
Abstract
Background
Pregnancy is a physiological process associated with an increased hemodynamic load and cardiac structural remodeling. Limited echocardiographic information exists on cardiac chambers, left ventricular (LV) systolic and diastolic functions, and LV mass during trimesters of normal pregnancy among African women.
Materials and Methods
Echocardiography was done at the beginning of the second trimester, beginning of the third trimester, and middle of the third trimester for 100 normal pregnant women and at one visit for age-matched 100 nonpregnant women. The data were analyzed using the Statistical Package for Social Sciences (SPSS) version 17 software. Analysis of variance was used to compare within trimesters, and a P value of <0.05 was considered significant.
Results
The mean (SD) ages of the patients and controls were 28.20 (±5.91) and 28.35 (±6.06) years, respectively (age range = 19-44 years, P = 0.86). Cardiac chambers, LV systolic function, and LV mass and its index increased significantly during pregnancy. A significant increase in A-wave velocity but slight increase in E-wave velocity and a reduction in tissue e′ velocity at the septal margin but a progressive increase in a′ velocity were also observed (P < 0.05).
Conclusion
Cardiac chamber dimensions, LV wall thickness, and mass, most indices of LV systolic and diastolic function, though within normal range, were significantly higher in pregnant than in nonpregnant Nigerian women.
Introduction
Pregnancy is a physiological state associated with a dramatic cardiac structural remodeling and an improved functional performance. 1 Cardiac adjustments to a pregnancy state may mimic abnormalities of the cardiovascular system.2–4 However, maternal cardiac disease occurs in 2% of all pregnancies, and this is the most important nonobstetric cause of maternal mortality. 5
The period of gestation can be divided into units consisting of three calendar months each or three trimesters, and “normal pregnancy” in obstetrics distinguishes pregnancies which are complicated. 6
Reports vary based on cardiac chambers' response to pregnancy. Mesa et al. 1 showed an increase in the left ventricular (LV) end-diastolic volume as early as 10 weeks gestation and a peak during the third trimester by echocardiography, whereas Geva et al. 7 did not observe any change in LV end-diastolic or end-systolic dimension throughout pregnancy. Other reports showed that left and right atrial and right ventricular diastolic dimensions increased throughout the gestational period.8,9
Variations exist in findings of cardiac systolic function during pregnancy. Cardiac output (CO) increased during normal pregnancy with the first increase noticed at as early as week 5 of gestation, reaching a peak at approximately the end of the second trimester according to some studies1,10 but late in the third trimester according to others 11 More recent studies showed no significant change in LV ejection fraction (LVEF) during pregnancy1,7 contrary to earlier report by Hunter and Robson 3 who found an increase in LVEF during the first two trimesters. A progressive decrease in LV fractional shortening (LVFS) was found by Schannwell et al. 8 , while Mesa et al. 1 and Clapp and Capeless 12 did not observe any change in LVFS during normal pregnancy further supporting the nonuniformity of cardiac response to normal pregnancy partly related to racial differences.
Cardiac diastolic function has been less studied than systolic function during pregnancy. The ratio of early-to-late diastolic flow velocity (E/A ratio) has been documented to be lower during the third trimester than at early trimesters and postpartum.8,9,13 However, very few studies in Nigeria have looked at the effects of pregnancy on the cardiovascular system.14–18
Hence the need for this study using two-dimensional, M-mode, and Doppler echocardiography for the assessment of changes in left and right ventricular dimensions (in systole and diastole), left and right atrial dimensions (in diastole), LV systolic and diastolic functions, and LV mass during trimesters of normal pregnancy.
Materials and Methods
The study was carried out at the Cardiac Care Unit of the Department of Medicine, Obafemi Awolowo University Teaching Hospitals' Complex (OAUTHC), Ile-Ife, Osun State. OAUTHC is a major tertiary referral center located in Osun State, Southwest geopolitical region of Nigeria.
A case-controlled study design was employed involving 100 normal pregnant women as subjects, each of whom carried a singleton fetus and 100 nonpregnant women as controls. Pregnant subjects were serially recruited at the early second trimester from the ante-natal clinic of the Department of Obstetrics, Gynaecology and Perinatology, OAUTHC, while the controls were age-matched apparently healthy nonpregnant volunteers from hospital employees, medical and nursing students, and members of the local community. They were confirmed nonpregnant by their last menstrual period and a urine pregnancy test. Inclusion criteria were female participants aged 18 years and above, and exclusion criteria were those with hypertension, diabetes, heart disease, fetal abnormality on ultrasonography, or any known systemic disease.
Each participant was interviewed with a structured questionnaire. All participants had clinical history, physical examination, and 12-lead electrocardiogram. Two-dimensional, M-mode, and Doppler echocardiography was done three times during their pregnancy, namely at the beginning of the second trimester (15 ± 1 weeks), beginning of the third trimester (28 ± 1 weeks), and middle of the third trimester (35 ± 1 weeks) and at one visit to Cardiac Care Unit for each control. At each visit, blood pressure was measured using an Accouson's mercury sphygmomanometer (Kris-Alloy) according to the recommendations of the British Hypertension Society. 19 Body weight was measured in kilograms using a weighing scale (Camry), and height was measured in centimeters using a stadiometer (ZT 120). Venous blood (2 mL) for packed cell volume was obtained from each participant following standard procedure. 20 Participants were taught how to collect a spot urine sample in a sterile universal bottle. Urinalysis was done using urinary dipstick, Combi-Uriscreen® 10SL to assess for protein, glucose, leucocytes, and nitrite in urine samples.
Transthoracic echocardiography was performed using the 5S probe for adults of GE Vivid 7 Pro ultrasound machine. The measurements were based on the recommendations of American Society of Echocardiography.21–24 Where applicable, measurements were indexed for body surface area, which was calculated with the Mosteller formula. 25 Tissue Doppler interrogation with the sample volume taken at the septal side of the mitral annulus to determine the tissue systolic velocity. There are no generally accepted reference values, but different cut-off points ranging from 5.4 to 7.8 cm/s have been used by various studies.26,27
LV diastolic function was assessed by determining early (E) and late (A) transmitral filling velocities as well as E/A ratio, deceleration time of the transmitral E velocity, and the isovolumic relaxation time. Using the pulsed wave tissue Doppler image, early (e′) and late (a′) diastolic mitral annular velocities were obtained from the septal side of the mitral annulus in the apical four chambers' view with septal annulus movement aligned with the sample volume line. The septal side was chosen, because in contrast to the lateral side, it moves in a direction more parallel to the ultrasound beam and is less affected by translational movement of the heart; thus, there is a narrow band of spectral velocity, and angle correlation is not needed. 28
Data Analysis
The data were analyzed using the SPSS version 17 software (SPSS Inc). Categorical variables were expressed as proportions (counts) and percentages, while continuous variables were expressed as mean ± standard deviation. Independent sample t-test was used to compare the age of pregnant and nonpregnant women. Comparison within trimesters (and with the healthy controls) was done using analysis of variance. Tukey's post hoc comparison test was then performed to ascertain which group was responsible for the significant difference in mean across the groups. In all the statistical tests, a value of P < 0.05 was considered significant.
Ethical clearance was obtained from the Ethics and Research Committee of our hospital. All participants gave written informed consent prior to enrollment in the study. The research was conducted in accordance with the principles of the Declaration of Helsinki.
Results
Demographic and clinical characteristics of the study participants
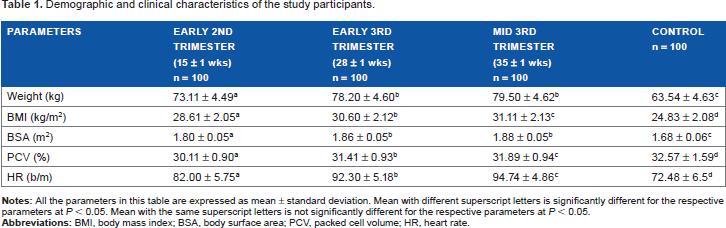
The demographic and clinical characteristics of the study participants are listed in Table 1. The mean (SD) ages of the subjects and controls were 28.2 (±5.9) and 28.4 (±6.1) years, P = 0.86, respectively (age range = 19-44 years). The subjects had statistically significant higher body weight, body mass index, and body surface area than the controls (P < 0.05, <0.05, and <0.05, respectively). The highest body weight, body mass index, and body surface area were attained at mid-third trimester (35 ± 1 weeks). The controls had significantly higher packed cell volume than the subjects (P < 0.05). The subjects had the least packed cell volume at early second trimester (15 ± 1 weeks). The subjects had significantly higher heart rate (HR) (P < 0.05). The highest HR was reached at mid-third trimester (35 ± 1 weeks). Urinalysis was similar in subjects and controls.
Demographic and clinical characteristics of the study participants.
Cardiac chamber dimensions in normal pregnant and healthy nonpregnant women
From Table 2, in diastole and systole, the subjects had significantly higher LV internal diameter (P < 0.05 and <0.05) and right ventricular internal diameter (RVD) (P < 0.05 and <0.05) than the controls. They also had significantly higher left atrial internal diameter (P < 0 .05) than the controls. Right atrial internal diameter in the subjects was higher than the controls only at the middle of the third trimester (P < 0.05). Right atrial internal diameter showed significant difference only between the early second trimester and the mid-third trimester (P < 0.05). LVDs and left atrial internal diameter showed no significant difference between the early third trimester and mid-third trimester (P > 0.05). RVD in diastole did not show significant difference within trimesters unlike RVD in systole that showed significant difference within trimesters except between the early third trimester and mid-third trimester (P < 0.05).
Cardiac chamber dimensions in normal pregnant and healthy nonpregnant women.

LV systolic function in normal pregnant and healthy nonpregnant women
From Table 3, SV and CO and their indexes and LVEF were significantly higher in subjects than in controls (P < 0.05), while LVFS was significantly lower in subjects than in controls (P < 0.05). The SV did not change significantly from the early third trimester. CO and its index and LVFS did not show significant difference between the early third trimester and mid-third trimester (P > 0.05). The highest LVEF was reached at mid-third trimester, and there was significant difference between controls and subjects and within trimesters (P < 0.05).
Left ventricular systolic function in normal pregnant and healthy nonpregnant women.

LV wall and mass in normal pregnant and healthy nonpregnant women
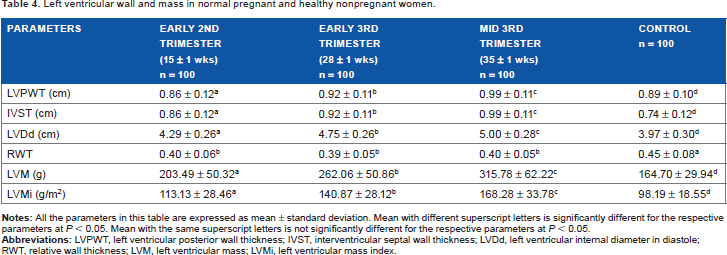
From Table 4, the LV posterior wall thickness, interventricular septal thickness, as well as LV mass and its index were significantly higher in subjects than in controls (P < 0.05, <0.05, <0.05, and <0.05, respectively). However, the relative wall thickness was lower in subjects (P < 0.05). LV internal diameter in diastole, interventricular septum thickness, LV mass, and its index were highest in the mid-third trimester (35 ± 1 weeks). Relative wall thickness showed significant difference between subjects and controls (P < 0.05) and not within trimesters.
Left ventricular wall and mass in normal pregnant and healthy nonpregnant women.
Doppler echocardiographic parameters in normal pregnant and healthy nonpregnant women
The conventional and tissue Doppler parameters of the study participants are shown in Table 5. There was a statistically significant increase in transmitral A wave velocity (P < 0.05) but slight increase in E wave velocity resulting in a significant decrease in the E/A ratio (P < 0.05) in subjects. The deceleration time (DT) of the early transmitral filling velocity and isovolumic relaxation time (IVRT) were significantly higher in subjects than in controls (P < 0.05 and <0.05, respectively). With increasing gestational age, there was a significant progressive fall in TD e1 velocity at the septal margin (P < 0.05), but the TD a1 velocity progressively increased (P < 0.05). Thus, the e1/a1 ratio decreased significantly at the septal margin as gestation increases (P < 0.05).
Doppler echocardiographic parameters in normal pregnant and healthy nonpregnant women.

Transmitral A velocity showed significant difference between controls and subjects and within the trimesters of pregnancy (P < 0.05). The E velocity did not show significant difference between the early third trimester and mid-third trimester (P 0.41). DT and IVRT showed significant difference between controls and subjects and within the trimesters of pregnancy (P < 0.05). TD e1 showed significant difference within trimesters of pregnancy (P < 0.05). TD a1 and e1/a1 also showed significant difference within trimesters except between the early third trimester and mid-third trimester (P > 0.05).
Discussion
The mean body weight of subjects increased across trimesters. Hematocrit trend was also similar to previous studies in Nigerians 29 and Caucasians.10,30 At 35 ± 1 weeks gestation, the HR had increased by 12.77%, from 82.00 ± 5.75 bpm at 15 ± 1 weeks to 94.74 ± 6.52 bpm, similar to other studies in Nigerians16,18 and in Caucasians. 10 The mean increase in HR among subjects was 17.20 bpm. This is within the range noted among Caucasians of 10-20 bpm.4,30
The subjects had significantly greater left and right atrial dimensions and LV and RV internal dimensions in systole and diastole. There was a progressive increase in these parameters across trimesters. These findings are similar to other studies2,8 The increase in cardiac chambers was due to structural remodeling as a compensatory mechanism for the chronic volume-overload state.1,2
SV, CO (and their indexes), and LVEF increased across trimesters. An increase in SV and CO was similar to the observation by Savu et al. 31 CO increased during pregnancy because of a higher SV in early pregnancy and a later increase in HR, whereas total vascular resistance decreased. 31 However, Savu et al. 31 did not find any significant change in LVEF. Furthermore, similar studies among Caucasians did not show any change in LVEF.1,12 This variation could be related partly to racial differences in systemic vascular resistance, especially in the black population.8,12,30,31 A progressive decrease in LVFS was noticed similar to Schannwell et al. 8 But Mesa et al. 1 and Clapp and Capeless 12 did not find any change in fractional shortening further supporting the nonuniformity of cardiac response to normal pregnancy partly related to racial differences.30,31
LV end-diastolic septal and posterior wall thickness and thus mass increased similar to other studies.8,9 This may be because of preload alterations. 32 Additionally, an increased myocardial contractility may provoke mild LVH. 32 Another mechanism is the neurohormonal response to pregnancy. Atrial natriuretic peptide and brain natriuretic peptide levels increase during the course of pregnancy. 33 Increased levels of atrial natriuretic peptide and brain natriuretic peptide may be related to changes in LV mass and LV volume. 33
The E velocity at 15 ± 1 weeks was significantly higher in subjects than in control similar to several studies.1,7–9 This is probably due to an increased preload as a result of an increased blood volume.34,35 Mabie et al. 36 in contrast did not find any change in E wave velocity at 8-11 weeks gestation or even at 36-39 weeks gestation. This may be because mitral inflow profile is affected by a complex interaction of many factors, including myocardial relaxation, ventricular compliance, pericardial restraint, preload and afterload, and myocardial contractility. 37
The A velocity progressively increased resulting in a decrease in the E/A ratio similar to previous studies.8,9,38 In the first trimester, the volume load occurs during the early diastolic phase, reflecting an increase in the E value; with the onset of the second trimester, and even more so the third trimester, atrial contraction becomes more important to LV filling. Alternatively, an increment in LV mass (wall thickness) may reduce ventricular compliance, necessitating more powerful atrial contraction. 1 DT of the E velocity and IVRT were significantly higher in subjects similar to other studies.9,38 IVRT, an active energy-dependent phase of the cardiac cycle, in the presence of physiologic cardiac hypertrophy is impaired and thus prolonged. 39
Peak tissue Doppler e1 velocity increased at the 15 ± 1 weeks (10.67 ± 1.65 cm/s) and subsequently declined to 8.60 ± 0.88 cm/s at 35 ± 1 weeks while peak tissue Doppler a1 velocity increased maximally at 35 ± 1 weeks (8.04 ± 0.92 cm/s) compared to 7.41 ± 1.12 cm/s at 15 ± 1 weeks. Comparatively, pregnant women at 28 ± 1 weeks had a significantly lower e1/a1 ratio (1.13 ± 0.07 vs 1.39 ± 0.10) which further decreased at 35 ± 1 weeks, reflecting the augmented a1 velocity, similar to findings by other investigators.1,9,36
Conclusion
Cardiac chamber dimensions, LV wall thickness, and mass, most indices of LV systolic and diastolic functions although within normal range, were significantly higher in pregnant Nigerian women than in the controls.
Author Contributions
Conceived and designed the experiments: VOA, MOB, RAA, POA, OOA. Analyzed the data: VOA, TOO, RAA, MOB, POA. Wrote the first draft of the manuscript: VOA, MOB, RAA, POA, OOA, TOO, AGA. Contributed to the writing of the manuscript: VOA, MOB, RAA, ONM, POA, EAA, SAO, AOA, EOA, AGA, TOO, OOA. Agree with manuscript results and conclusions: VOA, MOB, RAA, ONM, POA, EAA, SAO, AOA, EOA, AGA, TOO, OOA. Jointly developed the structure and arguments for the paper: VOA, RAA, MOB, OOA, POA, TOO, AGA. Made critical revisions and approved final version: VOA, MOB, RAA, ONM, POA, EAA, SAO, AOA, EOA, AGA, TOO, OOA. All authors reviewed and approved of the final manuscript.