
Abstract
Purpose
The current gold standard of popliteal artery aneurysm (PAA) treatment is saphenous vein bypass grafting. The aim of this retrospective single-center study is to investigate the safety and efficacy in the treatment of PAA by an endovascular implanted covered endoprosthesis.
Materials and Methods
Ten patients, mean age 64.6 (range, 52-78) years, with PAA were treated with an expanded Polytetrafluoroethylen (ePTFE)-covered stent graft (Viabahn®, W.L. Gore and Associates Inc, Flagstaff, AZ, USA). In median, 1.4 prostheses were implanted with a median length of 180 mm. Follow-up visits included determination of ankle-brachial index (ABI) and color-coded duplex sonography.
Results
The technical success rate was 100% (10/10). Clinically, there was an increase in ABI from 0.62 ± 0.17 to 0.91 ± 0.15 postinterventionally and to 0.89 ± 0.16 after an average follow-up of 24.7 months. During the follow-up period, 2 (20%) stent occlusions occurred; both of them were treated with a bypass graft.
Conclusion
The treatment of PAA with covered endoprosthesis is a safe and effective alternative to open surgical therapy, where open surgical therapy is contraindicated or patient refused open surgery.
Introduction
The popliteal artery (PA) represents the second most frequent localization of arterial aneurysms. 1 The PA is considered aneurysmal once the diameter is either 1.5 cm or 1.5 times the size of the normal proximal artery. Popliteal artery aneurysms (PAAs) occur much more frequently in men than in women (20:1 ratio). The incidence rate of PAA increases with age, and approximately one half of PAAs are bilateral. 2 Complicated PAA can cause rupture, distal embolization, and thrombosis, leading to a high risk of limb loss. 3 Although PAA expand at a growth rate of around 10% per year, rupture is rare with an annual occurrence rate of 1.4%. 4
There is a general consensus that all symptomatic PAA should be repaired regardless of size, and asymptomatic PAAs are recommended to be treated if the aneurysm diameter is greater than 2 cm, mural thrombus is present, or the patient has poor runoff. The current gold standard of PAA repair is saphenous vein bypass grafting with either ligation (most common) or endoaneurysmorrhaphy (resection of the aneurysm).4–6
Open surgical repair provides very satisfactory results, particularly in the elective setting. Thus, high rates of graft patency and freedom from amputation during follow-up have been reported. 1 In recent years, PAA exclusion with stent graft has been emerging as a possible alternative to open surgery, particularly in high-risk surgical patients.7–9 Endovascular treatment provides shorter operative times, shorter hospital stays with less perioperative morbidity, and faster recovery.10–12
The objective of this retrospective single-center study is to investigate the safety and efficacy in the treatment of PAA by an endovascular implanted covered endoprosthesis.
Materials and Methods
Patients
Ten patients with aneurysm of the PA were treated interventionally by implanting an ePTFE-covered endoprosthesis (Viabahn®, W.L. Gore and Associates Inc, Flagstaff, AZ, USA). Because of the retrospective nature of this research, ethical approval was not required. The research was conducted in accordance with the principles of the Declaration of Helsinki.
Technical success was defined as a complete restoration of the total length of the aneurysm with a residual stenosis ≤30% at the narrowest point remaining and observation of no endoleak.
All patients were examined prior to the intervention with a color-coded duplex sonography (CCDS) and a computed tomography angiography for intervention planning.
The mean age of the patients was 64.6 (50-78) years. There were nine male patients and one female patient in the study.
Clinical classification was done according to the Rutherford classification, 2 which revealed an average stage of 3.0 (1-4) prior to the intervention. Nine PAAs were symptomatic, only one PAA was asymptomatic. One patient had a critical ischemia at the time of treatment, the other eight patients had a mild (n = 5) or severe (n = 3) claudication.
Prior to treatment, all cases were discussed in a multidisciplinary board with vascular surgeons taking into account the comorbidities as well as the patient's wish for an interventional treatment; stent implantation was recommended in all cases.
The main inclusion criterion was an aneurysm of the PA. Also, there had to be at least one peripheral downstream artery present. Furthermore, an intraluminal wire passage of the lesion had to be achieved.
The intervention was performed in 10 patients (100%) using antegrade technique.
Intervention
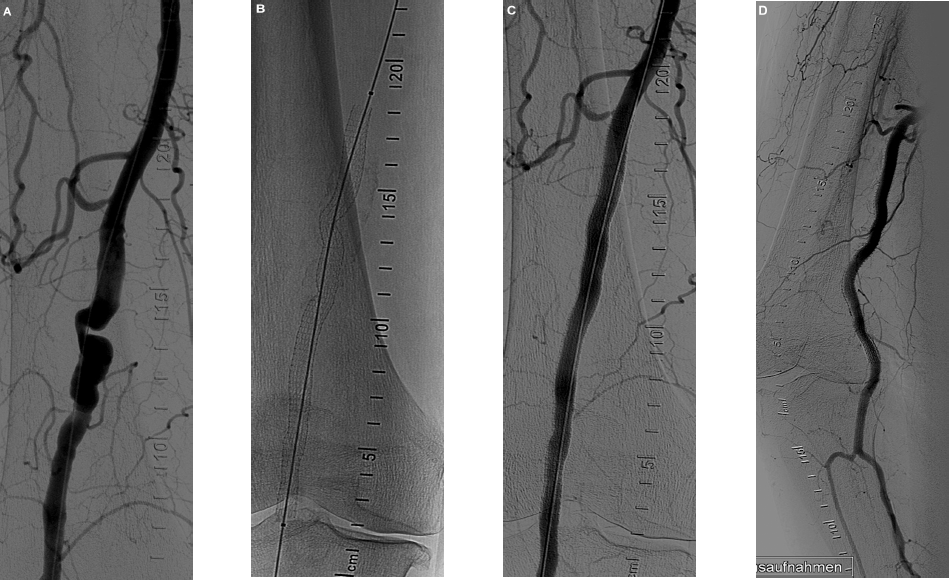
After completing an angiography using the standard technique, the nominal vessel diameter was estimated in the target lesion and a suitable stent graft was selected. According to the manufacturer's instructions, we select at least 2 cm of non-aneurysmal popliteal or superficial femoral artery (SFA) to serve as the proximal landing zone and at least 2 cm of non-aneurysmal PA to serve as the distal landing zone. The endograft(s) should exclude all mural thrombus from the arterial lumen. When treating PAA with multiple devices, it is recommended that there is at least 2 cm of overlap to minimize the risk of migration and endoleak. If unequal device diameters are used, the smaller device should be placed first and then the larger device should be placed inside of the smaller device. Depending on the caliber of the endoprosthesis, either a 6- or 7-F sheath was used. Then, a 0.018″ or 0.035″ hydrophilic-coated guide wire was passed through the lesion under the guidance of a roadmap display. After this, 5,000 IU heparin unfractionated heparin (UFH) was administered. The device must be deployed relatively slowly to prevent deployment inaccuracy. It is recommended to watch on fluoro as the device opens to ensure safe and accurate deployment. After implantation, the catheter was withdrawn and a control angiography was conducted. Postdilatation was performed by pressure only balloon angioplasty (POBA). The size of the balloon depends on the diameter of the implanted endoprosthesis (Figs. 1 and 2).

(
(
Finally, any residual stenosis >30% was treated with prolonged POBA. Hemostasis was achieved in all patients using a suture-mediated closure device (Perclose ProGlide; Abbott Vascular) in preclosure technique and an additional compression bandage.
Medication
All patients received acetylsalicylic acid (ASA) 100 mg/day prior to the intervention unless long-term medication had already been established. About 5,000 IU heparin was given intra-arterially during the intervention. Long-term ASA therapy (100 mg/day) was given post-interventionally. An additional dose of clopidogrel (Sanofi Aventis, Germany) 75 mg/day was given for a minimum of 6 weeks after a loading dose of 300 mg.
Follow-up
All patients were routinely followed-up before discharge and after 3, 6, 12, and 24 months by clinical examinations, standard treadmill ergometry, determination of the ankle-brachial index (ABI), and a CCDS.
Results
The technical success rate was 100% (10/10). In all patients, the angiography showed a patent PA with a residual stenosis of ≤20% after placement of the endoprosthesis. No endoleaks were observed (Table 1).
Interventional characteristics and results of the 10 patients.

The mean diameter of the treated aneurysm was 26.7 mm (19-36 mm). The mean length of treated aneurysm was 139.6 mm (90-210 mm). In median, 1.4 endoprostheses were implanted with a median length of the covered artery of 180 mm.
The inflow vessels of the endoprosthesis were SFA in seven patients and PA in three patients. In all patients (10/10), the outflow vessels were the distal third of the PA.
We had a median of 2.1 patent runoff vessels (1-3).
The average hospital stay endured 3 days (1-6).
Hemodynamic success is reflected by a significant improvement in ABI from 0.62 ± 0.17 before the intervention to 0.91 ± 0.15 at discharge to 0.89 ± 0.16 after 24 months (P < 0.05).
There was a clinical improvement in the Rutherford stages, from 3.0 prior to the procedure to 1.2 after 24 months.
During follow-up examinations, two reocclusions were observed (20%). In one patient, the reocclusion occurred one month after the intervention, and in the other patient, it occurred three months after the intervention. Both patients were successfully treated with a femoropopliteal bypass graft. No further stenoses or occlusions of the endoprosthesis were observed.
Complications
There were no perforations, distal embolisms, arterio-veneous (AV) fistulas, or pseudoaneurysms. There were no amputations or deaths during the 24 months follow-up period.
Discussion
In order to put our results into the context of the relevant literature, we performed a comprehensive PubMed research regarding the topic of endovascular treatment of PAAs. We included only recent studies from 2006 onward, which fully or partially used the same device as in our investigation.
The graft we used was an ePTFE-covered Viabahn stent graft, which is a modification of the Hemobahn stent graft. It provides more flexibility and is self-expanding. Besides Viabahn and Hemobahn stent grafts, data are published about wallgrafts 13 and multilayer stents.14,15
Peripheral artery aneurysms are mostly caused by a decrease in distensibility of the arterial wall due to arteriosclerosis. In the minority of cases, local trauma and infection can also be the underlying pathogenesis. A significant number of these aneurysms are asymptomatic and therefore not detected or detected by chance. About 80% of our patients had a symptomatic PAA (Rutherford II and III). This percentage is higher when compared with other studies. Only Idelchik et al treated 100% symptomatic patients, 16 whereas others reported about 35-46%.9,17,18
Regarding peripheral artery aneurysms, the lower limb is prone to aneurysm development. The most frequent subtype applies to the PA with an incidence rate of 0.1-2.8%. 19
PAAs are often bilateral or seen in combination with aneurysms of other location. There is a gender preference for male patients with a ratio of 20:1.
Incidence rate increases with age. Our patients were relatively young with the mean age of 64.6 years when compared with those in other studies (68-76 years).9,16,17,20
As in all other aneurysms, PAA implicates the risk of covered or open rupture, local compression of passing nerves and veins (with the risk of DVT), and acute or chronic ischemia. Because of recurrent flexion and extension of the knee joint, the artery resides in a disadvantageous localization for treatment.
Asymptomatic PAA smaller than 2 cm in diameter can usually be treated conservatively in surveillance with duplex sonography. The outcome of an interventional therapy is better in asymptomatic patients than that in symptomatic patients. 21 If the diameter is more than 2 cm, if it is causing claudication, or if a thrombotic seam is existent, nonconservative treatment is recommended. There are two strategies for treatment.
On the one hand, there is the traditional open surgery, which is performed by ligation and bypass with autologous vein or prosthetic graft. On the other hand, there is an alternative to an endovascular approach whose experience is rapidly increasing since the first implantation in 1994. Patient selection requires the evaluation of an adequate access vessel in the groin, proximal, and distal landing zones of non-enlarged diameter of 2 cm both and distant pulses. At least one lower limb artery must be patent. Nevertheless, results are better with a 2- or 3-vessel runoff. 9
We added our data from a retrospective single-center study like most of the authors from recent comparable literature, although there are only a few prospective single-center studies11,16 and retrospective multicenter studies.13,22 Collecting data in multicenter studies is mandatory especially to solidify knowledge about the topic.
We had a relatively small number (10) of PAAs treated with endovascular stenting compared with other studies that treated 24-178 patients.9,18,20,22,23 Naturally, this is a limitation of our validity.
Concerning the average aneurysm diameter, we measured 28 mm and are in the range of other studies that had 2-3.7 cm.9,11–13,16,18,20,22,24,25 Our average aneurysm length was 13.9 cm, and therefore, slightly longer than that in the literature (9.9-10 cm).4,9
The stents could be deployed with a 7-F or smaller sheath. They were oversized 10% in axial diameter to reach the optimal adaptation and to reduce the risk of endoleaks. Our technical success rate was 100%, which includes that no complications like endoleaks, access site hematomas, and infections occurred. Technical success in all cases was also reported by several authors of the literature we are referring to.17,20,22,23
If the proximal and distal landing zone differed more than 4 mm, we used overlapping variable-sized grafts with an overlap zone of at least 2 cm. If overlapping was necessary, the distal stents were implanted first. Consequently, we used an average of 1.4 stent grafts, which is less than that in other publications (1.9-2 stents),9,16,22 and covered an average of 18 cm. The last point is in the range of comparison with the literature (15-20 cm).16,18,20,22
Possible complications after endovascular repair of PAA comprise all types of endoleaks, including a backflow of blood via geniculate vessels into the aneurysmal sac, a complication that is similar to type 2 endoleaks after abdominal aortic aneurysm repair. In our study population, no endoleaks occurred, and they were also rare (0-20%) in other studies.11–13,24,25 Access site hematoma is a potential risk similar to angiography, in general, but we did not have this complication either. When graft occlusions occur, they are mostly seen in the first year. Thus, follow-up should be more intensive in this period. We observed two stent occlusions (20%) after 1 and 3 months. In the literature, we found stent occlusion rates of 9-20%.9,16–18,20,22 Stent fractures were not seen in our patients and they seem to be generally rare (0-16.7%).11,25 When reported, active and young patients are affected, especially in overlapping stent zones.
We have seen our patients for a mean follow-up of 24.7 months, and therefore, consider our observations as early results since most of the other authors reported from longer follow-ups of 22-72 months.9,16–18,20,22,23 Follow-up modalities were duplex ultrasound and the ABI. ABI increased from 0.62 before to 0.91 after intervention and was 0.89 after 2 years. Idelchik et al also used the ABI in the follow-up and observed a significant increase after 6 months and a slight decrease after 1 year. 16
The overall primary patency of the stent graft after 1 year was 80%. However, in the majority of our reference literature, it was even better (80-100%).9,11–13,16–18,20,24,25 The explanation might be that we had a very high percentage of symptomatic patients (80%), especially 40% patients with a Rutherford III stadium. Our primary patency after 2 years was still 80% since no further graft failures occurred. In the reference literature, we found a range of 85.5-90% after 2 years,9,13 63.7-86% after 3 years,13,18 86% after 4 years, 13 82-84% after 5 years,12,17 and 81% after 6 years. 22
In general, stent occlusions can be treated either by intra-arterial lytic therapy and endovascular reintervention or surgically. Together with the vascular surgery department, we decided to perform bypasses. Thus, we cannot discuss a secondary patency of endovascular treatment but other authors reported promising secondary patency rates of 85-90%.17,22
After endovascular intervention and surgical re-intervention with bypass, our limb salvage rate was 100%. Several other authors reported about high limb salvage rates using endovascular stents between 94 and 100%.9,11–13,18,22,24,25 The surgical approach also provides high limb salvage rates of 80-95%. Considering the differences in the length of follow-up and the fact that there is much more data about the surgical approach, we think that both methods provide comparably good prognoses. This claim is supported by the work of Galiñanes et al, who compared the outcome of endovascular and open repair of PAA in 2962 patients. 26 They found that complication rates did not differ significantly. In addition, no difference was observed in the 30- and 90-day mortality rate. Several further researches did not find a statistically significant difference in patency neither.11,12,18,25
Antiplatelet therapy is an important factor of the postinterventional course. In our department, we have good experiences with a scheme including 48 hours of full-dose heparin, clopidogrel 75 mg for at least 6 weeks, and lifelong ASA. Other reported schemes comprise combinations of clopidogrel and ASA,11,13,25 clopidogrel and/or ASA, 17 and only clopidogrel.12,24
In summary, if we obey inclusion criteria, endovascular treatment of PAA with a stent graft like the Viabahn prosthesis is a good alternative to bypass surgery where open surgical therapy is contraindicated or patient refused open surgery. It is a fast and safe procedure with minimum blood loss that does not require general anesthesia. Especially, elderly patients with cardiopulmonary risk factors could benefit from a faster discharge from the hospital, avoiding nosocomial complications like infections and immobility.11,12,26 Endovascular treatment is not suitable for patients with severe thrombosis, poor distal run off, highly angulated vessels, and in the presence of a longrange ectactic femoropopliteal artery.
In the case of a stent occlusion, intra-arterial lytic therapy and endovascular re-intervention or bypass surgery are still possible.
Author Contributions
Conceived and designed: CW, CL, RA. Analyzed the data: CW, FS, ES. Wrote the first draft: CW, HV. Contributed to the writing: CL, FS, ML, RA. Agree with the manuscript: CW, CL, HV, FS, ML, ES, RA. Developed the structure: CW, FS, HV, ML. Critical revisions: HV, ES, RA. All authors reviewed and approved of the final manuscript.