, drugs that can improve insulin resistance may be considered for treating medically refractory coronary spasm. Finally, the plasma concentration of endothelin-1 was elevated in two patients with CSA after they consumed alcohol (28). Although this study included only a small number of patients without any control arm, the results indicated a possible elevation of endothelin-1 endothelial dysfunction in patients with CSA, which is thought to play a role in the pathogenesis of coronary spasm. Although there is no data suggesting the effectiveness of endothelin antagonists in patients with CSA, these may prove to be effective in patients with medically refractory CSA.
Hyper-reactivity of coronary smooth muscle cells
It is believed that the hyper-reactivity of coronary smooth muscle cells is involved as the main cause of coronary spasm (10, 11). In porcine models of coronary spasm, it has been demonstrated that an increase in rho kinase-mediated phosphorylation of the myosin light chain plays a causal role in coronary spasm (11). Furthermore, intracoronary infusion of fasudil, a selective rho kinase inhibitor, improves coronary vasospasm, including chest symptoms, ischaemic ECG findings and angiographic findings, in response to acetylcholine in patients with CSA (43). At present, the selective rho kinase inhibitor is available only by injection. If an oral form of a selective rho kinase inhibitor becomes available clinically, it would be useful in preventing medically refractory coronary spasm.
Serotonin (5-hydroxytryptamine; 5HT), which is locally released from aggregated platelets, is one of the most important vasoactive substances and there are several studies regarding the relationship between serotonin and CSA. The genes for the 5HT(1B) and 5HT(2A) receptors are expressed in human coronary arterial smooth muscle cells (44). It has also been reported that the serotonin concentration is elevated in patients with CSA (45). Furthermore, intracoronary infusion of serotonin or a serotonin receptor agonist can provoke coronary spasm (46, 47). Thus, abnormality of serotonin may cause coronary spasm, mediated by hyper-reactivity of coronary smooth muscle. In an animal model, a selective 5-HT2A serotonergic receptor antagonist prevented serotonin-induced coronary spasm (48), and it is possible that serotonin receptor antagonists are effective to some extent in patients with medically refractory CSA.
Other Triggering Factors
Activation of the parasympathetic nervous system and ≈-adrenergic receptors is also thought to be responsible for coronary spasm (12, 13). Denopamine, a selective β1-adrenoceptor agonist, has been shown to decrease the frequency of coronary spasm attacks and the need for nitro-glycerin without causing any major complications (49). In addition, it has been shown that ≈-receptor blockers decrease the frequency of angina attacks (22, 50). These drugs may be useful for improving the symptoms of medically refractory coronary spasm.
In addition to the mechanisms described above, there are several other possible mechanisms for the pathogenesis of coronary spasm. A deficiency in magnesium is one of the factors responsible for coronary spasm (51-53). Several studies have shown that intravenous administration of magnesium sulphate improves clinical symptoms associated with coronary spasm (54-56). Oral magnesium supplementation has been shown to improve endothelial function and exercise tolerance in patients with coronary artery disease (57), but there is no reported study investigating the effect of oral magnesium supplementation in patients with medically refractory CSA. Furthermore, a relation between panic disorder and coronary spasm has been described (58), and it has been shown that the autonomic imbalance is involved in the mechanism of CSA (59). Although there are no established data, oral magnesium supplementation or antidepressant agents may be of some benefit for reducing angina attacks in patients with medically refractory CSA.
Non-Pharmacological Treatment for Medically Refractory Coronary Spasm
Non-pharmacological therapies for medically refractory CSA have been documented (60-68). Percutaneous coronary stenting has been shown to be effective in such cases without organic coronary stenosis (60, 61, 63) and in patients with organic coronary stenosis (62, 64). The restenosis rate after the implantation of a bare-metal stent is reported to be comparable between patients with and without CSA (64). Most of the studied patients had organic coronary stenosis, and the restenosis rate remains unclear in patients with CSA without organic coronary stenosis. Furthermore, in several studies coronary spasm continued to occur in the stented vessel or in other vessels after stenting, but did not occur at the stented lesion (65, 67, 68). Pharmacological therapy with vasodilators such as long-acting CCBs is essential in patients with medically refractory CSA, even though symptoms improve after coronary stenting. Recent studies have reported new cases of coronary spasm following implantation of a drug-eluting stent (69, 70); thus, coronary stents should be selected very carefully for patients with CSA. Furthermore, there are two reported cases of medically refractory CSA without significant coronary stenosis who underwent coronary aorta bypass grafting (CABG) with the internal mammary artery (66). The postoperative course was uneventful, but spasticity remained in the other vessels (20). Thus, the use of CABG for medically refractory CSA should be considered carefully.
Treatment for Life-Threatening Arrhythmia Complicated by Coronary Spasm
In patients with CSA, life-threatening arrhythmias such as ventricular tachycardia and ventricular fibrillation are frequently observed during coronary spasm. These arrhythmias are the main cause of cardiac death associated with coronary spasm. There are several reported cases of CSA and documented ventricular fibrillation. The patients were treated with an implantable cardioverter defibrillator (ICD) in addition to conventional vasodilator therapy (71-73). Al-Sayegh et al. reported two shocks in a patient within 4 months after ICD implantation because of recurrent ventricular fibrillation under conventional medical therapy. ICD implantation has both advantages and disadvantages for patients with both CSA and malignant arrhythmia, and its application should be considered carefully. In addition, the direct effect of shock delivery on coronary spasm remains unclear.
Countermeasures for Severe Coronary Spasm with Haemodynamic Instability during Spasm Provocation Test
Coronary angiography with the spasm provocation test is useful in establishing a final diagnosis of coronary spasm. Ergometrine maleate and acetylcholine are the two main agents used for spasm provocation test. Spasm provocation tests that use intracoronary infusion of these drugs are effective in producing coronary spasm with few major complications (14, 15), but the duration of coronary spasm seems to be shorter with the use of acetylcholine than with the use of ergometrine maleate. Thus, acetylcholine may be safer than ergometrine maleate in spasm provocation tests on both the left and right coronary arteries. However, acetylcholine itself causes sinus bradycardia and atrioventricular block, and thus a temporary pacemaker is needed to prevent such arrhythmias during acetylcholine infusion. A positive provocative test is defined as angiographic evidence of subtotal or total occlusion of a coronary artery due to coronary spasm accompanied by chest pain and/or ST segment changes on the ECG.
Nitroglycerin is infused intracoronarily to relieve coronary spasm when coronary spasm is diagnosed. However, severe and prolonged coronary spasm that does not respond to intracoronary administration of nitroglycerin can occur during the spasm provocation test. Sueda et al. (14) reported that major complications such as ventricular tachycardia and shock resulting from severe coronary spasm occurred during the spasm provocation test in 3 of 715 patients (0.4%) in whom the test was performed with acetylcholine. At our institution, 2 of 333 patients (0.6%) who underwent the spasm provocation test during the past 7 years suffered from shocks. Malignant arrhythmia that occurs during the spasm provocation test should be treated with unsynchronized electrical shock. Although the effect of electrical shock on coronary spasm is unclear, severe coronary spasm is usually relieved after such therapy. For haemodynamic instability due to severe coronary spasm during the spasm provocation test, intracoronary administration of nitroglycerin may not be effective in reopening the completely occluded coronary artery when coronary blood flow is severely reduced because of the shock. Furthermore, intracoronary infusion of nitroglycerin may even worsen the haemodynamics, leading to prolongation of the coronary spasm.
Intracoronary infusion of nicorandil is effective in treating severe coronary spasm (74, 75). Intracoronary infusion of this drug is not officially recommended because of the possibility of malignant arrhythmia, such as ventricular fibrillation, but we often administer 1 mg nicorandil intracoronarily to increase coronary blood flow without affecting the haemodynamics negatively, especially in patients with slow flow phenomenon after percutaneous coronary intervention. In addition, intracoronary administration of diltiazem, a CCB, has been also shown to relieve nitroglycerin-resistant coronary spasm without significantly decreasing blood pressure (76). These vasodilators may be able to relieve severe coronary spasm and should be tried under such conditions.
These vasodilators cannot elevate blood pressure, however, and the vasodilating effects of these drugs might be limited under conditions of hypotension and decreased coronary blood flow because of severe shock-induced coronary spasm. Under this condition, drugs that can elevate blood pressure to increase coronary blood flow dramatically and can dilate the coronary artery are ideal. Sueda et al. (14) reported the use of noradrenaline for shock during the spasm provocation test. According to our experience, intracoronary administration of low-dose adrenaline (2 μg) is also effective in relieving severe coronary spasm during the spasm provocation test (Fig. 2). The relief achieved with intracoronary infusion of noradrenaline or adrenaline may be due to coronary vasodilation, which is mediated by stimulation of β1-adrenoreceptors, and to the increase in coronary blood flow in response to the increase in blood pressure.

A representative case of severe coronary spasm that occurred after the spasm provocation test, and was relieved by intacoronary infusion of adrenalin.
Coronary angiograms of the right coronary artery.
As mentioned above, intracoronary infusion of fasudil, a selective rho kinase inhibitor, improved acetylcholine-induced coronary vasospasm in patients with CSA (43), and this drug may be effective for improving severe coronary spasm in patients during the spasm provocation test. However, this drug can decrease blood pressure, leading to a decrease in coronary blood flow. Furthermore, intravenous administration of magnesium sulphate improved clinical symptoms associated with coronary spasm (54-56), but because magnesium sulphate does not have a rapid vasodilating effect and can also decrease blood pressure this drug may not be suitable for use under conditions of severe coronary spasm with haemodynamic instability. In addition, Sueda et al. (77) showed that intracoronary administration of ozagrel, which is a thromboxane A2 synthase inhibitor, relieves acetylcholine-induced coronary spasm in patients with CSA. Although their study had no control arm, results showed that the drug might have some effect in patients with severe coronary spasm. However, detailed information about this drug is needed for future studies.
Summary and Conclusions
Regarding the treatment of coronary spasm, vasodilators such as long-acting CCBs and long-acting nitrates have been shown to be effective in most patients with CSA. However, some patients have medically refractory CSA. In general, endothelial dysfunction, hyper-reactivity of coronary smooth muscle cells, and other triggering factors, such as activation of the parasympathetic nervous system and ≈-adrenergic receptors, are involved in the pathogenesis of coronary spasm, and some drugs that can improve these abnormalities may be tried in such patients. With respect to the severe coronary spasm with haemodyamic instability that can occur during the spasm provocation test, drugs such as noradrenaline and adrenaline, which can increase systemic blood pressure to restore coronary blood flow and can dilate the coronary arteries, are effective. Coronary spasm plays a role in the pathogenesis of coronary artery disease, and cardiologists should have several options for medically refractory CSA or for severe coronary spasm with shock during the spasm provocation test.
Footnotes
Acknowledgement
We thank Yukihiro Fukuda, M.D., Keiji Matsuda, M.D., and Kentaro Ueda, M.D. of the Department of Medicine and Molecular Science, Graduate School of Biomedical Sciences, Hiroshima University, for their technical assistance, and Ms. Yuko Omura for her secretarial assistance.