
Abstract
Incidental extracardiac findings (ECFs) are commonly noted on cardiac imaging. The majority of the ECFs are noticed on computed tomography (CT), cardiac magnetic resonance scanning, and myocardial perfusion imaging. Although transthoracic echocardiography (TTE) is a widely used cardiac modality, there is scarcity of data describing ECF on TTE. ECFs have the potential to alter patient management. We present a rare case of a cystic mass seen in the posterior mediastinum on TTE, which led to further evaluation and diagnosis of esophagitis with ulceration.
Introduction
Incidental extracardiac findings (ECFs) are commonly seen on the many cardiac imaging modalities. The majority of the incidental ECFs are noticed on computed tomography (CT), cardiac magnetic resonance scanning, and myocardial perfusion imaging, but transthoracic echocardiography (TTE) can also reveal these incidental findings, especially since it is a widely used cardiac modality. However, there is scarcity of data describing ECFs on TTE. We present a rare case of a cystic mass seen in the posterior mediastinum on TTE, which led to further evaluation and diagnosis of esophagitis with ulceration.1–4
Case Summary
The patient is a man in his 70s with a past medical history of bipolar disorder, pulmonary embolism, deep venous thrombosis, benign prostatic hyperplasia, gastroesophageal reflux disease (GERD), and anemia who presented with chest pain. The patient had been experiencing chest pain for several months, which he described as being non-radiating, nonexertional, and often postprandial. The patient also reported he was not eating or drinking well secondary to a decreased appetite. The review of systems was negative for dizziness, syncope, shortness of breath, fevers, chills, nausea, vomiting, dysphagia, or recent weight loss.
On physical examination, the patient's orthostatic vital signs were as follows: supine blood pressure (BP), 100/75 mm Hg; pulse, 125 bpm; standing BP, 90/55 mmHg; and pulse, 128 bpm. Generally, the patient appeared in no acute distress with dry mucus membranes and decreased skin turgor. His cardiac examination revealed normal S1 and S2 heart sounds with tachycardia. The rest of the examination was unremarkable. Laboratory studies revealed a blood urea nitrogen (BUN) of 36 mg/dL and serum creatinine of 1.0 mg/dL. Cardiac markers were normal. The patient underwent a TTE for the evaluation of his chest pain. A possible cystic mass posterior to the left atrium was noted on the TTE (Fig. 1). This prompted further evaluation of the thoracic cavity with a CT of the chest. The CT revealed a diffuse, fluid-filled dilatation of the esophagus with mild distal wall thickening (Figs. 2 and 3). The patient subsequently underwent an esophagogastroduodenoscopy (EGD) revealing erosive esophagitis with ulcerations as well as a hiatal hernia. As a result of this finding, the patient was started on aggressive proton pump inhibitor therapy and will be followed by gastroenterology. Once the esophagitis has resolved, plans will be made to further evaluate the patient for possible motility pathologies that may have led to the distal esophageal thickening.
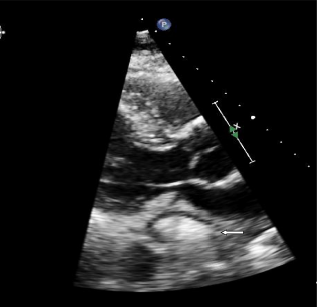
Transthoracic echocardiogram in the parasternal long axis view showing a cystic mass visible posterior to left atrium (arrow).

CT of the thorax in the axial plane at the level of the heart. Dilated, fluid-filled esophagus, posterior to the heart (arrow).

CT of the thorax in a more cranial axial plane than Figure 2 further reveals the dilated esophagus partially filled with fluid, posterior to trachea and anterior to the thoracic vertebrae (arrow).
Discussion
Incidental ECF on TTE has the potential to change management in patient care. Although there is no concrete definition of ECF in the literature and data are scarce, most physicians agree that liver, lung, and mediastinal abnormalities are characterized as ECF; however, aortic dilatation or an aortic atheroma and thrombus visualized on a transesophageal echocardiography (TEE) are not considered ECF. 1 In the literature, ECFs are characterized into low-risk findings, which include pleural effusions, ascites, or hiatal hernia, or high-risk findings, which include liver abnormalities, inferior vena cava (IVC) pathology, mediastinal masses, and descending aortic dilatation. 2
Alkhouli et al conducted a retrospective review of over 41,000 patients with ECF on TTE and TEE. ECFs were more commonly seen on TEE (22.2%) when compared to TTE (3.6%) with the discovery of aortic atheromas, aortic thrombi, and pleural effusions being the most common findings. 2 In this review, only six patients had mediastinal or lung masses and there were no reports of esophageal pathologies on TTE or TEE.
Furthermore, in a retrospective study of over a thousand people undergoing TTE, Khosa et al reported an ECF rate of 7.5%. 3 ECFs were divided into three different categories: benign, intermediate, and worrisome. Benign findings were described as hepatic cysts, hemangioma, and uncomplicated cholelithiasis; intermediate findings consisted of ascites, pleural effusions, and cholecystitis; and worrisome findings were significant of IVC filling defects, liver metastasis, portal vein thrombosis, to name a few. 3 Similar to Alkhouli et al, there were no reports of esophageal pathology presenting as ECF in this study either.
In our patient, the ECF represented esophagitis, which is defined as inflammation of the esophageal mucosal surface. The most common cause of esophagitis is GERD, but it may also be attributed to alcohol use, medications such as nonsteroidal anti-inflammatory drugs (NSAIDs), infection, radiation treatment, or autoimmune disorders.5,6 The presentation of esophagitis may range from retrosternal chest discomfort to dysphagia and odynophagia. At times, ulcerative esophagitis can cause significant odynophagia, which limits oral intake enough to cause dehydration and weight loss. Moreover, spontaneous substernal pain or burning may occur, unrelated to eating, which makes it difficult to distinguish the pain from a cardiac etiology. 1 In our patient, substernal chest pain was accompanied by loss of appetite; however, the severity and character of his symptoms warranted further cardiac work-up.
Conclusion
Although studies have been conducted to evaluate ECF on cardiac imaging studies, there is a paucity of studies on esophageal pathology as an ECF. In the case presented in this report, the appearance of a posterior mediastinal mass on TTE was essential in prompting further evaluation and eventual diagnosis of erosive esophagitis with ulceration. Various etiologies should be considered in the setting of ECFs, including esophageal pathology.
Author Contributions
Wrote the first draft of the manuscript: SS, SK, SK, RZ, ANM. Contributed to the writing of the manuscript: SS, SK, SK, RZ, ANM. Agree with manuscript results and conclusions: SS, SK, SK, RZ, ANM. Made critical revisions and approved final version: SS, SK, SK, RZ, ANM. All authors reviewed and approved of the final manuscript.