
Abstract
We report an interesting case of a man with a persistent left superior vena cava (PLSVC) with left azygos vein who underwent electrophysiological evaluation. Further evaluation revealed congenital dilated azygos vein, while a segment connecting the inferior vena cava (IVC) to the hepatic vein and right atrium was missing. The azygos vein drained into the superior vena cava, and the hepatic veins drained directly into the right atrium. The patient did not have congenital anomalies of the remaining thoracoabdominal vasculature.
Anomalies of the systemic veins are not uncommon, with a persistent left superior vena cava (PLSVC), absent right superior vena cava, and an interrupted inferior vena cava (IVC) being most frequent.1,2 PLSVC is the most common and important congenital malformation of the thoracic venous system, affecting about 0.3%-0.5% of the general population. 1 Nearly half of the patients with isolated PLSVC have other cardiac malformations, such as atrial septal defect, endocardial cushion defect, and tetralogy of Fallot. 2 The classification of PLSVC was based on the defect in the embryology development and anastomotic ramus between superior vena cava and the azygos venous system. 1 The common cardinal vein serves as the major venous drainage of the embryo, with the anterior cardinal vein carrying blood from the cephalic part of the embryo and the posterior cardinal vein carrying blood from the caudal part of the embryo.2,3 The distal part of the left cardinal vein then degenerates and the proximal portion connects to the right anterior cardinal vein, forming the superior vena cava. The left posterior cardinal vein degenerates with the formation of ligament of Marshall, a process completed around the eighth week of embryo life. The failure of the left posterior cardinal vein to degenerate results in a PLSVC state, even in association with a left azygos vein on some occasions.2,3
We share an interesting case of a man who presented with syncope. He underwent electrophysiological evaluation, and it was incidentally found that he has a constellation of PLSVC with left azygos vein and no other cardiac abnormalities.
Case Report
A 24-year-old man presented with multiple episodes of syncope. He was found to have electrocardiographic evidence of AV Block I° and AV Block II° in the follow-up, and the echocardiographic evaluation has shown no other cardiac abnormalities. Due to recurrent symptomatic bradycardia with AV Block I° and AV Block II°, he was referred for an electrophysiological evaluation. The left femoral vein was accessed with a 7-French triport sheath through which three quadripolar pacing electrode catheters were introduced in an attempt to reach the right atrium, right ventricular apex, and atrioventricular junction. However, access to the right ventricle was not possible. The catheter was observed to advance parallel to the spine, past the contour of the heart, and to return back into what seemed to be the superior vena cava. Iodinated contrast material was injected in order to obtain a venogram (Fig. 1). It was observed that the contrast material did not pass to the right atrium, which suggested an anomaly of the IVC.
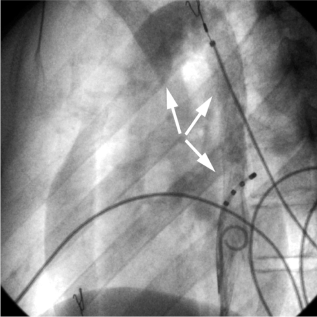
Venogram obtained during the first attempt in an electrophysiological study. The contrast agent passes into the dilated azygos vein (distal arrows) and PLSVC (proximal arrow).
Magnetic resonance (MR) angiography of the thorax and abdomen was performed for further evaluation of congenital cardiac and vascular defects (Fig. 2). Venous return from the inferior body regions drained into the dilated azygos vein, while a segment connecting the IVC to the hepatic vein and right atrium was missing. The azygos vein drained into the superior vena cava, and the hepatic veins drained directly into the right atrium. No other cardiovascular abnormalities were found.

MR angiography shows a dilated azygos vein (
In a second setting, with background knowledge of the anomalous venous return, an electrophysiological study was successfully performed via a right femoral access, passing the catheter through the azygos vein and superior vena cava (Fig. 3).

The EP catheters went advance through the azygos vein (distal) and superior vena cava (proximal) to complete the electrophysiological study.
Programmed atrial stimulation showed a dual AV node physiology with typical AV reentrant tachycardia configuration. However, radiofrequency ablation was not successful. The patient was discharged home on metoprolol with no symptoms of palpitations.
Aplasia of the IVC is a rare anomaly that is present in approximately 0.6% of the population.4,5 It usually presents through thrombosis of the lower extremities.4,5 We report a case of an adult patient with IVC interruption and azygos continuation, in whom any symptoms or signs of complications of this anomaly were absent. The anomaly initially prevented invasive electrophysiological evaluation from a femoral access.
Author Contributions
Conceived and designed the experiments: All authors. Analyzed the data: MSP, AE. Wrote the first draft of the manuscript: MSP, AE. Contributed to the writing of the manuscript: All authors. Agree with manuscript results and conclusions: All authors. Jointly developed the structure and arguments for the paper: MSP, AE. Made critical revisions and approved final version: All authors. All authors reviewed and approved of the final manuscript.