
Abstract
Background
Pulmonary hypertension (PH) is common in heart failure patients. Literature on PH in heart failure is sparse in Nigeria. This study was carried out to determine the prevalence of PH in heart failure patients and ascertain the relationship between left ventricular systolic and diastolic function and the degree of PH.
Methods
A total of 125 heart failure patients had echocardiography done. PH was diagnosed using tricuspid regurgitation jet and pulmonary ejection jet profile.
Results
PH was present in 70.4% of heart failure patients. Estimated mean pulmonary arterial pressure increased with increasing severity of systolic and diastolic dysfunction and had significantly negative correlation with ejection fraction, fractional shortening, and early mitral annular tissue diastolic velocity (E′), but positive correlation with left ventricular end-systolic volume, right ventricular dimension, transmitral E to A ratio, and E/E′ ratio.
Conclusion
PH is very common in heart failure and has significant relationship with left ventricular function.
Introduction
Heart failure according to the National Institute for Clinical Excellence is a complex clinical syndrome that can result from any structural or functional abnormality that impairs the ability of the heart to fill with or eject blood to support a physiological circulation. It commonly begins with the left heart and ultimately involves the right heart, giving a biventricular picture.
The overall prognosis in heart failure is poor, and the development of significant pulmonary hypertension (PH) is a predictor of all-cause death and cardiovascular mortality in heart failure, independent of other known variables.1–3
The World Health Organization classifies PH into five major categories (Venice 2003), and PH secondary to left heart disease falls in category two. 4
The hemodynamic definition of PH includes a resting mean pulmonary arterial pressure (MPAP) of more than 25 mm Hg, and/or a resting pulmonary vascular resistance (PVR) of more than 3 Wood units. 5
The underlying pathophysiology of PH in left heart disease is not fully understood and is likely to be multifactorial. 6
The initial cascade of events begins with increase in filling pressures in the left heart, which causes passive increase in backward pressures in the pulmonary veins with consequent increase in pulmonary capillary wedge pressure. This can result in acute pulmonary edema from alveolar capillary stress failure, which is a reversible phenomenon.7–9 Initially referred to as “reactive PH”, the early stage is usually responsive to measures designed to decrease filling pressures (diuresis and hemodynamic unloading). If left unchecked, the elevated left-sided filling pressure transitions into “fixed PH” characterized by pulmonary vascular remodeling, which in turn maintains the transpulmonary gradient in an effort to avoid pulmonary edema. 10
As pulmonary venous hypertension persists, the alveolocapillary membrane may undergo potentially irreversible remodeling characterized by excessive deposition of type IV collagen. 11 This results in pathological changes in the pulmonary veins and arteries, including muscularization of arterioles, medial hypertrophy, and neointima formation of the distal pulmonary arteries, leading to an increased transpulmonary gradient and PVR. 12 These structural changes in pre- and postcapillary vasculature result in PH not generally responsive to efforts targeted at reducing left ventricular (LV) filling pressure alone. 10
There is evidence in small cohorts from research done in Caucasians, which suggest that therapies aimed at pulmonary vasodilatation may be fruitful in patients with advanced heart failure.13,14
Evolving clinical trial evidence to date strongly supports a role for chronic PDE5 inhibition in selected patients with PH and LV systolic dysfunction. 15
In contrast to the advances in treatment, which have occurred in recent years for idiopathic pulmonary arterial hypertension, only little progress has been made for category II PH, and most guidelines give little advice, other than to manage systemic hypertension and volume status and to optimize underlying conditions. 6
In Nigerian population, there is very sparse literature on PH in heart failure patients, which should serve as a basis for conducting our own research with regard to developing newer trends in the management of this group of patients.
Objective
This study was carried out to determine the prevalence of PH in heart failure patients and ascertain the relationship between LV systolic and diastolic function and the degree of PH (or estimated pulmonary arterial pressures).
Methodology
Over an 18-month period from January 2012 to July 2013, 125 patients with heart failure diagnosed clinically using the Framingham criteria 16 were consecutively recruited into the study. Relevant clinical and demographic data were obtained, and they had echocardiography done using GE Vivid 7 (USA) cardiac ultrasound machine. Echocardiographic measurements were made using the recommendations of the American Society of Echocardiography and involved taking an average of three consecutive cardiac cycles. Araoye point-score system 17 was used in distinguishing hypertensive cardiomyopathy from idiopathic dilated cardiomyopathy. PH was diagnosed by echocardiography on finding a right ventricular acceleration time (AT) less than 100 ms with a right ventricular acceleration to ejection time ratio <0.30 from the pulmonary ejection jet profile.18–20 MPAP was estimated using the regression equation developed by Dabestani et al. 20 : MPAP = 90 - (0.62 x AT). LV systolic function was determined by deriving the left ventricular ejection fraction (LVEF) and fractional shortening from 2D-guided M-mode echocardiography. LV systolic dysfunction was defined by ejection fraction (EF) less than 55% and was further categorized into mild (EF between 45% and 54%), moderate (EF between 30% and 44%), and severe systolic dysfunction (EF < 30%). 21 LV diastolic function was determined from conventional and tissue Doppler echo by deriving the transmitral early to late inflow velocity ratio (E/A), and ratio of transmitral early filling velocity to early mitral annular septal tissue velocity (E/e′). It was graded into grade 1 (E/A ratio <1), grade 2 (E/A ratio between 1 and 2 with e′ < 10 cm/s), and grade 3 (E/A of ≥ 2 with e′ <8 cm/s).22,23 The heart failure with preserved ejection fraction (HFpEF) was defined using the latest recommendations of the European Society of Cardiology and American Heart Association24,25: clinical signs and/or symptoms of Heart failure (HF), normal or mild reduction of systolic with LVEF >50%, and evidence of reduced diastolic LV function. Heart failure with reduced ejection fraction (HFrEF) is defined as the clinical diagnosis of HF and EF ≤40%, 24 while patients with an EF in the range of 40%-50% represent an intermediate group. 24
Data were entered into the Statistical Package for the Social Sciences (SPSS) 17.0 computer software. Continuous variables were expressed as mean and standard deviation, chi-square analysis was used to express associations between categorical variables. Independent t-test and analysis of variance were used to express relationship between two or more groups of continuous variables, respectively. Pearson correlation coefficient was used to express relationship between continuous variables. Results were presented in tables and charts. Statistical significance was defined as P-value ≤0.05.
Ethical clearance was obtained for the study from OAUTHC Ethics and Research Committee. The research was conducted in accordance with the principles of the Declaration of Helsinki. Patients gave their written, informed consent to participate in the research.
Results
The study sample comprised 125 patients of whom 64 were males with 68.8% of them having pulmonary hypertension (PH) and 61 were females with 72% of them with PH. The clinical and demographic data of the study sample and the mean and standard deviation of each parameter between patients with and without PH are presented in Table 1. There was no statistical difference in the demographic parameter such as the mean age, sex, height, weight, body surface area (BSA), body mass index, and diastolic blood pressure between the two groups. On comparing the proportion of patients with PH in subjects with HFrEF and those with HFpEF, of 100 patients with HFrEF, 73 (73%) had PH, while, of 25 with HFpEF, 15 (60%) had PH. There is no significant difference in the proportion of heart failure patients with PH between both groups (χ2 = 1.62; P = 0.203). Hypertensive heart disease (HHD) was the most common etiology of heart failure accounting for 65% of heart failure cases, followed by dilated cardiomyopathy and majority of them have PH as shown in Table 1. Also, no statistical difference was observed on comparing the proportion of HF with PH and those without PH on medication such as angiotensin-converting enzyme inhibitor/angiotensin receptor blocker (ACEI/ARB), digoxin, spironolactone, furosemide, and beta-blocker.
Clinical and demographic data of the study population.

P-value between PTH in HFpEF and HFrEF (P = 0.203).
Table 2 shows the range, mean, and standard deviation of the LV echocardiographic parameters. The LV internal diameter in diastole ranged from 3.20 to 8.50 cm with a mean of 5.96 ± 1.23 cm. The LV mass index ranged from 47.69 to 379.37 g/m2 with a mean value of 147.60 ± 63.31 g/m2. The EF ranged from 11% to 88% with a mean value of 40.94% ± 16.53%.
Left ventricular echocardiographic findings of the study population.

The pulmonary flow Doppler parameters and right ventricular dimension are represented in Table 2. The right ventricular AT ranged from 22 to 133 ms with a mean value of 71.64 ± 21.78 ms. The estimated mean pulmonary artery pressure ranged from 7.54 to 76.36 mmHg with a mean value of 45.58 ± 13.50 mmHg.
Distribution of heart failure patients according to severity of systolic dysfunction is shown in Figure 1. Systolic dysfunction as represented by low EF, when further categorized according to severity, showed that 19 patients (15.2%) had mild systolic dysfunction, 49 (39.2%) had moderate systolic dysfunction, and 32 (25.6%) had severe systolic dysfunction.

Distribution of heart failure patients according to severity of systolic dysfunction.
All heart failure patients had diastolic dysfunction, and this was categorized into three grades (1-3) according to severity. Grade 1 diastolic dysfunction (impaired relaxation) was present in 38 patients (30.4%) and grade 2 (pseudonormal) diastolic dysfunction in 20 patients (16.0%), while 67 (53.6%) of the heart failure patients had grade 3 (restrictive) diastolic dysfunction as shown in Figure 2.

Distribution of heart failure patients according to grade of diastolic dysfunction.
Echocardiographic parameters were compared between heart failure patients with PH and those without, and findings are as shown in Table 3. There was no significant difference in the echocardiographic findings between both groups (P > 0.05).
Echocardiographic parameters of pulmonary hypertensive vs nonpulmonary hypertensive heart failure patients.

The analysis of variance of estimated MPAP across the grades of systolic function shows significant variation (P 0.045). The estimated MPAP varies with increasing severity of systolic dysfunction and is presented graphically in Figure 3.
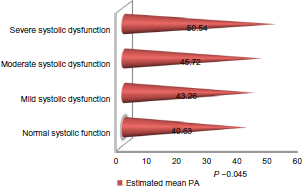
Graphical representation showing the mean values of estimated MPAP across the grades of severity of systolic dysfunction.
Likewise, the estimated MPAP varies across the grades of diastolic dysfunction (P 0.022). The MPAP increases with increasing severity of diastolic dysfunction from grade 1 to grade 3 and is presented graphically in Figure 4.

Graphical representation showing the mean values of estimated MPAP across the grades of severity of diastolic dysfunction.
Significant correlates of estimated MPAP
The estimated MPAP had a significant negative correlation with the EF (r = −0.248; P = 0.006), fractional shortening (r = −0.258; P = 0.004), and early mitral annular tissue diastolic velocity (r = −0.252; P = 0.006), while it had a significant positive correlation with LV end-systolic volume index (r = 0.182; P = 0.047), right ventricular diameter (r = 0.189; P = 0.049), ratio of transmitral early to late filling velocity (r = 0.228; P = 0.016), and the ratio of transmitral early filling velocity to early mitral tissue annular diastolic velocity, a surrogate marker for LV end-diastolic pressure (r = 0.241; P = 0.010), although they have relatively weak correlation coefficients, as shown in Table 4 and Figure 5.

Scatter plot depicting the correlation between estimated MPAP and LVEF.
Significant correlates of estimated MPAP.

Discussion
Our results showed that the prevalence of PH in heart failure patients attending our institution is 70.4%. Some studies in Caucasian heart failure populations have comparable prevalence. Butler et al. 26 found that a prevalence of 72% enrolled into an academic program. Costard-Jackle and Fowler 27 identified PH in 79% of patients with advanced heart failure who were referred for consideration for cardiac transplant. In a community-based study involving 1,049 heart failure patients, Bursi et al. 1 found PH in 79% of patients.
Though the gold standard for diagnosis of PH is right heart catheterization, Doppler echocardiography has proven useful as the optimal screening tool for assessment of PH. 28
This study found no statistically significant difference in the prevalence of PH in heart failure with reduced and preserved EF, even though this was higher in heart failure with reduced EF (73% vs 60%). The equally high prevalence of PH found in patients with HFpEF is comparable to that obtained in the study by Leung et al. 29 , who reported a prevalence of 53%. Lam et al. 30 found a higher prevalence of 83% in HFpEF. This higher value may be due to the fact that it was a community-based study in contrast to our hospital-based study.
Morbidity and mortality in HFpEF are similar to values observed in patients with HFrEF, yet no effective treatment has been identified. While early research focused on the importance of diastolic dysfunction in the pathophysiology of HFpEF, recent studies have revealed that multiple nondiastolic abnormalities in cardiovascular function also contribute. 31 An extensive overview of all HFpEF trials performed so far 32 showed evidence of diverging efficacy of comparable pharmacological agents in HFrEF and HFpEF for ACEIs, ARBs, betablockers, and statins.33–35 With similar prevalence of PH in HFrEF and HFpEF, understanding the pathophysiological mechanisms underlying PH may lead to breakthrough on possible pharmacological agents to reduce mortality and morbidity in HF.
The similarly high prevalence of PH in both forms of heart failure is also likely accounted for by diastolic dysfunction, which has been reported to be a strong independent predictor of the development of PH and a common denominator in both forms of heart failure, irrespective of systolic function. The concomitant systolic dysfunction in HFrEF possibly serves to augment the degree of PH already present. Our study found increasing mean values of MPAP with increasing severity of systolic dysfunction to buttress this point. We also observed that the MPAP correlated inversely with LVEF and positively with end-systolic volume index. Similar findings were noted by Enriquez-Sarano et al. 36 , who demonstrated that the degree of PH as represented by systolic pulmonary arterial pressure correlated with EF (r = −0.23, P = 0.02) and end-systolic volume index (r = 0.20, P = 0.04). However, these parameters were not noted to be independent predictors of pulmonary pressures.
We found a significant correlation between the severities of diastolic dysfunction parameters and estimated MPAP. This is similar to findings in other studies and is in consonance with the pathophysiologic process, leading to PH earlier described.36,37 Neuman et al. 37 demonstrated an association between the severity and grade of diastolic dysfunction and estimated pulmonary arterial pressure after analyzing 477 consecutive echocardiographic studies in subjects with HFpEF. Enriquez-Sarano et al. 36 found a significant inverse correlation between systolic pulmonary arterial pressure and mitral valve deceleration time in heart failure patients.
Our study found no significant difference in the echocardiographic parameters measured between pulmonary hypertensive and nonpulmonary hypertensive heart failure patients. This may be because the cardiac structural and/or functional changes are a fundamental occurrence in heart failure, irrespective of the development of PH or not. The time course and extent of pathological changes observed in PH secondary to left heart disease may be variable according to individual patients and are likely linked to constitutional factors. 6 The sample size used in this study may partly contribute to these findings.
The role of genetic polymorphisms in determining susceptibility to the development of PH secondary to left heart disease has not received much attention. Genetically determined predisposition to neurohormonal aberrations might be responsible for the emergence of PH in some patients with left heart disease and not in others in a manner similar to that observed in the Pulmonary arterial hypertension (PAH) literature of “multiple hit” theory. 38 Once PH is manifest, there is a secondary response of the effect of this pathology on the right ventricle, which is also clinically variable in phenotypic expression. 39
Lam et al. 30 showed that patients with systemic hypertension and heart failure had higher systolic pulmonary arterial pressure than those with systemic hypertension but without heart failure, despite similar pulmonary capillary wedge pressures providing evidence that heart failure may influence elevation of pulmonary artery pressure.
Vasoconstrictor endothelin-1 (ET-1) has been reported to be in high concentration in heart failure 40 and is due to the imbalance from endothelial dysregulation, which had been incited by the exposure of the pulmonary endothelium to the high back-pressures transmitted from the chronically elevated LV end-diastolic pressure. 41
ET-1 concentration has a strong positive correlation with New York Heart Association (NYHA) class and a strong inverse relationship with LVEF and cardiac index. 42 This is also supportive of the finding of the relationship between EF and MPAP found in our study.
Despite evidence for the expression of ET-1 excess in both WHO category 1 and 2 PH, the outcome of targeting that aberration through the use of endothelin antagonists is quite dissimilar, with a marked benefit for category 1, but notable worsening in the context of left heart disease. 43
Conversely, emerging evidence now suggest therapeutic modulation of the nitric oxide pathway with the use of phosphodiesterase-5 inhibitors (PDE5I) in the two distinct PAH categories. 44 PDE5I increase cGMP levels by blocking their catabolism. PDE5I attenuate adrenergic stimulation, 45 reduce ventricular–vascular stiffening, 46 antagonize maladaptive chamber remodeling, 47 improve endothelial function, 48 reduce PVR, 43 and may enhance renal responsiveness to natriuretic peptides, 49 suggesting that this agent may be beneficial in HFpEF and PH. 31
Trials of pulmonary vasodilators may also identify a subset of heart failure patients who may benefit from them as a bridge to heart transplant to prevent fixed irreversible elevation in PVR, which precludes heart transplant.50,51
Conclusion
PH is very common in our heart failure patients, accounting for a prevalence of 70.4%, and this high prevalence cuts across heart failure with both low and normal EF. LV diastolic and systolic dysfunction contributes to its presence and severity. Knowledge of this high burden and effect of PH in our heart failure patients serves as a basis for conducting therapeutic trials targeted at PH secondary to heart failure in our environment. Longitudinal studies are recommended to assess the effect of PH on the outcome of our heart failure patients.
Author Contributions
Conceived and designed the experiments: VNA, OEA, OJB, MOB. Analyzed the data: VNA, OEA, OJB, OOA. Wrote the first draft of the manuscript: VNA. Contributed to the writing of the manuscript: VNA, OEA, AOA, OOA, OJB, MOB. Agreed with manuscript results and conclusions: VNA, OEA, AOA, OOA, OJB, MOB. Jointly developed the structure and arguments for the paper: VNA, OEA, AOA, OOA, OJB, MOB. Made critical revisions and approved the final version: VNA, OEA, AOA, OOA, OJB, MOB. All the authors reviewed and approved the final manuscript.