
Abstract
Left ventricular (LV) hypertrophy is an important predictor of morbidity and mortality in hypertensive patients, and its geometric pattern is a useful determinant of severity and prognosis of heart disease. Studies on LV geometric pattern involving large number of Nigerian hypertensive patients are limited. We examined the LV geometric pattern in hypertensive patients seen in our echocardiographic laboratory. A two-dimensional, pulsed, continuous and color flow Doppler echocardiographic evaluation of 1020 consecutive hypertensive patients aged between 18 and 91 years was conducted over an 8-year period. LV geometric patterns were determined using the relationship between the relative wall thickness and LV mass index. Four patterns of LV geometry were found: 237 (23.2%) patients had concentric hypertrophy, 109 (10.7%) had eccentric hypertrophy, 488 (47.8%) had concentric remodeling, and 186 (18.2%) had normal geometry. Patients with concentric hypertrophy were significantly older in age, and had significantly higher systolic blood pressure (BP), diastolic BP, and pulse pressure than those with normal geometry. Systolic function index in patients with eccentric hypertrophy was significantly lower than in other geometric patterns. Doppler echocardiographic parameters showed some diastolic dysfunction in hypertensive patients with abnormal LV geometry. Concentric remodeling was the most common LV geometric pattern observed in our hypertensive patients, followed by concentric hypertrophy and eccentric hypertrophy. Patients with concentric hypertrophy were older than those with other geometric patterns. LV systolic function was significantly lower in patients with eccentric hypertrophy and some degree of diastolic dysfunction were present in patients with abnormal LV geometry.
Introduction
One of the most important individual risk factors for cardiovascular disease (CVD) is hypertension. 1 Left ventricular hypertrophy (LVH), which is defined as an abnormal increase in left ventricular (LV) mass, is one of the organic processes resulting from hypertension. 1 LVH has been widely documented to be an independent cardiac risk factor in hypertensive patients,2,3 and the structural classification of LV geometry also provides useful and additional prognostic information.4,5 Some authors6,7 have observed that age significantly affects LV structure and geometric patterns.
The LV adaptation to hypertension takes four different geometric patterns using the combinations of left ventricular mass index (LVMI) and relative wall thickness (RWT). The heart may adapt to hypertension by developing concentric hypertrophy (CH) with increased LVMI and RWT, eccentric hypertrophy (EH) with increased LVMI and normal RWT, concentric remodeling (CR) with normal LVMI and increased RWT, or by retaining normal geometry (NG) with both normal LVMI and RWT. Each geometric pattern is associated with a distinct combination of pressure and volume stimuli, contractile efficiency (reduced in those with concentric hypertrophy and concentric remodeling), and prognosis (worst with concentric hypertrophy and best with normal geometry).8,9
In Nigeria, studies on LV geometric patterns10–13 involving large number of hypertensive patients are limited and there is little information regarding the association between age and geometric patterns in hypertensive Nigerians. We therefore present an eight-year echocardiographic study of LV geometric patterns of 1020 consecutive hypertensive patients seen at the Cardiac Care Unit of Obafemi Awolowo University Teaching Hospitals Complex (OAUTHC) Ile-Ife, a tertiary hospital in Southwest Nigeria. This study will further help define the pattern of LV geometry in hypertensive subjects in our environment, as well as add to the national and global database.
Materials and Methods
Two-dimensional, pulsed, continuous, and color flow Doppler transthoracic echocardiography was performed on 1020 consecutive hypertensive patients between 2002 and 2010 with Siemens Sonoline G 60s using standard procedures.14,15 The left ventricular mass was derived using the Devereux modified ASE cube formula: 16

Upper normal limits for LV mass index were 134 and 110 g/m2 in men and women respectively.13,17 Relative wall thickness (2 X posterior wall thickness/LV diastolic diameter) was calculated. A partition value of 0.45 for relative wall thickness was used for men and women.13,18
Demographic parameters of patients were recorded. Weight was measured using a standard weighing scale, while height was measured using a stadiometer. The body mass index was derived by dividing the weight (in kilograms) by the square of the height (in meters).
Patients were considered hypertensive if they had a resting systolic blood pressure (SBP) > 140 mmHg and/or diastolic blood pressure (DBP) > 90 mmHg measured after at least 15 minutes of rest in the sitting position with an Accosson mercury sphygmomanometer and adapted cuff at the brachial artery or if they were on antihypertensive therapy. 19 Korotkoff phase 1 was used for SBP and phase 5 for DBP. Three consecutive measurements were performed at 5-min intervals and the mean values for SBP and DBP were noted. Hypertensive patients with heart failure, myocardial infarction, renal failure, and cerebrovascular diseases were excluded from this study. The patients gave their informed consent before participating in this study and ethical clearance was obtained for the study from OAUTHC Ethics and Research Committee.
Statistical analysis
SPSS software version 16.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Categorical variables were expressed as proportions and percentages, while continuous variables were expressed as mean ± SD. Categorical variables were compared using chi square. Analysis of variance (ANOVA) was used to determine the significant differences of the studied parameters among the four groups of LV geometric pattern. Multiple comparisons between the 4 groups were performed by one—way analysis of variance with the Duncan post hoc test. The level of statistical significance was P < 0.05.
Results
Of the 1020 hypertensive patients seen, 568 (55.7%) were male and 452 (44.3%) were female, with a male to female ratio of 1.3:1. The mean age was 57.78 ± 12.87 years (range 18 to 91 years). The demographic characteristics of hypertensive patients are shown in Table 1. The average body mass index (BMI) of the patients was 27.03 ± 5.34 with the mean systolic and diastolic blood pressure of 143.74 ± 21.94 and 87.98 ± 12.80 respectively.
Demographic characteristics of hypertensive patients.
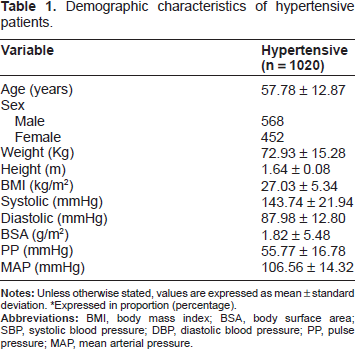
*Expressed in proportion (percentage).
Table 2 shows the demographic characteristics of different LV geometric patterns in hypertensive subjects. 237 (23.2%) patients had concentric hypertrophy, 109 (10.7%) had eccentric hypertrophy, 488 (47.8%) had concentric remodeling, and 186 (18.2%) had normal geometry. Patients with concentric hypertrophy were older than those with other geometric pattern. They also had significantly higher SBP, DBP, mean arterial pressure, and pulse pressure than those with normal geometry.
Demographic characteristics of the different left ventricular geometric patterns.

P-value < 0.05;
P-value < 0.01;
P-value < 0.001 vs. normal geometry).
Table 3 shows the echocardiographic parameters of different LV geometric patterns in the patients. The mean LV internal diameter in diastole was significantly higher in patients with eccentric hypertrophy compared to other geometric patterns. The left atrial dimension was significantly higher among those with concentric and eccentric hypertrophy compared to those with normal geometry. Patients with eccentric hypertrophy had statistically significant lowest indices of systolic function (ejection fraction and fractional shortening) compared to other geometric patterns. The Doppler echocardiographic parameters showed some degree of diastolic dysfunction in hypertensive patients with abnormal LV geometric patterns. Such parameters included the E/A ratio, deceleration time (DT), and isovolumic relaxation time (IVRT), and patients with concentric hypertrophy showed significant differences in all these three parameters compared with those with normal geometry.
Two-dimensional and Doppler echocardiographic characteristics of different geometric patterns in hypertensive subjects.
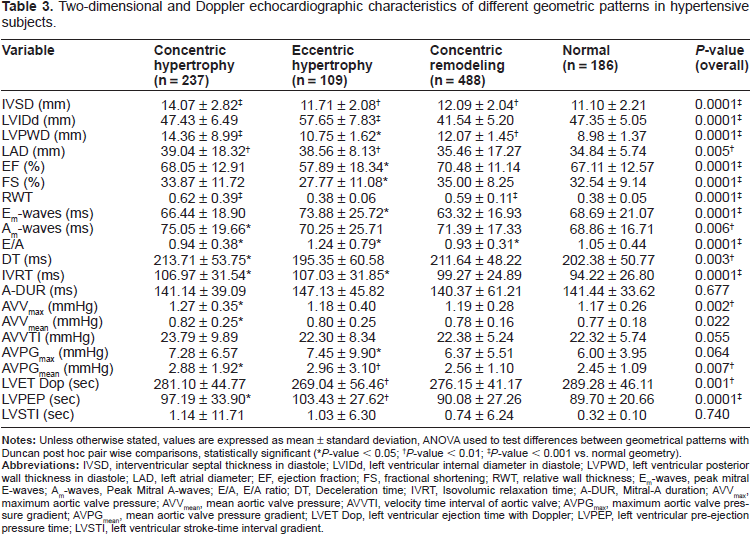
P-value < 0.05;
P-value < 0.01;
P-value < 0.001 vs. normal geometry).
Discussion
With hypertension, the cardiovascular system adapts to neuro-humoral and hemodynamic variations, which may lead to the development of different LV geometric patterns, each carrying a different risk profile for major adverse cardiovascular events. 20
LV hypertrophy is a powerful independent predictor of morbidity and mortality in hypertensive patients. 21 Our results showed that concentric remodeling was the most common LV geometric pattern, followed by concentric hypertrophy, which agrees with the findings of Wang et al 22 and Fox et al. 23 Akintunde et al24,25 and Adamu et al 12 also reported that concentric remodeling and concentric hypertrophy were the predominant LV geometric patterns among their studied population of Nigerian hypertensives.
In a study in Texas, USA, eccentric hypertrophy was the most common LV geometric pattern in hypertensive patients with LVH and with or without clinical evidence of coronary artery disease. 26 The least common LV geometric pattern found in our study was eccentric hypertrophy, which agreed with the findings of other studies conducted within11,12 and outside of22,23 Nigeria. Environmental factors, ethnic differences, and genetic variability may have contributed to the differences in geometric patterns. 10 The link between genetics, ethnicity, and hypertension may therefore involve environmental factors.27–29
According to the paradigm of compensatory ventricular response to a chronic pressure overload, ventricular wall thickness should increase proportionally to blood pressure level to maintain normal wall stress. 30 However, LV adaptation to hypertension has been shown to be more complex than expected. 31 Concentric hypertrophy, one of the patterns of remodeling, is thought to ultimately progress to left ventricular dilatation and failure in hypertensive. It portends poor prognosis and the greatest risk of cardiovascular events. 4 Concentric hypertrophy was also associated with the highest mortality in hypertensive patients 23 and carried the greatest stroke risk, followed by eccentric hypertrophy. 32 Milani et al 33 in the Ochsner studies reported an increased cardiovascular risk associated with concentric hypertrophy and concentric remodeling. Concentric remodeling and concentric hypertrophy may predominate in “early” and “intermediate” hypertensives due to the predominating pressure overload whereas eccentric hypertrophy progressively takes over with increased LV mass due to increases in volume overload. 31
In our study, patients with concentric hypertrophy were significantly older than those with normal geometry, which is similar to the findings of previous studies.6,7,34 We also found that systolic function was significantly lower in patients with eccentric hypertrophy compared to those with normal geometry and concentric hypertrophy, which was similar to other findings.11,23,35
We also observed enhanced longitudinal LV function and augmented EF with increasing degrees of concentric remodeling as earlier reported in London by Chahal et al. 35 The hemodynamic changes seen in eccentric hypertrophy are associated with increased in LV end diastolic and systolic volume due to LV volume overload, hence heralding the development of heart failure in hypertensive patients. Studies have shown that severe systolic dysfunction is observed more frequently in hypertensive patients with eccentric hypertrophy than concentric hypertrophy. 36,37
The Doppler echocardiographic parameters showed some degree of diastolic dysfunction in our hypertensive patients with abnormal LV geometric patterns. Other studies have also demonstrated that hypertensive patients may have diastolic dysfunction, regardless of the differences in their structural geometries.12,25,38–40 In addition, the degree of impairment of cardiac diastolic function differed between hypertensive patients with different LV geometric patterns,12,39,40 which was worst in those with concentric geometry. 12 Diastolic dysfunction was observed in incipient stages of hypertensive heart disease, and thus its early detection may help in the risk stratification of hypertensive patients. 38 Karaye et al recently assessed right ventricular (RV) systolic and diastolic dysfunction (RVSD and RVDD, respectively) in Nigerian hypertensives, stratified by LV geometric patterns. The study revealed that approximately two-thirds of the hypertensives had RVDD, while about one-third had RVSD. Subjects with eccentric hypertrophy had the highest prevalence of RVSD, while RVDD was common across all groups. 41 Since studies have shown that prompt diagnosis and treatment of hypertension could reverse or retard the LV hypertrophy in hypertensive patients,42,43 these should be among the main goals in such patients.
Conclusions
Concentric remodeling was the most common LV geometric pattern in our hypertensive patients. This was followed by concentric hypertrophy and eccentric hypertrophy. Patients with concentric hypertrophy were older than those with other geometric patterns. LV systolic function was significantly lower in patients with eccentric hypertrophy and some degree of diastolic dysfunction were present in hypertensive patients with abnormal LV geometry.
Author Contributions
Conceived and designed the experiments: RAA, MOB, AOA. Analyzed the data: RAA, OJB, VOA, LAB, TOM, EAA, OOA. Wrote the first draft of the manuscript: RAA, OJB. Contributed to the writing of the manuscript: RAA, OJB, MOB, AOA, VOA, LAB, TOM, EAA, OOA. Agree with manuscript results and conclusions: RAA, OJB, MOB, AOA, VOA, LAB, TOM, EAA, OOA. Jointly developed the structure and arguments for the paper: RAA, OJB, MOB, AOA, VOA, LAB, TOM, EAA, OOA. Made critical revisions and approved final version: RAA, OJB, MOB, AOA, VOA, LAB, TOM, EAA, OOA. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.