
Abstract
Aim
To highlight the prevailing lack of suspicion of cardiac amyloidosis (CA) amongst physicians, leading to preventable delay in management of patients of heart failure (HF).
Methods
Six patients of CA diagnosed in 6 months were retrospectively analyzed. Clinical history, investigations, treatment, and follow-up data is analyzed.
Result
A speckled interventricular septum on echo favored CA. Speckle tracking showed reduced global longitudinal strain with typical left ventricular apical sparing in all patients. Bone marrow study confirmed light chain amyloidosis (AL) in all patients.
Conclusion
CA, a frequently missed diagnosis, can be detected early with the help of clinical red flag signs, echocardiogram, serum and urine immune electrophoresis and bone scan.
Introduction
Amyloidosis is caused by aggregation of misfolded insoluble fibril protein in various tissues and organs. Cardiovascular system involvement is a frequent cause of morbidity and mortality. 1 This disorder is highly underdiagnosed, especially in India due to want of clinical suspicion and insufficient data. This results in an unfortunate delay in its detection and management. Two clinically important forms of cardiac amyloidosis (CA) are immunoglobulin-derived light chain (AL) and transthyretin-derived (ATTR). There are only few reports of CA in Indian literature.2–4 Treatment regimens for AL and ATTR amyloidosis have advanced over the years with improvement in prognosis. However, the overall longevity of such patients remains unfortunate.
Material and Methods
Total 6 cases of CA who were hither to being serially managed as other ailments were diagnosed, treated, and followed up between October 2021 and April 2022. Retrospective analysis of records was done. The diagnosis of amyloidosis was based on clinical history and examination findings, electrocardiogram (ECG), cardiac biomarkers (N-terminal probrain natriuretic peptide [NT-proBNP]), measurement of serum immunoglobulin free light chain assay, and bone marrow examination. Detailed TTE including Doppler data and speckled tracking was available in all whereas cardiovascular magnetic resonance (CMR) (cases 3, 4, and 5) was performed in 3 of the patients.
Result
Clinical details of patients diagnosed with CA is described in Table 1, which showed predominance of male gender and age ranged from 54 to 72 years. Commonest presentation was signs and symptoms of heart failure (HF).
Clinical Details.
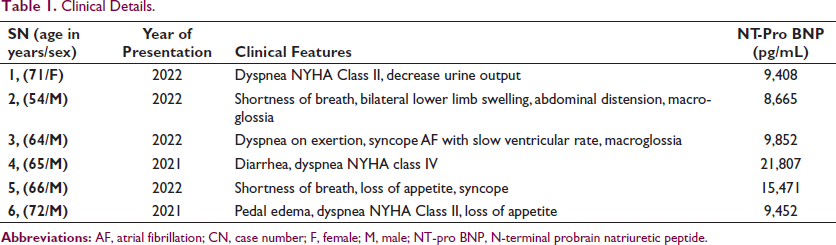
Two patients had history of syncope. Case 3 presented with atrial fibrillation with slow ventricular rate. Orthostatic hypotension was evident in case no. 3 and 5. Chest X-ray showed varying degree of cardiomegaly with signs of pulmonary venous and arterial hypertension. ECG showed repolarization changes, low voltage complex, and poor progression of “R” waves in precordial leads (pseudoinfarction pattern) in all. NT-pro BNP levels were elevated in all patients (Table 1).
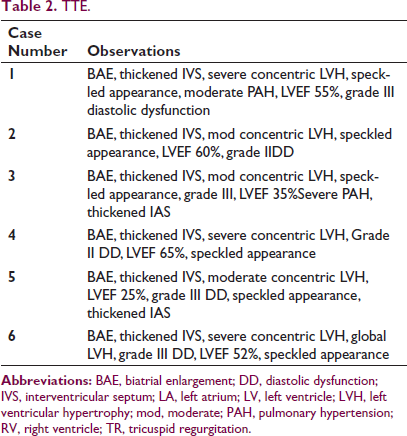
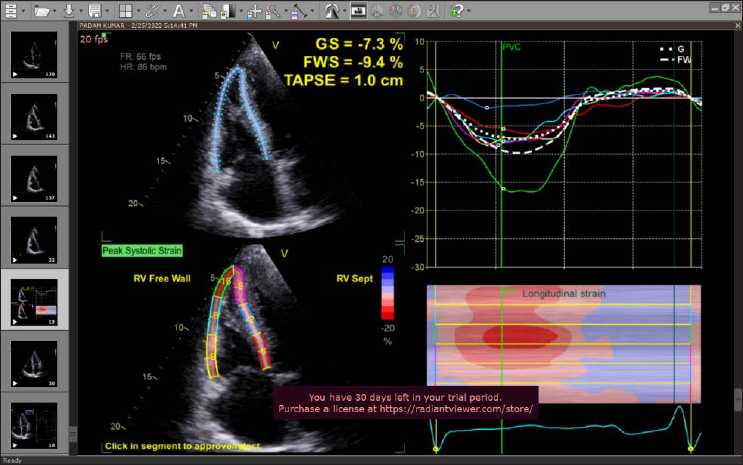
TTE details are enumerated in Table 2. Severe concentric left ventricular hypertrophy (LVH), diastolic dysfunction, sparkling appearance of myocardium, and preserved LV systolic function was present in all cases except case no. 3 and 5, who had reduced left ventricular ejection fraction (LVEF). Speckled tracking imaging in all our cases showed left ventricle apical sparing (“cherry on top” appearance) on polar graph and markedly abnormal global longitudinal strain (GLS) (Figure 1).
TTE.
Speckled Tracking Echocardiography Showing Typical LV Apical Sparing (Cherry on Top Appearance) and Markedly Reduced GLS.
Three patients underwent CMR which showed subendocardial late gadolinium enhancement (LGE). All patients underwent coronary angiography out of which case no 2, 3, and 4 had normal coronaries while the rest showed nonobstructive coronary artery disease.
Diuretics and other conservative measures were administered in all patients (Table 3). They were evaluated by a hematologist at our center. Bone marrow examination, serum, and urine electrophoresis were done. All patients were diagnosed as AL-type amyloidosis. Chemotherapy was received by only 3 patients.
Therapeutics and Outcome.
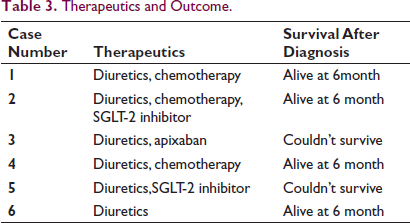
Out of total 6 patients, 2 patients succumbed within 6 months (average: 3.2 months) of diagnosis, among which 1 patient was on chemotherapy.
Discussion
Systemic amyloidosis is a multisystem disease that can present as an involvement of single organ to aggressive involvement leading to multiorgan failure. 5 The delay in diagnosis further adds to the poor prognosis. Early diagnosis can be done by identification of red flag signs that consist of clinical evidence of intolerance to heart failure (HF) medications because of symptomatic hypotension, neurological (sensorimotor polyneuropathy, paresthesia, and weakness), autonomic dysfunction (orthostatic hypotension, postprandial diarrhea alternating with constipation, gastroparesis, urinary retention, and incontinence), periorbital bruising, persistent mild elevation in serum troponin, and orthopedic complications (carpal tunnel syndrome, lumbar canal stenosis, spontaneous rupture of biceps tendon, knee, and hip arthroplasty). 6 Low QRS voltage on ECG and LVH on echocardiogram (ECG) is a characteristic feature. However, only 30% patients show the lack of low QRS voltage on ECG using commonly applied criteria. Low voltage is defined as less than 5 mm in the limb leads or less than10 mm in the precordial leads. However, these are nonspecific features and the absence of low voltage does not exclude CA as patients with CA to even meet ECG criteria for LVH. Hypertensive heart disease, hypertrophic cardiomyopathy (HCM), and amyloidosis having increased wall thickness on echo but low QRS voltage in ECG and LVH seen on TTE is a characteristic feature of amyloidosis. HCM patients usually having asymmetrical septal hypertrophy on echo and most of patients with hypertensive heart disease have concentric symmetrical LVH. Most commonly used ECG criteria to define LVH is Sokolow-Lyon voltage criteria SV1 + RV5 or RV6 ≥ 3.5 mV (35 mm) or RaVL ≥ 1.1 mV (11 mm). 7
All patients had marked elevation in NT-proBNP. A comprehensive TTE was performed. A thickened IAS and IVS > 12mm with speckled or granular appearance strongly favored CA in this study. 8 All patients had features of diastolic dysfunction on mitral inflow assessment. Speckle tracking showed good systolic function at the apex with basoapical gradient. The sensitivity of ApSpar_Ratio (apical sparing pattern ratio) for detecting CA is 58% in patients with AL type and 71% in patients with septal or posterior wall thickness ≥1.2 cm. 9 Increased LVEF/GLS and an apical-sparing pattern on polar graph is a valid tool for screening of patients at increased risk for CA. 10
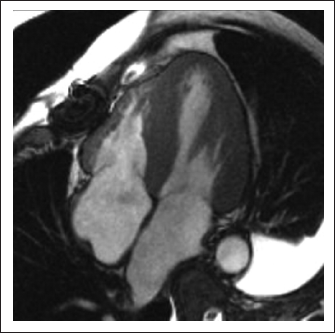
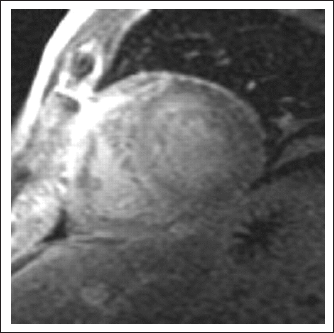
CMR with LGE identifies myocardial infiltration: following contrast administration classical pattern of subendocardial LGE along with abnormal blood pool and myocardial gadolinium kinetics (Figures 2 and 3). The disease can be assessed at 3 different stages using T1 mapping techniques—edema (native T1), myocyte response (intracellular volume), and infiltration (amyloid burden, ECV), providing prognostic markers. 11 CMR was performed in 3 cases. All patients had diffused subendocardial LGE within the myocardium.
CA Showing Diffused Myocardial Thickening and Mild Biatrial Enlargement.
Showing Widespread Late Gadolinium Enhancement.
In our study, all patients were diagnosed as AL type on serum and urine electrophoresis and bone marrow study. The combination of abnormal light chain on serum electrophoresis with a typical echo appearance is highly suggestive of AL amyloidosis. All patients with diagnosis of ATTR-CA should undergo tests for TTR gene mutations to differentiate wild type from hereditary (variant) forms.12, 13 Pyrophosphate scan (Tc-PYP) was not performed in any of our patients, however it is very sensitive and specific to diagnose ATTR-CM. A total of 10% cases of AL amyloid can have positive PYP scan (Figure 4). 13
PYP Scan Reporting.
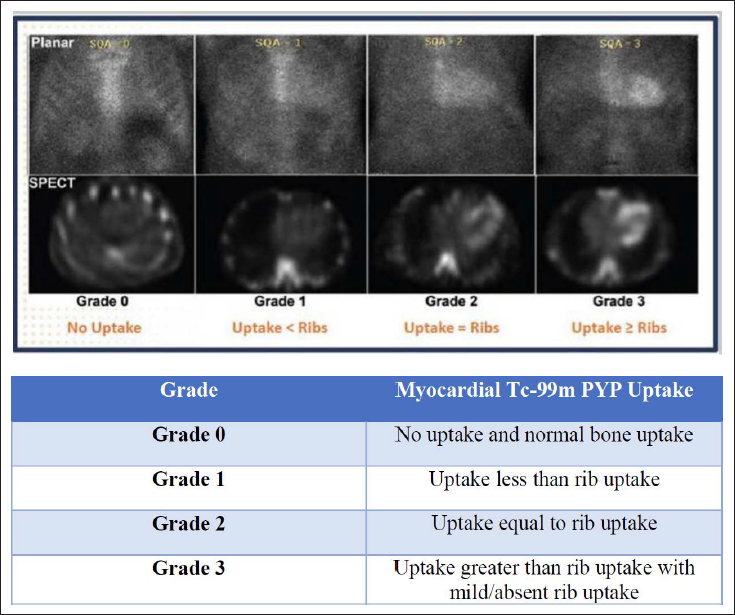
Quantitative myocardial to contralateral lung/rib uptake ratio at 1 h >1.5 indicates ATTR positive, 1-1.5 ATTR equivocal, and <1 ATTR negative. 3-h imaging is required when results are equivocal, as bone uptake increases at 3 h.13, 14
CA has a very poor prognosis and 2 patients expired within a short period of 6 months despite chemotherapy and HF medications. Their mortality could have been prevented by a timely diagnosis. Recent chemotherapy regimens using bortezomib, lenalidomide, and dexamethasone can cause remission and extend survival.2, 15
Standard HF therapy except diuretics may be even harmful due to hypotension and rhythm disorders. According to ESC statement, beta blockers, angiotensin-converting enzyme inhibitors, and angiotensin receptor blockers should not be used. Use of digoxin should be cautiously in patients of CA. 16 Patients with atrial fibrillation and CA have an increased risk of left atrial thrombus that is not adequately captured by the CHA2DS2-VASc score. ESC and AHA Society recommends that all patients of CA with history of atrial flutter and atrial fibrillation should receive anticoagulation.
Heart transplantation is an option to allow a strategy of autologous stem cell transplantation in patients with AL type. In patients with ATTR-CA, candidates for heart transplantation should not have significant extra cardiac disease. 13 Tafamidis is recommended regardless of NYHA functional class (ESC), 15 from NYHA functional class I-III (AHA). 12
Conclusion
Lack of suspicion and subsequent failure to recognize the red flags of CA play a big role in the unfortunate delay in its diagnosis and management, especially in a developing nation like India.
This case series may contribute toward creating awareness amongst physicians so that the tell-tale signs of CA are spotted early. Timely diagnosis of this otherwise progressively deteriorating disease will go a long way in reducing the associated morbidity and mortality. Early initiation of novice treatment options holds an exciting promise of favorably modifying this otherwise lethal condition.
Footnotes
Acknowledgements
The authors express their sincere gratitude to the Department of Cardiology, Sir Ganga Ram Hospital, New Delhi, India for their encouragement and motivation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed Consent
A written informed consent for patient information and images to be published have been obtained by the patient.