
Abstract
Objectives
We sought to evaluate the utility of multidetector computed tomography (MDCT) in preoperative planning of cardiac resynchronization therapy (CRT) device implantation.
Background
Variation in coronary venous anatomy can affect optimal lead placement and may warrant preimplantation visualization prior to CRT lead placement.
Methods
Prospective randomized enrollment of 29 patients (17 males; mean age at implant 66.7 ± 12.8 years) was undertaken. Patients were randomized to preimplantation MDCT (GE® 64-detector Lightspeed, n = 16) or no MDCT. Implantation was planned based on three-dimensional coronary venous reconstruction as visualized in the CT group. Measurement of coronary sinus (CS) angulation, CS ostial (os) diameter, right atrial (RA) width, volume, and height was undertaken prior to implant. Intraoperative CS lead implantation times (introduction, cannulation, and left ventricular [LV] lead positioning), procedure time, fluoroscopy time, and venogram contrast volume were measured to determine if there was a difference between patients who underwent preimplant CT scan and those who did not.
Results
CS os diameter (mean = 13.8 ± 2.9 cm) was inversely correlated with total fluoroscopy time (r = -0.57, P = .008), and total procedure time, but this correlation was not statistically significant (r = - 0.36, P = 0.12). RA width (mean = 52.8 ± 9.9 cm) was associated with a shorter total procedure time (r = −0.44, P = .047) and LV lead positioning time (r = −0.33, P = .012). There were no statistically significant differences between the CT group and the non-CT group with respect to total intraoperative and fluoroscopy times or venogram contrast volumes. Total procedure time was longer in the CT group but the difference was not statistically significant (94 ± 27.2 vs. 74.7 ± 26.6; P = .065).
Conclusion
Noninvasive visualization of the coronary venous anatomy before CRT implantation can be used as a guide for lead placement. While no significant differences were noted between the two groups with respect to intraoperative variables, CS os diameter and RA width inversely correlated to a shorter procedure time and LV lead positioning time, respectively. Further clinical trials regarding the utility of MDCT to visualize coronary venous anatomy prior to CRT implantation for procedural planning and lead placement guidance are warranted.
Introduction
Cardiac resynchronization therapy (CRT) has become a treatment option for highly symptomatic heart failure patients with a wide QRS complex on electrocardiography and depressed left ventricular (LV) systolic function.1–4 Electrical and mechanical cardiac dysynchrony has been shown to have a detrimental impact upon overall cardiac function with poor ventricular filling times and septal dyskinesis in addition to exacerbation of preexisting valvular conditions, particularly mitral regurgitation.5–7
To improve CRT implant success rate, LV pacing target regions can be assessed before implantation. Ideally, knowledge of the coronary venous anatomy should be assessed before noninvasive implantation, either in the outpatient clinic or in the hospital setting to determine whether a transvenous approach is feasible. Variation in coronary venous anatomy has been described in addition to the absence of coronary sinus (CS) tributaries, especially in post-myocardial infarction patients secondary to scarring. 8 The feasibility of using multi-detector computed tomography (MDCT) to visualize the coronary anatomy was previously studied, further describing the marked variability in venous anatomy. 8
Initial experience with CRT utilized epicardial LV pacing through leads positioned via limited thoracotomy. This method of lead placement was associated with surgical risk, which led to the development of transvenous LV pacing techniques. With currently available pacemaker lead technology and appropriate experience, LV pacing can be undertaken through the left-sided epicardial tributaries of the CS. Successful LV lead implantation is dependent upon the presence of preexisting intracardiac leads; the anatomy of the coronary veins; available instrumentation including guide catheters, sheaths, wires, and LV pacing leads; and the individual experience of the physician conducting the procedure. Furthermore, knowledge of LV venous anatomy may be useful beyond the actual procedure of LV lead implantation. Recent studies demonstrated that the location of the LV lead within the LV has a dramatic effect upon the hemodynamics of LV contraction as well as on long-term outcomes following CRT device implantation. 9
The process of gaining proper coronary access requires extensive knowledge of the right atrial (RA) and CS anatomy. This can be individualized to each patient by imaging the coronary venous system using MDCT coronary angiography prior to lead implantation. The success of CS cannulation is also implanter dependent, and complications have been known to arise including coronary venous dissection, phrenic nerve stimulation, lead dislodgement, hematoma, and pneumothorax. Currently, there is a consensus that the cannulation of the CS remains the technique of choice to place the LV lead. Cannulation of the CS can be exceedingly difficult and time consuming using fluoroscopy alone. The need for general anesthesia, possible intubation, and esophageal manipulation further limits the utility of this approach. 10 With preoperatively obtained MDCT, it may be possible to use the visualized anatomy to aid in directing CRT implantation. The purpose of this study was to determine the utility of preoperative MDCT with anatomical characterization of CS dimensions and tributary structure in guiding CS lead implantation in patients undergoing CRT implantation.
Methods
This is a prospective randomized trial targeting patients (age >18) with class II, III, or IV heart failure (as defined by the New York Heart Association [NYHA]) and an ejection fraction of less than 35% who were admitted to North Shore University Hospital and were deemed to require CRT implantation as part of standard medical management. A total of 29 patients were enrolled into the trial. Three individual implanters participated in this study. Initially, patients were randomized to either a control group which received CRT without MDCT guidance or the MDCT experimental group where the implanters reviewed the images prior to CRT implantation. After the first 12 patients, the protocol was adjusted and every patient enrolled underwent a preoperative MDCT scan. The initial randomization was maintained, however, and the implanter reviewed the MDCT images of only those patients who were randomized into that group. Expansion of MDCT to all enrolled patients was implemented to further explore the anatomical variables. Both groups received the standard of care for their heart failure, which is implantation of the CRT. The biventricular pacing generator used was Medtronic® Concerto model #C154DWK for all patients. The atrial and ventricular leads varied and were left up to the discretion of the implanting electrophysiologist.
The implanter reviewed the MDCT images of the coronary venous anatomy prior to CRT implantation. In order to minimize potential bias for trying to implant leads at a faster pace, the implanter was blinded to the specific variables measured during the procedure. A health-care provider was present in the operating room during the procedure to perform data collection intraoperatively.
Informed consent and follow-up
Following approval by the institutional review board of the North Shore LIJ Health System, the study began with the recruitment of eligible patients. The patients who were randomized to receive MDCT were consented and then underwent CRT. Patients enrolled in the trial were followed up within 48 hours and received routine phlebotomy to monitor their serum creatinine levels following the CT scan. This research was conducted in accordance with the principles of the Declaration of Helsinki.
Participation Criteria
Inclusion criteria stated that all patients must be ≥18 years of age with Stage II, III, or IV heart failure who have a creatinine ≤1.6 mg/dL. These patients were already admitted to North Shore University Hospital and were scheduled to undergo CRT for their heart failure as standard of care. Also, patients must not have undergone CRT implantation in the past. Patients with atrial fibrillation were not excluded. Exclusion criteria pertained to any patient less than 18 years of age or who did not meet NYHA HF class II, III, or IV criteria, was not eligible for CRT implantation based upon current guidelines, and who had a creatinine level greater than 1.6 mg/dL.
Variables Analyzed and Endpoints
The primary endpoint was total procedure time, which was defined as time from initial incision to wound closure. Additional parameters analyzed intraoperatively and compared with the control group (where the implanter did not review the MDCT) included CS access to CS cannulation time, CS cannulation to LV introduction time, LV introduction to positioning, LV lead time (measured from initial CS access to successful LV lead positioning), total fluoroscopy time, and volume of dye used during venogram.
MDCT anatomical measurements
All patients were scanned with an MDCT scanner (GE® LightSpeed VCT, GE Healthcare Amersham Health, Princeton, NJ, USA) equipped with 64-MDCT technology. Scan parameters were as follows: number of slices per rotation, 64; individual detector slice width, 0.625 mm; and 12.5-cm spatial coverage in 5 seconds at a gantry rotation speed of 330 ms. After the patient was advanced into the scanner bore, a 20-mL test bolus of contrast was administered. Images were then obtained over the CS body to time the arrival of contrast material to the coronary veins. The scan was timed when a threshold of approximately 100 Hounsfield units was reached in the CS body. Patients were asked to breathe deeply and then hold their breath. After bolus administration of 70 mL of nonionic iodinated contrast material (Omnipaque™ [iohexol]; GE Healthcare, Amersham Health) at a flow rate of 5 ml/s, image acquisition was performed. The scan time was approximately 10 seconds (one breath-hold).
Image acquisition was performed at 10% increments through the R-R cardiac cycle interval. After retrospectively gated image acquisition to allow for the full cardiac cycle phase acquisition, images were transferred to a GE® AW workstation where they were reconstructed with the appropriate electrocardiogram (ECG) gating phase for adequate image and structure visualization and interpreted by an experienced reader. Specific attention was focused on analysis of the anatomic characterization of the coronary venous system.
The tributaries of the cardiac venous system were also identified on axial and volume-rendered reconstructions and a 3-dimensional (3D) reconstruction of the venous system was created. The presence of the following cardiac veins was evaluated: CS, great cardiac vein, anterior interventricular vein, middle cardiac vein (posterior interventricular), lateral cardiac vein (marginal vein), and posterolateral cardiac vein. Quantitative parameters were also assessed. The ostium of the CS was defined as the site where the CS makes an angle with the RA. Multiplanar reformatting of axial images was used to determine the CS ostial (os) diameter and CS angulation. Further, RA height and width were quantified.
Surgical Procedure
Standard surgical technique was employed. The right ventricular lead was advanced under fluoroscopic guidance to the right ventricular apex and secured by passive fixture. The CS was visualized using GE® Iohexol contrast dye and the CS cannulated using fluoroscopic guidance to allow lead entry and positioning into the posterolateral position to pace the LV without diaphragmatic stimulation. Two-dimensional fluoroscopic visualization of CS tributaries was obtained during LV lead implantation. A CS occlusion balloon was inflated and contrast injected retrograde to blood flow in order to opacify the coronary venous system. The RA lead was then advanced under fluoroscopic guidance to the RA and secured by active fixture. Acceptable pacing and sensing parameters were obtained. The pulse generator was attached to the leads, and the set screws were tightened and verified. The defibrillator was placed into the pocket. Defibrillation threshold testing was then performed. Finally, postprocedure chest radiograph was ordered and checked for lead placement.
Statistical Methods
The primary endpoint variable of the study was the total procedure time. The Mann–Whitney test was used to compare the various time parameters between the two treatment arms. Correlations (Spearman) were calculated to determine the strength of correlations among various CT scan parameters (RA volume, RA width, RA height, CS angulation, and CS os diameter) and parameters of interest (time to sinus lead implantation, time to CS cannulation, fluoroscopy time, volume contrast, total procedure time, etc.)
Results
There were a total of 29 patients who completed the study. Baseline patient characteristics included age, race, American Heart Association Heart Failure Class (I–IV), and medication regimens (Table 1). Of the 29 patients overall, the mean age at time of enrollment was 66.7 ± 12.8 years (range 39-87 years). In the patient cohort, 12.5% (2/29), 81.25% (13/16), and 6.25% (1/16) patients were classified as heart failure classes II, III, and IV, respectively.
Baseline characteristics.

Intraoperative Parameters
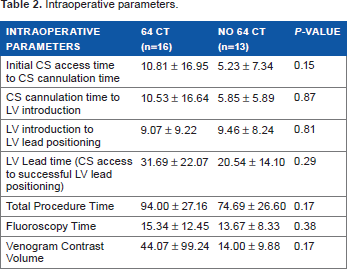
There were no statistically significant differences between the MDCT group and the non-MDCT group with respect to intraoperative lead implantation times, venogram contrast volume, and fluoroscopy times. Table 2 lists the individual steps and times recorded from initial CS access time through final LV lead positioning, fluoroscopy time, and venogram contrast volume.
intraoperative parameters.
Coronary Venous Anatomical Measurements
Among all CT scans, CS os diameter (mean = 13.4 ± 2.9 cm) was inversely correlated with total procedure time, though this correlation was not statistically significant (r = −0.35, P = .1234). CS os diameter was also inversely correlated with the total fluoroscopy time (r = −0.57, P = .0084). Figure 1 demonstrates the scatter plot and the trend line for both correlations. RA width (52.8 ± 10.1 mm) was inversely correlated with total procedure time (r = 0.45, P = .0469) and LV lead positioning time (r = −0.33, P = .012). Figure 2 demonstrates the scatter plot of total procedure time versus RA diameter with a trend line.
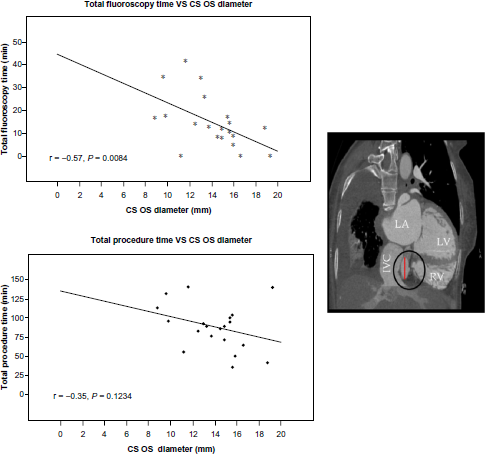
Correlation between CS os diameter (red line across the sagittal CT section) and total procedure and total fluoroscopy times. Both times display significant inverse correlation with CS os diameter.
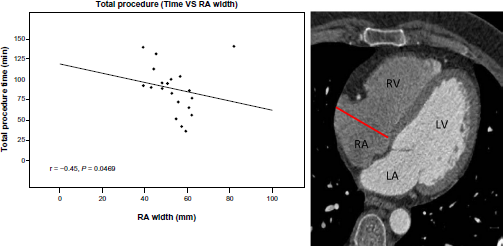
Correlation between the RA (red line across the axial CT slice) width and total procedure time. Larger RA width is inversely correlated with total procedure time.
Venous Anatomy
Eight cardiac venograms were deemed to be of acceptable quality (with sufficiently distal contrast penetration) and were compared to 3D reconstructions of the coronary venous system (Fig. 3). Out of four anterior, seven lateral, five middle, and six posterior veins identified on fluoroscopy, the MDCT scans identified 4/4 anterior veins (100%), 4/7 lateral veins (57%), 3/5 middle veins (60%), and 4/6 posterior veins (66.7%). For the instances where the vessels were not visualized on fluoroscopy (four anterior, one lateral, two middle, and two posterior veins), the CT result was concurrent in 1/4 (25%), 0/1, (0%), 1/2 (50%) and 2/2 (100%) instances.
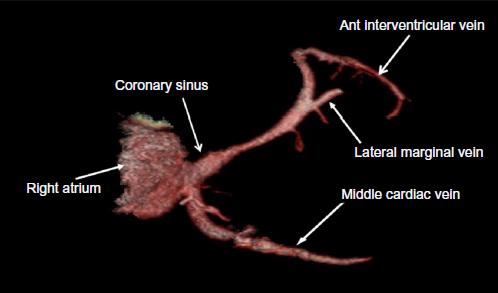
3D reconstruction of the coronary venous system.
Discussion
When CRT was introduced as a potential therapeutic option for patients with medical therapy–refractory heart failure, operators depended upon epicardial LV pacing conducted via leads that were placed via a limited thoracotomy, a procedure which carried an obvious surgical risk. 8 Since the introduction of CRT, new techniques to facilitate implantation have been developed so as to justify the risk–benefit ratio associated with the procedure. The utilization of transvenous lead placement has resulted in significantly reduced morbidity and mortality, facilitating a potentially challenging procedure.
Despite the technical utility of utilizing the transvenous approach, variations in vascular anatomy have the potential to render even this less invasive procedure more difficult, resulting in increased operative times, exposure to fluoroscopy, contrast dosages, and errors in lead placement. As a result, precise knowledge of coronary vascular anatomy prior to implantation has the potential to decrease the morbidity associated with unexpected vascular variations. The expansion of available noninvasive means to accurately assess the cardiac arterial and venous system, particularly via coronary CT angiography and magnetic resonance angiography, may alter the way in which we approach CRT. Prior to the modern era of noninvasive cardiac visualization, coronary veins could only be visualized via retrograde venography, an invasive procedure that carries with it the risks associated with any type of invasive angiography including infection, vascular disturbance, and contrast-induced nephropathy, as well as exposure to fluoroscopy.11–13 Over the past five years, however, numerous studies indicating good results with noninvasive assessment of the coronary venous system in particular have been published.
The use of MDCT angiography to assess coronary arteries has been studied extensively. The utility of this technology in the evaluation of the venous system, however, is less proven. In 2000, Schaffler et al demonstrated adequate delineation of the venous system (particularly the CS and its tributaries) and its spatial relation to other cardiac structures using ECG-triggered electron beam CT. 14 Mao et al examined the use of electron beam computed tomography to visualize the venous system, relationships to coronary arteries, and the presence of unexpected venous anomalies. 15 More recently, several other studies examining the use of 16- and later 64-MDCT have demonstrated success in adequately mapping venous structures. Despite concerns over inadequate venous opacification given that the MDCT studies were geared toward visualization of the arterial system, venous anatomy could be adequately delineated in the vast majority of patients. Information regarding vessel lengths, diameters, course, and relation to other anatomic structures was readily available from analysis of the CT images.16,17
The clinical implications of precise knowledge of the venous anatomy prior to implantation can be very significant for many aspects of electrophysiology. While the information obtained from MDCT can certainly be useful for procedures such as radiofrequency ablation and myoblast transplantation performed via catheter-based procedures, the significant technical difficulties that are often encountered during CRT implantation make application of noninvasive imaging to this procedure even more significant. There is a significant potential for cardiac venous anatomical variation particularly with reference to the task of localizing lateral and posterior venous branches of the venous system. 18 In 2005, Jongbloed et al used MDCT to map variations in the cardiac venous system, noting significant interindividual differences in the origin and continuity of the major venous tributaries as well as the number of vessels, particularly posterolateral tributaries, available for cannulation of the CS. 8 As a result, knowledge of the presence of unexpected variations in anatomy prior to CRT implantation can be a boon to the operator.
Anatomical variation has led to a unique classification of the venous system. Singh et al proposed using a segmental approach to classifying the CS branches and tributaries by the segment of myocardium that a particular vein or venous tributary overlies utilizing their original location rather than anatomical designations. 19 Studies have also concentrated on targeting the anatomic origin of the venous system and applying noninvasive visualization of the venous anatomy prior to radiofrequency ablation. Tada et al enrolled 70 patients (65 had paroxysmal atrial fibrillation and atrial tachycardia) who underwent MDCT to determine the morphology and size of the left atrium and pulmonary veins prior to ablation. Visualization was possible in 91% of the patients with specific visualization of the lateral aspect of the LV with at least one vein being invariably detected and two veins visualized in 36% of patients and more than two veins in 45% of enrolled patients. 20
The feasibility of noninvasive evaluation of the coronary veins has been confirmed in populations of patients with and without coronary artery disease as well as prior infarction. Van de Veire et al studied venous anatomy with MDCT in 100 patients comprising three groups: control patients, patients with coronary artery disease, and patients with a history of prior myocardial infarction. The CS, middle cardiac vein, and posterior vein of the LV were identified in all subjects. The left marginal vein was observed significantly less in patients with a previous history of myocardial infarction. 21 Absence of LV tributaries in patients with a history of myocardial infarction may lead to more difficult lead positioning techniques which may also impart longer fluoroscopy exposure and longer procedure times. Drastic alterations in venous anatomy may preclude transvenous placement of LV lead altogether, leading to a surgical implantation. Clinical implications of preoperative visualization of the coronary venous system specifically the lateral aspect of the LV can contribute to successful lead implantation for CRT.
Our study demonstrates the capacity of MDCT to delineate large venous structures as well to characterize the environment through which the LV lead must be advanced to achieve optimal LV pacing. By utilizing 3D reconstruction, CS os diameter, angulation, RA, height, and width could be assessed with great accuracy thereby providing a wealth of information prior to introduction of the leads required for CRT. Furthermore, we showed that MDCT can be used to reconstruct coronary venous structures with accurate fidelity compared to intracoronary venograms. The ability to predict availability of appropriate target vessels is an additional utility of MDCT scanning prior to CRT implantation.
The ability of MDCT to provide information regarding the venous anatomy becomes even more important when attempting more technically challenging procedures such as CRT. The implantation of a biventricular pacemaker usually requires stimulation of the LV, which is currently most often achieved via the transvenous approach, usually through a tributary of the CS. The need for placement of a LV lead necessitates knowledge of the posterolateral cardiac venous anatomy to facilitate access to the often small, tortuous tributaries of the CS.15–17 In addition, variations in the angle and diameter of the great cardiac vein could make cannulation of a LV vein more challenging, thus increasing operative times, exposure to fluoroscopy and the potential for suboptimal lead placement. In addition to facilitating the actual procedure, visual knowledge of the venous anatomy prior to the procedure may prepare the operator for the degree of difficulty of the procedure and even guide selection of equipment. As a result, there is a significant potential benefit for utilizing coronary CT angiography prior to attempting BVP implantation, and as the spatial and temporal resolution available for CTA increases, so will the amount of information that can be garnered from these studies.
Our data showed that there was no statistically significant difference between the MDCT group and non-MDCT group with respect to intraoperative times, fluoroscopy time, or venogram contrast volume. These findings are likely due to the small sample size of the study. Comparison of the two groups of patients showed that although not significant, the majority of the intraoperative variables measured, including initial CS access time, time of CS cannulation, LV introduction time, and time of final LV lead positioning took longer to complete in the MDCT group. Difficulties in lead advancement intuitively would likely cause a low lead implantation success rate, longer times of fluoroscopy use and larger quantities of dye, as was the case when comparing the two groups of patients. The anatomy through which the LV lead is advanced consists of the subclavian vein, the superior vena cava, the RA, the CS os, and the course of the CS as well as its tributaries. The anatomic dimensions of these structures can vary from patient to patient and can drastically affect the CRT implantation procedure, as demonstrated by the broad range of intraoperative variable measurements. The intrinsic environment of the venous system itself specifically the Valve if Vieussens and Thebesian valves may pose a mechanical or obstructive threat toward a successful, shorter lead implantation. Another explanation for the increased times seen in the MDCT group may relate to the inherent learning curve by implanters in using the CT images to guide lead placement compared to use of more familiar CS venograms for guidance. This highlights an important point that familiarity, and a certain experience is required in interpreting these MDCT images for them to be used in a beneficial manner.
We showed that greater the CS os diameter and RA width, shorter is the CS lead implantation time. The CS os diameter and the course of the CS play an important role in determining the success of lead advancement toward the optimal posterolateral position of the LV. It may also be possible to use MDCT to exclude patients from transvenous lead implantation. Knowledge of a small CS os preoperatively may warrant epicardial lead placement to pace the LV. Perhaps there lies a critical diameter of the CS os, which would direct implanters toward an epicardial approach. Preoperative knowledge of the CS os diameter and RA dimensions may allow implanters to stratify patients into a group that would be more technically difficult or less suited for a successful, shorter, and safer transvenous approach to CRT implantation. Figure 3 shows a full 3D reconstruction of the CS, its course, and major tributaries. Our data indicate that this 3D reconstruction may be used with high certainty to predict the presence of appropriate tributaries for LV lead placement. Smaller caliber vessels that may have been noted on fluoroscopy may not have been visualized, but these caliber vessels are too small for lead advancement and therefore are of no major clinical significance. Use of this “roadmap” preimplantation may guide the implanter toward the optimal posterolateral lead implantation site, thereby achieving cardiac resynchronization.
The utility of MDCT in CRT is likely to expand beyond facilitating the actual procedure and to affecting the long-term outcomes of CRT therapy as our experience with resynchronization grows. At present, implantation of the LV lead is targeted to the lateral/posterior wall of the LV. The reasoning behind this approach is that positioning the lead as far away from septum and to the latest depolarizing section of the ventricle should have the greatest impact in LV dyssynchrony. However, recent work by Merchant et al indicates that simply positioning the LV lead in the lateral/posterolateral position of the LV lead is not always sufficient and longitudinal outcomes depend on the leads' position along the long axis of the ventricle as well. 22 Specifically, patients undergoing CRT were divided into two groups based on the final location of the LV lead; apical or basal/midventricular. After 15 months of follow-up, the group with the apical lead demonstrated a clinical severity–adjusted HR of event-free survival of 2.3 compared to the basal/midventricular group. NYHA and LV remodeling were also adversely affected. Derval et al recently demonstrated that hemodynamic and echocardiographic changes induced by resynchronization vary dramatically in each patient based on the position of the LV lead, that position not being limited to the posterior/lateral sites of the ventricle traditionally utilized. 23 As the role of the pacing site location becomes more important, the individual venous anatomy of each patient will become crucial in planning the CRT procedure and affecting long-term outcomes.
Conclusion
Noninvasive visualization of the coronary venous anatomy before CRT implantation can be used as a guide for lead placement. Lead placement and choice of approach (transvenous vs. epicardial) can be directly and indirectly affected by variations in anatomy and limitations in anatomical dimensions through which the lead is advanced. Our study shows that intracardiac venous anatomy, in particular CS os diameter and RA width, do play a role in predicting optimal lead positioning by visualizing CS anatomy and course. Further analysis of the use of MDCT as a guide for CRT lead implantation is warranted.
Author Contributions
Conceived and designed the experiments: JNC, JNM, RJ, ANM. Analyzed the data: JNC, JNM, RJ, ANM. Wrote the first draft of the manuscript: JNC, ANM. Contributed to the writing of the manuscript: JNC, JNM, RJ, ANM. Agree with manuscript results and conclusions: JNC, JNM, RJ, ANM. Jointly developed the structure and arguments for the paper: JNC, JNM, RJ, ANM. Made critical revisions and approved final version: JNC, JNM, RJ, ANM. All authors reviewed and approved of the final manuscript.