
Abstract
Left ventricular diastolic dysfunction (LVDD) is one of the earliest signs for abnormal cardiac function in patients with type 2 diabetes (T2DM). It is important to explore the risk factors that will assist in identifying the severity of the LVDD in this population. We examined the influences of fitness and fatness on the level of left ventricular (LV) impairment in patients with T2DM. Twenty-five patients (age: 64.0 ± 2.5 years, body mass index [BMI] = 36.0 ± 1.5 kg/m2, mean ± standard error of measurement) with T2DM and preserved systolic function, but impaired diastolic function, mitral valve (MV) E/e′, participated in the study. LV function was assessed using a stress echocardiograph, aerobic power was assessed with a sign- and symptom-limited graded exercise test, and the fatness level was assessed using Dual-energy X-ray absorptiometry and BMI. Patients in the higher 50% of BMI had higher lateral and septal MV E/e′ (~34% and ~25%, respectively, both P < 0.001), compared to those in the lower 50% of BMI, with no difference in LV ejection fraction (LVEF) (P > 0.05). In addition, a higher BMI correlated with a higher lateral (r = 0.62, P < 0.001) and septal (r = 0.56, P < 0.01) E/é. There was no such relationship for VO2peak. BMI and VO2peak were not correlated with LV systolic function (ejection fraction). In individuals with T2DM and diastolic dysfunction, a higher BMI was associated with worsening diastolic function independent of their aerobic capacity. The data provide a simple and practical approach for clinicians to assist in the early identification and diagnostics of functional changes in the heart diastolic function in this population.
Introduction
Cardiovascular disease (CVD) is the leading cause for morbidity and mortality in patients with type 2 diabetes (T2DM). Subclinical left ventricular diastolic dysfunction (LVDD) is an early indicator of abnormal myocardial function in this population. 1 In fact, the prevalence of LVDD in those with T2DM is between 65% and 75% in women and 35% and 45% in men. 2 Furthermore, up to 75% of those with LVDD have preserved left ventricular (LV) systolic function as measured by LV ejection fraction (LVEF).3,4
Although early screening for LVDD is considered important in T2DM management, it can be expensive, requires advanced technology, needs staff expertise, and is time consuming. Thus, predictors that are practical and simple to measure need to be identified. Currently, there are several conditions that may predict LVDD, including chronic obstructive pulmonary disease (COPD), hypertension, ischemic heart disease, diabetes, obesity, and systolic dysfunction, independent of age and sex.5–8 However, to date, little is known about their relationship to the severity of the LVDD in patients with T2DM who were already experiencing reduced diastolic function.
Obesity, reduced physical activity, and reduced exercise capacity are risk factors for both T2DM and CVD.9,10
Additionally, patients with T2DM are characterized by a reduced aerobic capacity (VO2peak) compared to nondiabetics,1,11 which is correlated with a higher risk of cardiovascular and all-cause mortality observed in this group. 1 In contrast, increased physical activity in patients with T2DM and CVD may improve myocardial function, glycemic control, and cardiorespiratory fitness and perhaps ultimately contribute to reduce the risk of morbidity and premature mortality.9,12 Interestingly, the associations between fitness and fatness with LVDD severity in patients with T2DM who have established LVDD, but preserved systolic function, are not clear but may be clinically significant as it may not be practically possible to screen all patients for LVDD. In addition, it may be used as a simple and low-cost tool to predict the severity of LVDD in this population. As such, the main purpose of this study was to examine whether fitness and fatness are related to the severity of LVDD in patients with T2DM having established isolated diastolic dysfunction (ie, preserved systolic function). We hypothesized that patients with higher body mass index (BMI) and lower fitness levels would have poorer LV diastolic function.
Methods
Twenty-five (male/female [M/F] = 12/13) patients (age: 64.0 ± 2.5 years, BMI = 36.0 ± 1.5 kg/m2, mean ± standard error of measurement [SEM]) with T2DM (fasting glucose = 9.4 ± 0.7 mmol/L) participated in this study (Table 1). Patients were recruited from Austin Health (Hospital), Melbourne, Australia, over a period of two years. Patients with established diagnosis of T2DM requiring pharmacological therapy were included if their medications were not modified in the past three months (ie, clinically stable state) and had impaired diastolic function at peak exercise as assessed on stress echocardiography. Impaired diastolic dysfunction was defined as an early velocity of MV septal annulus (e′) <8 cm/seconds and either a deceleration time (DT) >220 ms or E/e′ >10.13–15 Exclusion criteria included history of lung disease requiring regular inhaler use, LVEF <45%, uncontrolled diabetes (hemoglobin A1c [HbA1c] >9.0%), occult coronary artery disease, or evidence of myocardial ischemia on stress echocardiography.
Group characteristics.

Each participant received written and verbal explanations about the nature of the study before signing an informed consent. The study protocol was approved (H2010-03936) by the Human Research Ethics Committees of both Austin Health and Victoria University, Melbourne.
The study protocol has been previously described in detail. 15 Participants underwent a signs- and symptoms-limited graded exercise stress test for cardiac and aerobic power assessments, dual-energy X-ray absorptiometry (DXA) scanning for the assessment of body composition, and a fasting blood test for the assessment glucose and lipid concentrations. Our study was approved by Austin Health, Human Research Ethics Committee, approval number H2010/03936 which complied with the Declaration of Helsinki.
Stress Echocardiography
All eligible participants had an evaluation of diastolic function with echocardiography imaging while in stable state. Exercise stress echocardiography was performed using a symptom-limited graded exercise on a Cybex MET 100 cycle (Cybex Metabolic Systems). Images of the left ventricle in motion and hemodynamic measures were recorded immediately after exercise. The following measures were assessed: MV DT (m/second), MV early wave for mitral inflow (MV E, m/second), MV ratio of E and A waves of mitral inflow (MV E/A), MV early diastolic annular velocity (e′) lateral (m/second), MV e′ septal (m/second), MV E/e′ (lateral), and MV E/e′ (septal), where E/e′ = ratio of E and e′, which is a noninvasive estimate of LV filling pressure.16,17 Septal refers to measurements at the septal MV annulus; lateral refers to measurements at the lateral annulus. LVEF is expressed as percentage and was assessed before exercise.
Aerobic Power
Aerobic power (VO2peak) was assessed during the same sign- and symptom-limited graded exercise test performed for stress echocardiography, which was started after a five-minute period of rest. The protocol included an initial intensity of 25 W and increased to 40 W after 1 minute, followed by increments of 20 W/minute for males and 10 W/minute for females. The test was terminated when a participant's rating of perceived exertion reached very hard (Borg scale = 17). Expired respiratory gases were collected through a breath-by-breath (BxB) pneumotach system connected to gas analyzers. The BxB data were integrated for each 15 seconds interval. The gas analyzer was calibrated immediately before each test using gases that had been calibrated at alpha standard. Heart rate was measured at rest and during the incremental test by 12-lead electrocardiography (Mortara, X-Scribe II). Participants had been asked not to consume caffeine or alcohol for a minimum of 2 hours prior to exercise test.
Body Composition
DXA (GE Lunar Pxodigy, Software version 9.1) was used to assess total body fat percentages as described previously.18,19 All DXA measurements were performed at the Bone Density Unit, Austin Health. BMI was measured by mass (kg) divided by height squared.
A fasting blood sample
A blood sample was collected following overnight fast. Blood was analyzed for HbA1c (%), fasting blood glucose (mmol/L), high-density lipoprotein (HDL, mmol/L), total cholesterol (mmol/L), low-density lipoprotein (mmol/L), and triglycerides (mmol/L) at Austin Health as described previously.18,19
Statistical Analysis
Due to the cross-sectional nature of the study, patients' characteristics were stratified as being in the higher or lower 50% of BMI, VO2peak, and LVDD (E/e′), and an unpaired t-test was used to compare between groups (ie, high vs low for each respective comparison). A Spearman's rho correlation was used to assess the correlation between BMI and VO2peak with LV parameters. Data are reported as mean ± SEM, and all statistical analyses were conducted at the 95% level of significance.
Results
Stratified patients' characteristics are summarized in Table 2. There were no significant differences in age, HbA1c, and lipid profiles between groups (all P > 0.05) with the exception of HDL that was lower in patients with higher BMI. BMI was correlated with total body fat (kg; r = 0.94, P < 0.001) and total fat percentage (%; r = 0.69, P = 0.01).
Characteristics of patients stratified as higher 50% or lower 50% of the cohort.
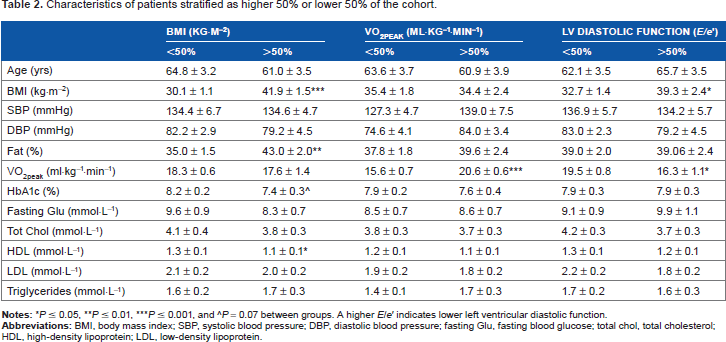
P ≤ 0.05
P ≤ 0.01
P ≤ 0.001, and ^P = 0.07 between groups. A higher E/e′ indicates lower left ventricular diastolic function.
Patients with higher BMI had higher degree of diastolic dysfunction. Lateral and septal E/e′ were higher in the higher 50% of BMI (by ~34% and ~25%, respectively, both P < 0.001), compared to those in the lower 50% of BMI (Table 3). BMI significantly correlated with lateral (r = 0.62, P < 0.001) and septal (r = 0.56, P < 0.01) E/é.
LV measures stratified as higher and lower 50% for BMI and VO2peak.

P ≤ 0.05
P ≤ 0.01
P ≤ 0.001, and ^P = 0.07 between groups.
No significant difference in measures of systolic function, LVEF, was observed between those in higher and lower 50% of BMI (Table 3).
Diastolic dysfunction was not different between those in the higher 50% of aerobic power compared to those in the lower 50% (Table 3), despite a significant difference in VO2peak between the groups (20.6 ± 0.6 vs 15.6 ± 0.7, P < 0.001; Table 2). LVEF tended to be higher (~5%, P = 0.07) in those with higher aerobic power (Table 3). Aerobic power was not correlated with both diastolic and systolic measures.
Discussion
Patients with T2DM and echocardiographic evidence of LVDD exhibited higher LV filling pressure as estimated by E/e′ (both lateral and septal) if they were in the higher 50% for BMI. Similar relationships were not evident for those in the lower 50% of VO2peak.
It is previously reported that there is a link between metabolic control of blood glucose (normal blood glucose, impaired fasting glucose, and T2DM) and LV structure and function.4,20–24 In fact, the degree of LVDD appears to increase with the duration of T2DM (>4 years post-diagnosis) and more severe impaired glucose metabolism.20,25 In addition, LVDD is often present in those with impaired glucose tolerance, despite a lack of outward symptoms. 4 Given that it is not always feasible to screen all patients for LVDD, it is important to identify related, low cost, and easy to measure predictors that may assist in the early identification of patients at a higher risk for LVDD. In this study, we have examined two potential low-cost factors: BMI, as a measure of fatness, and VO2peak, as a measure of aerobic capacity as potential predictors for LVDD.
We reported that BMI strongly correlated with whole body fatness (measured by DXA) in this population and as such it can be used as a low-cost and easy to measure option to quantify obesity levels. In the current study, BMI was correlated with LVDD in patients with T2DM. It has been previously reported that BMI is an independent predictor of LVDD; and furthermore, overweight and obesity have a negative impact on diastolic function.26,27 The prevalence of LVDD in patients with T2DM was reported to be related to the fatness level and increases from 25% in those with normal weight to 30%-50% in overweight/obesity individuals and up to 57% in patients who are morbidly obese.26,28 We similarly found that higher BMI was related to worse peak-exercise diastolic function, even within our very heterogeneous population. However, this association was not evident for those with a lower VO2peak, and so our hypothesis was only partly supported by the data. It is not clear why VO2peak was not associated with LVDD in the current study, as previous studies reported correlations between this parameter and LVDD. 29 Indeed, it has been suggested that exercise E/E′ can distinguish between patients with exercise capacity of 8 METs or higher, which corresponds to VO2peak of ~28 mL/kg/minute, compared to those with lower exercise capacity (less than 8 METs). 30 However, the mean VO2peak in the current study was ~18 mL/kg/minute (or ~5 METs), which may limit the correlation. Furthermore, we used peak-exercise echocardiographic parameters to assess diastolic function, which are more sensitive than resting measures. 17 An additional study reported a significant relationship between functional capacity and LV diastolic function in healthy community–dwelling older adults (age >65 years). 31 The difference between the current study and the referred study was in the population studied; in the current study, only patients with T2DM who also have LVDD were included, which may explain the variance in results. In addition, the method used to assess aerobic capacity varied between studies; our study utilized the standard technique of indirect calorimetry to measure VO2peak, whereas earlier study used the less precise six-minute walking test. To further note in this population, exercise capacity and tolerance can be limited by diseases, such as that of the lung, eg, COPD7,8,32; however, in the current study, patients who have a history of lung disease that requires regular inhaler use were excluded. Our data further suggest that in our group of patients, VO2peak and BMI are not correlated, which may indicate that improvement in VO2peak post-interventions may be independent of change in BMI.
Together, the results from the current study indicate that not all risk factors for cardiometabolic disease have the same predictor capacity for LVDD, and BMI appears to be superior for predicting LVDD in patients with T2DM when compared to aerobic power. Our findings suggest that the use of BMI is not only a cost-effective clinical tool but given the ease or measuring fatness is also an efficient way of taking a preventative approach to screening for disease risk predictors.
Higher BMI was not correlated with LV systolic function, in contrast to the previously published data. 33 Our data show that those with higher VO2peak tend to have a higher LVEF, but no significant correlation was found between the two variables. This finding is interesting as previous studies that examined the relationship between VO2peak and LVEF in patients with LV systolic dysfunction (systolic heart failure) reported no correlations between these factors. 29 This supports the hypothesis that exercise capacity in patients with systolic heart failure is largely due to alteration in the periphery (ie, skeletal muscle). 34 Future studies should explore which factors (central and peripheral) are responsible for the reduction in exercise capacity in patients with T2DM with preserved LVEF but compromised diastolic function.
A potential limitation of the current study is the relatively small sample size. Thus, in one sense, these new data should be seen as hypothesis generating. In addition, the inclusion of patients with T2DM who have already developed some degree of LVDD may limit the findings. This is however, also a strength of the study as for the first time we looked at a selected group of individuals who may represent this population more closely than all people with T2DM, irrespective of LV diastolic function. Finally, some patients have reported a smoking history, which may affect exercise capacity; yet, these patients represent the smoking habits that are present in the general population, which may assist with the generalization of the results.
Conclusion
In conclusion, in individuals with T2DM with diastolic dysfunction, a higher BMI was associated with worsening diastolic function that is independent of their aerobic capacity. The data provide a simple and practical approach to assist in identification of functional changes to the heart diastolic function in this population.
Author Contributions
Conceived and designed the experiments: IL, MA, MS, DH, GJ, CW. Analyzed the data: CS, EH, MH, IL. Wrote the first draft of the manuscript: CS, IL. Contributed to the writing of the manuscript: All authors. Agree with manuscript results and conclusions: All authors. Jointly developed the structure and arguments for the paper: CS, IL, MA, DH. Made critical revisions and approved final version: All authors All authors reviewed and approved of the final manuscript.