
Abstract
Objective
The rotational atherothrombectomy with Straub Rotarex® is a safe and efficient treatment of acute/subactute vascular occlusions. The purpose of this study was to evaluate the benefit of paclitaxel-coated angioplasty after rotational atherothrombectomy over an observation period of six months.
Materials and Methods
Overall, 29 patients were treated with the Rotarex catheter in combination with paclitaxel-coated angioplasty. All patients had acute/subacute and chronic occlusions of the superficial femoral artery (SFA) and/or popliteal arteries. The ankle-brachial index (ABI) was detected before the intervention, after the procedure, and after six months. Also clinical examination and ultrasound scans were done in the observation period.
Results
There were no technical failures. The ABI shows a significant increase from 0.52 ± 0.17 to 0.91 ± 0.25 in the follow-up. By ultrasound examination, there were found two (6.9%) restenoses during the follow-up. There was one dissection during the intervention (3.5%).
Conclusion
The rotational atherothrombectomy in combination with paclitaxel-coated angioplasty might be an effective and safe method with a promising low rate of restenosis at six months.
Introduction
Mechanical rotational thrombectomy devices can be utilized as a safe and effective alternative in the treatment of acute or subacute infrainguinal occlusions and chronic occlusions of the iliac and femoropopliteal arteries. The limitation of rotational thrombectomy with Rotarex® catheter (Rotarex, Straub Medical AG, Wangs, Switzerland) is that there is no treatment possible in the infrapopliteal artery.1,2 Laser atherectomy, 3 the SilverHawk™ atherectomy catheter, 4 and the pathway atherectomy system are other atherectomy devices with promising results in initial trials.4,5 The comparatively high restenosis rate is the main problem with treatment of arterial stenosis and occlusions. To raise the patency rate after arterial intervention, a lot of methods have been developed. In randomized trials, the stent implantation has demonstrated an advantage over percutaneous transluminal angioplasty (PTA) alone. However, this benefit was not always significant. 6 Stents coated with different drugs to reduce the restenosis rate are interesting approaches. 7 The objective of this study is to investigate the combination of mechanical rotational catheter system and Paclitaxel-coated balloon angioplasty for femoropopliteal occlusion.
Materials and Methods
Patients
In this single center, retrospective study, 29 patients with acute/subacute or chronic occlusions of the superficial femoral artery (SFA) or popliteal artery (PA) were included. This study was exempt from the requirement for ethics committee approval because patients received standard treatment and the study constituted a retrospective review of their records. In our institute, the interventional strategies are primary methods. All patients were treated using the Rotarex catheter and drug-eluting balloons (DEBs; IN.PACT™ Pacific or IN.PACT™ Admiral Medtronic, USA). The risk profile, clinical classification according to the Rutherford classification, 8 and the pattern of occlusions are demonstrated in Table 1. Before treatment, after procedure, and after six months, all patients' data were recorded by clinical investigation and documented by Rutherford stage, standard treadmill ergometer, and designation of the ankle-brachial index (ABI). To exclude reocclusions, additional ultrasound examinations were carried out. To plan the treatment, either a color-coded duplex sonography (CCDS) or a CT-/MR-angiography was carried out. Inclusion criteria were de novo occlusions and reocclusions of untreated vessels. Leastways, one peripheral downstream artery had to be presented. Then an intraluminal wire passage of the occlusion had to be established. An ipsilateral access was used in 27 patients (93%), and in 2 patients (7%), the cross-over technique was used. In 90% (n = 26) of patients, recanalization was done with Rotarex 6F device. In three cases (10%), the intervention was performed with Rotarex 8F system. DEBs of different sizes were used according to the vessel diameters. Technical success after atherothrombectomy and DEB use was defined as complete recanalization of the occlusion with a residual stenosis ≤50%.
Patient Characteristics*.

Reported as mean ± SD, or n/N (%).
Mechanical rotational catheter system (Straub Rotarex)
The Rotarex system was described in prior trials. The working principal is the Archimedes screw with a rotating inner helix and even rotating head of the catheter (1, 2).
DEB (Paclitaxel) catheter
The paclitaxel-eluting PTA balloon catheters (IN.PACT Pacific and IN.PACT Admiral) are over the wire (OTW) peripheral balloon catheters, specifically designed for PTA in atherosclerotic vessels. The catheter has a dual lumen shaft, one central lumen for the guide wire and a second tube used to inflate and deflate the balloon. The length and size of each balloon is specified; the maximum guide wire diameter for Pacific™ is 0.018 inch (0.46 mm) and the maximum guide wire diameter for Admiral is 0.035 inch (0.89 mm). IN.PACT Pacific and IN.PACT Admiral are DEB coated with Paclitaxel (3 μg/mm3 balloon surface) and urea as hydrophilic natural spacer. 9
Intervention
First of all, 5,000 IU heparin (UFH) were given intra-arterial. The caliber of the Rotarex catheter for the target lesion was selected after implementation of angiography using a standard technique. According to the instructions for use, a vessel diameter up to 5 mm has to be treated with the Rotarex 6F catheter. For lesions with a vessel diameter of 5-8 mm, a Rotarex 8F catheter has to be used. Vessels less than 3 mm cannot be treated by Rotarex. The upper limit is a vessel diameter of 8 mm. First, the occlusion was probed with a hydrophilic-coated guide wire (Terumo stiff, 0.035 inch). Then a 0.018 inch hydrophilic and Teflon-coated guide wire was placed via a straight 4F catheter. Above the target lesion, the tip of the Rotarex catheter was placed and the complete occlusion was passed with alternating forward and backward movements. After this procedure and complete passage of the target lesion, a control angiography was obtained. A maximum of three passages with the Rotarex catheter were conducted (mean 2.0 ± 0.6; range 1-3). Finally, a PTA with DEBs of different sizes was accomplished. Therefore, the recumbent guide wire was used. The time of deflation was three minutes. The technical success after intervention was defined as treated target lesion with a residual stenosis <50%. After the femoral artery angiographic procedures, the puncture site was closed with hemostasis devices. Distal protection devices were not used generally (Fig. 1 and Fig. 2).

Preinterventional angiogram of a chronic total occlusion of the SFA (

Preinterventional angiogram of a acute total occlusion of the femoropopliteal artery (
Medication
Our patients received acetylsalicylic acid (ASA) 100 mg/day before intervention. During the intervention, each patient was given 5,000 IU heparin. After treatment, the ASA therapy (100 mg/day) was continued as a permanent therapy. For six weeks, a dose of 75 mg of clopidogrel/day was also given. After intervention, a loading dose of 300 mg of clopidogrel was administered. For each patient, a full heparinization for 48 hours was conducted.
Results
The technical success of rotational atherothrombectomy and DEB–PTA was 100% (Fig. 2). A significant increase in the ABI from 0.52 ± 0.17 prior to the treatment to 0.89 ± 0.18 after intervention demonstrated a hemodynamic success. In the follow-up after six months, the ABI increased to 0.91 ± 0.25 (Fig. 3). The improvement of Rutherford stage showed a raise in clinical conditions (Table 2). The treated lesion length was 16.2 ± 8.5 cm (5-35 cm). The period of rotational atherothrombectomy was 5 ± 2.3 (1-15) minutes. In the middle, 2.2 ± 0.67 (1-3) passages were accomplished. On average, 108 ± 41.2 mL (50-200 mL) were aspirated. After Rotarex atherothrombectomy and PTA with IN.PACT Pacific with different lengths and sizes (Table 2), 26 patients (89.7%) showed a residual stenosis of ≤30%. In the middle, 1.8 DEB/patient were used. These patients required no further therapy. In three patients (10.3%), a stent implantation was necessary because of a residual stenosis of 50% or dissection (Table 2). In the follow-up, no in-stent restenosis was documented by ultrasound examination. In the follow-up examinations, two high-grade restenoses (6.9%) were documented by clinical investigation and ultrasound scans. These were successfully treated by repeat PTA.

Improvement of the ABI values over a period of six month. The increase is significant over the entire period of observation (P < 0,001).
Target lesion characteristics*.
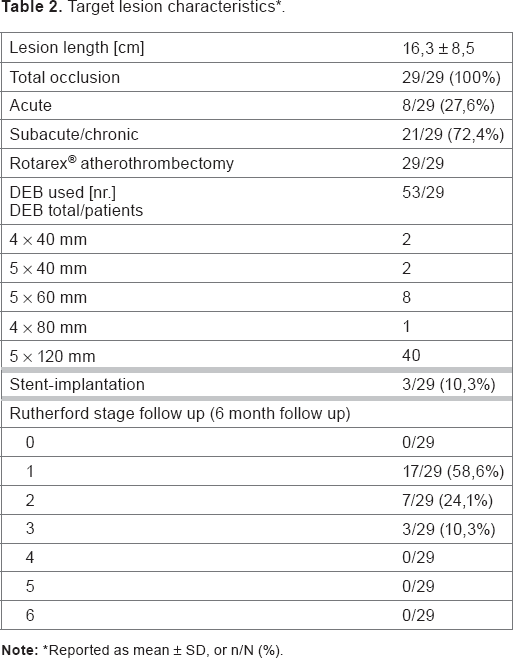
Reported as mean ± SD, or n/N (%).
Complications
There were no perforations. Arteriovenous fistulas, distal embolisms, and pseudoaneurysms were not observed. In one case, a dissection occurred during the procedure. This complication was treated by PTA and stent implantation. Therefore, the rate of complications was 3.5%. There were no amputations. Two patients died during the six-month follow-up period.
Discussion
We investigated the clinical outcome of a mechanical rotational thrombectomy catheter in combination with paclitaxelcoated angioplasty for the therapy of acute/subacute or chronic vascular occlusions. In varying studies, the Rotarex catheter system has proved its efficiency in the therapy of acute and subacute occlusions.1,10
Important reasons for repeated PTA are restenosis and reocclusions after balloon angioplasty or stent implantation. Restenosis can occur in 40-60% of patients.6,11 The most common cause for the formation of restenoses is intimal hyperproliferation. The reason for this problem seems to be barotrauma that occurs during the PTA. Further elastic recoil and remodeling are reasons for restenosis.12,13 Regardless of all the technological progresses in balloons, the high rate of restenosis is problematic.11,14
The THUNDER study concluded that the rate of restenosis in the six-month follow-up could be reduced if paclitaxel-coated balloon catheters are used. 15 The PACIFIER trial implied similar results with significant reductions of restenosis in the follow-up after femoropopliteal PTA. 9 In our study, just two restenoses were discovered in the six-month follow-up. Until expansion, the paclitaxel adheres to the balloon catheters. The drug released during the inflation of the balloon is taken up by the vessel wall. 16 Therefore, a DEB can only be used once.
Another risk factor for percutaneous intervention is the development of thrombosis or a delayed endothelialization. In particular, this trouble occurs if agents like paclitaxel are used for prevention of restenosis. 15 According to present literature, we prescribe clopidogrel for all patients to prevent thrombosis. In our patients, no thrombotic or embolic incidents were seen.
Restenosis rate after Rotarex atherothrombectomy in acute and subacute occlusions of femoropopliteal arteries was specified between 18 and 54%.1,11,17,18 In this study, a significantly lower rate of restenosis was noted (6.9%) after six months. Therefore, the combination of Rotarex atherothrombectomy and DEB–PTA might be better. A porcine overstretch model showed a reduction of intimal hyperplasia after the intra-arterial exposure of paclitaxel. 19 After treatment with paclitaxel-coated balloon catheters in in-stent restenosis of coronary arteries, a significant reduction in incidence of restenosis was noted. 20 In a randomized trial between conventional angioplasty balloon and DEB, Fanelli et al described a benefit of DEB–PTA. There was a significant improvement of ABI and Fontaine stage after DEB–PTA vs angioplasty with a conventional balloon. Major adverse events after PTA with a conventional balloon were significantly higher than DEB–PTA. 21 Similar results were described by Scheinert et al in the LEVANT I trial that postulated a prevention of femoropopliteal restenosis after PTA with paclitaxel-coated balloon. 22 Another possibility of directional atherectomy is the SilverHawk atherectomy catheter. A technical success rate of 96% was reported by Zeller et al. 4 The restenosis rate of SilverHawk atherectomy after six months was 22%. They concluded that an additional balloon angioplasty might be necessary in selected cases. 4
Distal embolic protection is a very important tool for directional atherectomy. The DEFINITIVE Ca(++) trial investigated the safety and effectiveness of directional atherectomy and distal embolic protection of treatment of calcified femoropopliteal disease. 23 The results demonstrated that the atherectomy devices (SilverHawk and TurboHawk™) are safe and effective in treatment of moderate to severely calcified lesions in femoropopliteal arteries. They support the use of distal embolic protection device (SpiderFX™). A permanent negative pressure inside the Rotarex device is beneficial for the system. Thereby, the thrombotic material can be aspirated into the cutting window of the catheter. There, the material is crushed and transported via a screw conveyor into a collection bag.1,2 There are no interruptions necessary for cleaning the protection device, and a continuous workflow of atherectomy is guaranteed.
The complication rate in our patient collective (3.5%) is comparable with that of other atherectomy studies.3,18,23 The complication in our study group (n = 1) could be treated during the intervention.
The benefits of other directional atherectomy devices in combination with paclitaxel-coated balloon catheters have to be investigated in other studies. Also long-term results are necessary for a final evaluation of rotational atherothrombectomy in combination with paclitaxel-coated balloon catheters.
The price of the Rotarex system is comparable to that for SilverHawk atherectomy or laser angioplasty. The costs of the Rotarex system and the use of paclitaxel-coated balloon catheters can be covered within the German DRG system, which is relevant for us. 24 The use of atherectomy systems in combination with DEB means initially higher costs than PTA or stent-assisted PTA. We think that by the use of both systems in combination, the rate of restenosis could be reduced. Thus, the higher costs of procedure can be justified.
Conclusion
The use of the Rotarex system for the atherectomy of acute/subacute and chronic occlusions of femoropopliteal arteries in combination with paclitaxel-coated balloon catheters is safe and effective. The DEB seems to be a prevention of restenosis at the six-month follow-up.
Author Contributions
Conceived and designed the experiments: CW, FS, CWL. Analyzed the data: FS, PW. Wrote the first draft of the manuscript: FS. Contributed to the writing of the manuscript: FS, CW, CWL, PK. Agree with manuscript results and conclusions: FS, CW, CWL. Jointly developed the structure and arguments for the paper: FS, CW, PK. Made critical revisions and approved final version: RA, HV, ES, ML. All authors reviewed and approved of the final manuscript.