
Abstract
Patients with end-stage liver disease in need of liver transplantation increasingly are older with a greater burden of cardiac disease and other co-morbidities, which may increase perioperative risk and adversely affect long-term prognosis. Cirrhosis of any etiology manifests hemodynamically as a state of low systemic vascular resistance, with high peripheral, but low central blood volume, leading to a state of neurohormonal activation and high cardiac output, which may adversely affect cardiac reserve under extreme perioperative stress, aptly termed cirrhosis-associated or cirrhotic cardiomyopathy. Evidence of asymptomatic cirrhotic cardiomyopathy may be found in subtle electrocardiographic and echocardiographic changes, but may progress to severe heart failure under the demands of bleeding and transfusions, vasopressors, rebounding peripheral vascular resistance, withdrawal of cardioprotective beta-blockers and mineralocorticoid antagonists, exacerbated by sepsis or systemic inflammatory response syndrome. This review will add to the current body of literature on cirrhotic cardiomyopathy by focusing on the role of advanced echocardiographic imaging techniques, cardiac biomarkers, and advanced heart failure therapies available to manage patients with cirrhotic cardiomyopathy while waiting for liver transplant and during the perioperative period.
Keywords
Introduction
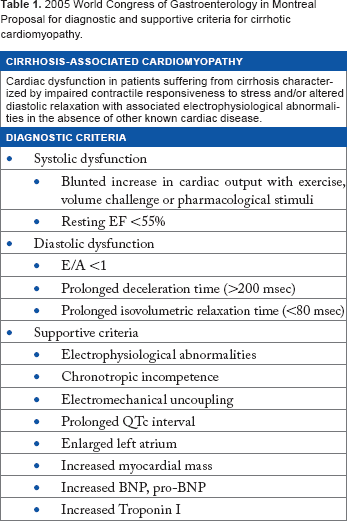
2005 World Congress of Gastroenterology in Montreal Proposal for diagnostic and supportive criteria for cirrhotic cardiomyopathy.
Working Definition of Cirrhotic Cardiomyopathy
First described in 1953, cirrhosis-associated cardiomyopathy (CAC) was described as a state of hyperdynamic circulation in patients with alcohol-related cirrhosis, characterized by high cardiac output, tachycardia, vasodilation, and a blunted response to cardiac inotropes or vasopressors. 7 In 2005, a working group on the cardiac manifestations of end-stage cirrhosis of any etiology was convened, and CAC was defined as “chronic cardiac dysfunction in patients with cirrhosis, characterized by blunted contractile responsiveness to stress, and/or altered diastolic relaxation with electrophysiological abnormalities, in the absence of known cardiac disease” (Table 1). 6 The net effect of derangements in neurohormones, activation of the sympathetic nervous system, and an excess of circulating vasodilating substances is a state of decreased systemic vascular resistance with peripheral hypervolemia, but with central hypovolemia, which results in a high circulatory state. Increased systemic blood flow may lead to cardiac volume overload and secondary four-chamber cardiac dilatation, followed by myocardial failure. Any loss of myocardial contractile reserve may be well-masked by the peripheral vasodilated state, manifested by hemodynamic stress related to extreme hypotension (eg, bleeding, sepsis) and worsened by increases in endogenous and exogenous vasopressors, with resulting increased afterload and subsequent heart failure.
Neurohormones, Hemodynamic Stress, and Molecular Derangements
Progressive cirrhosis, with portal hypertension, is characterized by the development of portosystemic shunts and inadequately cleared circulating vasoactive substances eg, nitric oxide, vasoactive intestinal peptide, endocannabinoids, and bile salts, which create a state of splanchnic and arterial vasodilation, leading to ineffective central blood volume, initially compensated by high cardiac output.3,8 With worsening cirrhosis, systemic vascular resistance continues to fall, but cardiac compensation reaches a maximum. Concomitant compensatory responses include activation of the renin–angiotensin–aldosterone and sympathetic nervous systems with associated renal bed vasoconstriction and sodium and solute-free water retention to maintain blood pressure. 9 Progressive cirrhosis, from the pre-ascitic stage through frank hepatorenal syndrome, is correlated with steady increases in plasma renin and aldosterone levels, which are not suppressed by expansion of central blood volume. 10 Progressive cardiac dysfunction occurs in the setting of chronic renin-angiotensin-aldosterone and sympathetic nervous system activation, high circulating blood volume, and elevated levels of circulating vasoactive substances, which have direct myocardial toxicity. 6 Patients with cirrhosis are often intolerant to angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, which is likely related to the crucial role of the renin–angiotensin–aldosterone system in maintaining adequate vital organ perfusion.10,11
Increases in plasma norepinephrine, secondary to sympathetic nervous system activation, is associated with severity of Childs–Pugh score, as well as presence of hepatorenal syndrome. 10 Sympathetic nervous system activation serves to maintain vascular tone in the presence of inadequate arterial blood pressure, and sustained elevation of resting heart rate contributes to the high circulating volume/high cardiac output seen in end-stage cirrhosis. Sympathetic nervous system activation is associated with progressive sodium and solute-free water retention through its vasoconstrictive effects on the afferent and efferent renal arterioles. 10 Despite the widespread use of beta-blockers in cirrhotic patients as a treatment for variceal bleeding, chronic activation of the sympathetic nervous system leads to down-regulation of beta-adrenoreceptors and impaired or uncoupling of beta-adrenoreceptors signaling pathways, which manifests as myocardial hyporesponsiveness to catecholamines. 12 In rat models of cirrhosis, there appears to be nitric oxide-mediated vascular and cardiac inotropic hyporesponsiveness to vasoconstrictors, with improvement after addition of nitric oxide inhibitors. 13 Numerous other cytokines such as TNF-alpha and other cytokines that activate the nuclear-factor-kb pathway as well as endocannabinoids and bile salts are implicated in the vasodilatory and vascular/inotropic hyporesponsiveness seen in cirrhotic animal models.3,6,8 The overall systemic effect of cirrhosis is a high output state with high heart rate, high cardiac output, inadequate central blood volume, and low peripheral vascular resistance, which creates a state of high sheer wall stress, high volume overload state of the heart. The molecular effects of cirrhosis include beta-adrenoreceptor down-regulation, signal transduction abnormalities, nitration of cardiac proteins, and toxicity from endocannabinoids and bile salts, resulting in a toxic myocardium.
Cardiac Risk Profile in LTx Candidates
In 2013, there were 6,256 patients with ESLD who underwent LTx in the United States, with 16,411 patients currently on the waiting list. 14 Increasingly, LTx candidates are older, with a greater burden of CAD, co-morbidities of diabetes mellitus, hypertension, and hyperlipidemia, with higher Models of End Stage Liver Disease (MELD) scores at time of transplant, indicating a higher risk patient population.15,16 Burden of CAD in ESLD patients varies from 18-28%.1,17 Recently, Cross and colleagues reported that age, diabetes, prior CAD, left ventricular hypertrophy, and preoperative troponin I level >0.07 were predictors of post-LTx cardiovascular events after a mean of 8.2 years of follow-up, with 3.9% of patients in the cohort dying of perioperative heart failure, cardiac arrest, or acute coronary syndrome. 17 Safadi and colleagues reported that prior CAD, prior stroke, and post-operative sepsis predicted greater risk for acute coronary syndrome or death within 30 days after LTx. 16 Perioperative beta-blocker use was found to have a protective effect, further supporting their use during major abdominal surgery. Indeed, cirrhotic patients who tolerate perioperative beta-blockers are less likely to be on pressors or have suffered hepatorenal syndrome, possibly identifying lower risk surgical candidates. Not surprisingly, non-alcoholic steatohepatitis, a growing indication for LTx, is strongly associated with cardiovascular disease. 18
With regard to cardiovascular disease evaluation and management in the liver or kidney transplant candidates, the American Heart Association and American College of Cardiology (AHA/ACC) 2012 Guidelines recommend:
Non-invasive stress testing may be considered in LTx candidates with no active cardiac conditions on the basis of the presence of multiple CAD risk factors regardless of functional status. Relevant risk factors among transplantation candidates include diabetes mellitus, prior cardiovascular disease, left ventricular hypertrophy, age greater than 60 years, smoking, hypertension, and dyslipidemia. The specific number of risk factors that should be used to prompt testing remains to be determined, but the committee considers three or more to be reasonable (Class IIb; Level of Evidence C). 15
The recommendation was based on expert consensus and in accordance with prior American Association for the Study of Liver Diseases 2005 Practice Guidelines, which was an opinion-based (Grade III) recommendation:
Chronic smokers, patients over the age of 50 years, and those with a clinical or family history of heart disease or diabetes should undergo evaluation for CAD (Grade III). 19
Guidelines for this patient population depart from standard ACC/AHA Guidelines for pre-operative cardiac risk-stratification prior to surgery in that symptoms and functional capacity are not the key considerations in whether to perform stress testing. Patients with ESLD frequently have exertion intolerance that is difficult to isolate from cardiac insufficiency, and which may also conceal traditional cardiac symptoms as patients become more sedentary with disease progression. Importantly, the presumption of preoperative stress testing is that surgery will occur soon after risk stratification, which increasingly does not occur in this population, as wait times for LTx continue to increase and cardiac reserve may decline associated with worsening cirrhosis.
Pre-LTx Testing Modalities
The decision whether to perform myocardial perfusion scintigraphy (MPS) or dobutamine stress echocardiography (DSE) depends on patient-specific factors and physician and center expertise, in addition to the predictive accuracy of these testing modalities in the ESLD patient. There are numerous reports regarding poor correlation between segmental wall motion abnormalities on non-invasive imaging and angiography in this patient population.20–22 Additional concerns have been raised regarding the pharmacologic action of adenosine or dipyridamole stress agents in the vasodilated patient, as they may be inadequate to stress the myocardium under this condition. 20 Conflicting reports on the positive and negative predictive values of MPS testing are likely related to index of suspicion for CAD, as well as severity of cirrhosis, as assessed by MELD score. In one study, MPS demonstrated a negative predictive value of 99%, but this was in a low-risk cohort. 23 With regard to DSE, there are numerous reports of blunted heart rate and inotropic responses to dobutamine in cirrhotic patients, 1 yielding low negative predictive values because of inability to reach a targeted, predictive peak double product. More recently, Safadi and colleagues demonstrated increased negative predictive value of 89% for DSE in LTx candidates, but the majority of subjects had low MELD scores, thus the confounding effects of cirrhotic cardiomyopathy (blunted heart rate and inotropic response) were not likely evident in this population. 16
With the above recommendations for initial risk-stratification, the presumption is that the cardiac risk profile for a solid organ transplant candidate will not change meaningfully during time on the waiting list. However, the major dilemma in LTx is that progressive cirrhosis itself profoundly impacts myocardial reserve and integrity, which is not fully evaluated by standard stress imaging.
ECG Assessment in LTx Candidates
Prolongation of the QT interval (>440 milliseconds) is the most common ECG finding in cirrhosis, seen in up to 50% of patients and is associated with sudden cardiac death. 24 Chronic hyperactivation of the sympathetic nervous system and delayed repolarization of cardiomyocytes secondary to defects in K+ channel function have been observed in cirrhotic patients with associated QT prolongation, which may reverse after LTx, although may persist in up to 50% of patients.24–26 In addition, increased QT dispersion is associated with worsening liver dysfunction and with levels of plasma nora-drenaline. 26 TIPS insertion has been shown to prolong the QT interval, implicating myocardial volume overload as the mechanism, and is associated with one-year mortality. 27 Not surprisingly, use of beta-blockers for the treatment of varices is associated with reduction in QT prolongation.28,29 There is also experimental and clinical evidence of electromechanical uncoupling, with dysregulation in the normal sequence of cardiomyocyte depolarization and contraction.29,30
Echocardiographic Assessment of LTx Candidates
In addition to 12-lead ECG and non-invasive stress testing, echocardiography provides valuable information regarding the development of clinically important systolic and diastolic dysfunction. Trans-thoracic echocardiography (TTE) is non-invasive, available at the bedside, and low cost relative to other imaging modalities. As such, it is an important imaging technique to better understand the dynamic myocardial changes that may occur as cirrhosis worsens, volume overload becomes more severe and hepatorenal syndrome develops. The American Association for the Study of Liver Diseases recommends TTE as part of the evaluation of LTx candidates to assess for systolic and diastolic dysfunction, outflow gradients, hypertrophy, chamber sizes, and non-invasive assessment of pulmonary pressures. 19 Many echo studies on this patient population have been done, demonstrating variable findings, most notably the presence of diastolic dysfunction, using both 2-D imaging and TDI assessments, demonstrating the association of diastolic dysfunction with worse outcomes after TIPS and LTx.8,27
Basic 2-D and tissue Doppler indices of diastolic and systolic function
In a recent autopsy study of 133 patients with cirrhosis, cardiomegaly and left ventricular hypertrophy were found in up to 43% of patients. 31 Diastolic dysfunction is common in cirrhotic patients and has been widely reported in many clinical studies, most commonly evaluating abnormalities in E/A ratio.27,32 Using basic 2-D indices of diastolic dysfunction, pulsed-wave Doppler at the mitral valve leaflet tips provides information about early and late diastolic filling in normal sinus rhythm, with rapid passive filling (E-wave) followed by atrial contraction (A-wave). 33 Measurements of E-wave deceleration time, along with measurement of isovolumic relaxation time by pulsed-wave Doppler at the septal insertion of the mitral valve, provide estimates of diastolic parameters and can guide in categorizing patients on the spectrum of diastolic abnormalities using a validated grading system. 33 However, E/A is load-dependent, making its use in cirrhosis problematic, as fluid shift is a prominent physiologic derangement in this condition. Diastolic dysfunction parameters may change based on weight, whether or not measurements were obtained before or after paracentesis, or whether obtained before or soon after other major interventions such as TIPS, which precipitates a marked increase in preload and can precipitate fulminant heart failure from latent or subclinical cirrhotic cardiomyopathy. For these reasons, and despite the 2005 working group definition centered on these parameters, newer investigations are focused on TDI assessments of diastolic parameters (s', e', a'), and using the well-known combined parameter of E/e', which has been associated with increased pulmonary capillary wedge pressure in cardiac patients (although without cirrhosis).33,34 Tissue Doppler indices measure intra-myocardial velocities along the longitudinal axis at the mitral septal or lateral annulus insertion and can quantify regional peak velocities in systole (s'), early diastole (e'), and late diastole or atrial “kick” (a'). TDI is an increasingly attractive modality to assess diastolic dysfunction in the setting of suspected cirrhotic cardiomyopathy given both angle-independence and load-independence. 34
Myocardial Strain Imaging
Echocardiographic strain imaging, also known as deformation imaging, is an increasingly attractive imaging modality used to quantify myocardial dysfunction under conditions of ischemia, dyssynchrony, pressure and volume overload related to valvular heart disease, infiltrative heart disease such as amyloidosis, chemotherapy cardiotoxicity, heart transplant rejection, and more recently in the assessment of cirrhotic cardiomyopathy.35–37 Strain or regional deformation describes lengthening, shortening, or thickening of the myocardium. Strain is expressed as a percent (%) shortening, with more negative values in the longitudinal plane indicating normal myocardial systolic function. Strain can also be expressed as a rate, as thickening or shortening per unit time expressed in milliseconds, although the clinical literature appears to favor strain over strain rate. Strain imaging is currently primarily used as a research tool, but it is increasingly used as a clinical tool, in its most understandable form, as linear or longitudinal strain using apical or long-axis images. Strain measurements can be derived either from post-processing of TDI velocity data or using speckle tracking computer software. 35
Most of the published literature on strain using TDI reports measurements of longitudinal strain from the apical windows, and this is the technique we and others have used for variable assessments of other cardiomyopathies.38–41 Speckle tracking is also a post-processing computer algorithm, which uses grayscale digital images of the myocardium containing speckle patterns, which are then tracked as blocks of pixel movement and analyzed for change in location, thus reflecting tissue movement, and quantified as speckle pixels moving closer or farther apart. Importantly, strain can identify myocardial dysfunction in patients where visually the ejection fraction appears to be normal. Increasingly strain is becoming more understandable in the clinical literature and offers insight into subclinical myocardial dysfunction that is not readily apparent by older, less sensitive echocardiographic indices. Specific to cirrhotic cardiomyopathy, there are a few reports of use of strain in this population. Sampaio and colleagues reviewed 109 cirrhotic patients with an average MELD score of 14, without known significant prior cardiac disease. 37 In addition to basic echocardiographic measurements, 2-D strain assessment using speckle tracking was obtained in the apical four- and two-chamber views and compared with 18 healthy controls. In the cirrhotic group, peak longitudinal strain was lower than in controls and significantly lower in patients with an EF < 55% (-16.73 vs −20.19% P = 0.013). While this study evaluated an overall population of cirrhotic patients arguably not very sick given relatively low MELD scores, it provides an example of the use of strain in this context and serves as a foundation for future papers. Other studies using longitudinal strain in cirrhotic patients were not able to observe significant differences in strain parameters associated with severity of liver disease. 36
Echocardiographic assessment of myocardial energy expenditure
Myocardial energy expenditure (MEE) is a non-invasive estimation of left ventricular workload and biomechanical energy expenditure and may serve as an estimation of myocardial oxygen consumption. MEE is a non-invasive calculation used in research echocardiography, calculated as circumferential end-systolic stress (kdyne/cm2) × ejection time (seconds) × stroke volume (cm3) × 4.2 × 10−7, and is expressed as kcal/systole or cal/minute. 42 If left ventricular mass is also measured, then in combination with MEE, a non-invasive estimation of myocardial oxygen consumption may be obtained and expressed as mL O2/g/minute. Reference values for a healthy cohort without heart disease yield an approximate resting myocardial oxygen consumption of approximately 0.12 + −0.04 mL O2/g/minute and correlate with invasive estimations of the same. 43 While laborious to measure and calculate, this non-invasive echocardiographic assessment of MEE may add to clinical insights into cirrhotic cardiomyopathy, as it has been in the context of pressure and volume overload related to valvular heart disease and hypertension.
Biomarkers
Serial use of biomarkers is an increasingly important strategy for the diagnosis and management of patients with heart failure. BNP and pro-peptide N-terminal pro-peptide BNP (NT-proBNP) are frequently used in distinguishing heart failure as the cause of dyspnea, for serial assessment and medication uptitration, in clinical trials as markers of heart failure severity and for long-term prognosis, particularly in special heart failure populations eg, cardiac amyloidosis.44–48 BNP is secreted from the ventricles in response to volume or pressure overload as a compensatory neurohormone to promote natri- and diuresis in the setting of an activated renin–angiotensin–aldosterone system. 49 BNP has been studied in cirrhotic patients as a surrogate for cirrhotic cardiomyopathy, with recent predictive data regarding incidence of renal failure and mortality after LTx, and its association with MELD scores, severity of cirrhosis, and diastolic or systolic dysfunction.50–52 Increasing BNP levels in the setting of dyspnea, exertional intolerance, and progressive renal dysfunction in cirrhotic patients may alert clinicians to re-assess myocardial systolic and diastolic function, particularly with impending LTx surgery.
Cardiac troponin T and I are thin filament contractile proteins elevated in the setting of myocardial necrosis, with serial measurement of these markers considered standard of care for assessment of acute coronary syndrome. 53 Elevated troponin also occurs under variable conditions of demand ischemia related to myocardial pressure and volume overload, under conditions of myocardial infiltration, and in the setting of high-output heart failure eg, cirrhosis.1,17,54,55 For patients with cardiac amyloidosis, elevated troponin is now part of the prognostic risk-stratification or staging of patients with primary amyloidosis. 56 In the cirrhosis literature, there are numerous reports of elevated troponin associated with severity of liver disease and with adverse outcome after LTx,16,17 with the recognition that myocardial wall stretch and stress unrelated to significant epicardial CAD occurs under the condition of advanced cirrhosis and high MELD scores.
Galectin-3 has recently emerged as a potential biomarker as an index of cardiac fibrosis, and may predict incident heart failure, as recently demonstrated in the Framingham Offspring Cohort. 57 Galectin-3 is a beta-galactoside-binding lectin that mediates cardiac fibrosis, which can be assayed in serum and is found to be associated with acute and chronic heart failure.58,59 Galectin-3 is activated by tissue damage, which is demonstrated in animal models of heart failure. 60 However, galectin-3 is also activated in animal models of liver fibrosis, and is increasingly studied as a marker of cirrhosis, with evidence of regression of liver fibrosis in animal models treated with galectin-3 inhibitors. 61 It is unclear whether circulating galectin-3 from liver fibrosis may be cardiotoxic, thus providing an additional link between progressive cirrhosis and developing cirrhotic cardiomyopathy. Given this potential mechanistic link, for this reason galectin-3 levels may be difficult to interpret with regard to myocardial reserve in this context.
LTX and TIPS
Cardiac evaluation of LTx candidates should follow previously described guidelines, with serial assessment using ECG, TTE, or right heart catheterization based on individual clinical concerns. In a recent report from our institution, we identified over a three-year period 3% (9/298) of LTx patients who developed severe HF after LTx. 62 In these nine patients, etiology of liver failure was hepatitis C with hepatocellular carcinoma in four, hemochromatosis in four (with one showing evidence of iron deposition in the heart on biopsy), and one with primary biliary cirrhosis. Average MELD score at time of transplant was 29.7 ± 8.2. Preoperative ECG showed prolonged QTc averaged at 450 ± 36 milliseconds, EF 58.9 ± 2.4%, with mildly reduced s’ on tissue Doppler of the lateral mitral annulus of 10.8 ± 1.7 cm/second. Intraoperative average transfusion volume was 14.6 ± 5.7 L, with very high average pressor requirements. Post-operatively, average EF was 26.7 ± 12.5% (range 10-45%), with 66.6% showing moderate to severe RV dysfunction and s’ of lateral mitral annulus of 8.8 ± 2.2 cm/second. In six patients, echo imaging was additionally suggestive of Takotsubo cardiomyopathy. 63 Six patients required inotropes and pressors, and two patients required mechanical circulatory support device therapy; venoarterial extracorporeal membrane oxygenation (VA ECMO) and biventricular assist device (BIVAD). Three patients died from heart failure within one month of transplant, with the other six recovering normal cardiac function. In one patient in whom BIVAD therapy was used, global longitudinal strain of the left ventricle was obtained within 6 months and immediately prior to transplant. Interestingly, whereas ejection fraction was 62% and LV strain −39% within 6 months of transplant, just prior to transplant EF was 64%, but LV strain was only −18%. This example illustrates the increased sensitivity of strain imaging in detecting myocardial dysfunction in the absence of overt dysfunction on 2-D imaging. 64 Importantly, in six patients, sepsis or systemic inflammatory response syndrome was presumed, raising the issue whether septic cardiomyopathy and Takotsubo cardiomyopathy are distinct entities of reversible cardiomyopathy, or whether underlying cirrhotic cardiomyopathy increases vulnerability to these events. 65 In another case report of two LTx patients who suffered cardiovascular collapse at time of graft reperfusion, Takotsubo cardiomyopathy-like imaging was demonstrated. 66 Post-reperfusion syndrome is defined by severe hemodynamic disturbances at time of liver graft reperfusion, which can affect up to 30% of LTx patients and can lead to cardiac arrest and death. 67
Advanced Heart Failure Therapies for Myocardial Failure after LTx
Proposed cardiac assessment – initial screening and recommendations for follow up.

For patients who demonstrate clinically significant myocardial failure while on the LTx waiting list, consideration should be given to a combined heart–liver transplantation. Heart–liver transplantation is a viable option with acceptable one- and five-year outcomes, with United Network Organ Sharing (UNOS) policies dictating the combined organ allocation policy. 67
Conclusions and Future Directions
CAC is an important clinical problem. With increasing age and co-morbidities of LTx candidates, concern for clinically important cardiac disease in both the early and later stages of cirrhosis may warrant a more systematic approach in order to avoid adverse outcomes. New imaging modalities and increasing use of biomarkers to elucidate masked cardiac dysfunction may offer novel predictive opportunities to define patients at risk for perioperative cardiac complications. Increased use of temporary support devices may play an increasing role in supporting the acutely failing myocardium in the perioperative period. Finally, prospective, observational studies of serial imaging and biomarkers in the ESLD population are well overdue and should be performed by the transplant community.
Author Contributions
Conceived and designed the experiments: MF, PCS. Analyzed the data: MF, PCS. Wrote the first draft of the manuscript: MF, PCS. Contributed to the writing of the manuscript: MF, PCS. Agree with manuscript results and conclusions: MF, PCS. Jointly developed the structure and arguments for the paper: MF, PCS. Made critical revisions and approved final version: MF, PCS. Both authors reviewed and approved of the final manuscript.
Abbreviations
Brain Natriuretic Peptide
Coronary Artery Disease
Cirrhosis-associated Cardiomyopathy
Dobutamine Stress Echocardiography
Electrocardiography
End Stage Liver Disease
Liver Transplantation
Myocardial Energy Expenditure
Models for End Stage Liver Disease
Myocardial Perfusion Scintigraphy
N-terminal pro-peptide brain naturietic peptide
Tissue Doppler Imaging
Transjugular Intrahepatic Portosystemic Shunt
Transthoracic Echocardiogram