
Abstract
With the introduction of the revised World Health Organization Classification of Tumors of Hematopoietic and Lymphoid Tissues in 2001, many patients had to be re-evaluated for the correct diagnosis of T- and NK-cell lymphomas. Because some T-cell malignancies are associated with poor outcome, it is important to identify subsets of patients that may benefit from novel or more intensive therapies. The purpose of this study was to determine, for the first time, the relative frequencies, pathological features and outcomes of patients with T- and NK-cell lymphomas in a predominantly Russian Slavic population. We identified 291 patients with a diagnosis of T- and NK-cell malignancies treated at our Center between 2000-2008. In applying the revised WHO classification, we confirmed the diagnosis and had complete clinical follow up and pathological information on 264 cases that were included in the analysis. We found some differences in frequency of several subsets as compared with previously published reports, including younger age of onset and relatively higher incidence of T-LGL in our patients. We also confirm that intensive treatment regimens of advanced stage PTCL and ALK—ALCL led to considerable improvement in response rates, but not in the overall survival.
Introduction
The understanding and classification non-Hodgkin's lymphomas (NHL) have evolved over the last thirty years. Currently, the most widely accepted system is the recently revised World Health Organization (WHO) Classification of Tumors of the Haematopoietic and Lymphoid Tissues. 1 Previous classification systems relied primarily on morphology and werre less reproducible and poorly predictive of patient outcome.2–6 The WHO system relies on a multi-parameter approach to classification using morphologic, immunophenotypic, molecular, and clinical aspects to define disease entities. The WHO classification groups T- and NK-cell leukemias and lymphomas, and divides T-cell neoplasms into those that express an immature or precursor (pre-thymic) phenotype, and those expressing a mature or peripheral (post-thymic) phenotype. The normal counterpart of the neoplastic cells, initially proposed by the Kiel classification in the 1970's 2 is now further defined with regulatory T-cells (Treg) for adult T-cell leukemia/lymphoma (ATLL), and follicular T-helper cells (TFH) for angioimmunoblastic T-cell lymphoma (AILT). Until recently, T-cell lymphomas were often treated and analyzed along with high grade B-cell lymphomas with little appreciation of their different natural history and responsiveness to therapy. Thus, many disease-specific outcomes reported in previous studies may be open to question.6–10
T-cell and NK-cell leukemias and lymphomas are relatively uncommon constituting <10% of non-Hodgkin lymphomas occurring in Europe and North America. 11 The majority of these neoplasms exhibit a mature or post-thymic phenotype. These tumors characteristically express CD3, albeit at variable levels, and a monoclonal T-cell receptor (TCR) α and β, and less frequently a γ and δ TCR rearrangement. These minimal requirements permit classification of these tumors as belonging to a T-cell lineage. Additional markers expressed on these tumors often include CD4, and less frequently, CD8. Malignant NK-cell disorders occur less frequently and also express cell surface markers that facilitate identification. NK-cell markers include CD16, CD56, and CD57. 12 CD3 is not usually seen on the cell surface, and is often cytoplasmic. Additional molecular markers and immunohistochemical tools for diagnosis of T- and NK-cell lymphoma are being researched.13–15
There are marked geographical and ethnic variations in the incidence of T-cell malignancies. In the United States and Western Europe, peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS), anaplastic large cell lymphoma (ALCL) and angioimmunoblastic T-cell lymphoma (AILT) are the most frequent.3,16,17 In Asia, Central and South America, a larger fraction of lymphoid malignancies are represented by NK/T-cell tumors that are rare in North America and Europe.18–21 The incidence of adult T-cell leukemia/lymphoma (ATL), characterized by CD4-positive lymphocytes with a monoclonal integration of human T-cell lymphotrophic virus-1 (HTLV-1) provirus in the tumor cells, 22 mimics the geographical seroprevalence of the causative agent, with increased frequencies in Africa, Caribbean basin and southern Japan.
T-cell lymphomas in general carry a poorer prognosis than do B-cell lymphomas, and the clinical outcome is related to the specific subtype.6,23 Treatment of patients with ALK+ ALCL versus PTCL-NOS with CHOP-based chemotherapy is likely to result in different long-term disease-free survivals. As a result, assigning patients to the correct diagnostic category is critical for selection of therapy and interpretation of clinical trials.
Little is known about the frequency of the various subtypes and clinical outcomes of T-cell lymphomas seen in the Russian Federation. Herein we describe the relative frequencies, clinicopathological features and treatment outcomes for 264 patients with T- and NK-cell lymphomas re-classified under the WHO Classification in a predominantly Russian Slavic population treated at our institution.
Materials and Methods
Patients
Clinical, laboratory and pathology records of all patients seen between 2000-2008 at the Federal Research Hematology Center, Russian Academy of Medical Sciences were reviewed and those assigned the diagnosis of T- and NK-cell leukemia or lymphomas were selected. All patients were of Eastern European Caucasian (mostly Slavic) background. The diagnoses were reviewed and regrouped, when appropriate, according to the revised WHO classification system. In 51 uncertain cases, further pathological and immunohistochemical analysis were preformed on archived material. Several cases were also reviewed by Dr. E. Jaffe in the Laboratory of Pathology at the National Cancer Institute in Bethesda, MD, USA. Cases in which the diagnosis could not be confirmed were excluded. Few cases where a definitive diagnosis could not be reached because of inadequate histopathology, immunohistochemical stains, or lack of appropriate materials for additional testing, were also excluded from the final analysis. Ultimately, from the total of 291 cases screened, 264 cases fulfilled the diagnostic criteria and were the subject of the analysis. During the study period, a number of chemotherapeutic agents and combination chemotherapies were used (Supplemental Table 1). In general, high-dose pulsed combination chemotherapy was used for aggressive T-cell lymphomas and long-term intensive combination chemotherapy regimens were used for treatment of T-cell lymphoblastic lymphoma. Patients achieving a complete remission routinely received involved-field radiotherapy as consolidation. Single agent chemotherapy was used for the treatment of indolent T-cell lymphomas when clinically indicated.
Clinicopathologic features of 264 cases of T- and NK-cell neoplasms.

Clinical treatment responses were defined as follows: A complete response (CR) required the patient to have no evidence of disease that persisted for at least 6 weeks, a partial response (PR) was defined as ≥50% reduction in the sum of measurable tumor, or minimal residual disease present at re-staging, and progressive disease (PD) defined as a greater than ≥25% increase in measurable tumor, or the appearance of at least one new lesion. Patients not meeting the criteria for any of these three response categories were determined to have stable disease (SD). Initial tumor staging and re-staging was performed using CT-imaging, bilateral bone marrow aspirate and biopsies with pathology review, cytology and studies for the presence of clonal TCR rearrangements using polymerase chain reaction (PCR).
Laboratory Data
Hematoxylin-eosin stained tissue sections, immunohistochemical analysis of paraffin-embedded and/or frozen sections, fluorescence microscopy and/or flow cytometry to detect expression of CD2 (AB75, Novocastra, Newcastle-upon-Tyne, UK), CD1a (MTB1, Novocastra), CD3 (Policlon Dako, Glostrup, Denmark), CD4 (1F6, Novocastra), CD5 (SP19, Dako), CD7 (CD7-272, Novocastra), CD8 (1 A5, Novocastra), CD10 (56C6, Novocastra), CD16 (2H7, Novocastra), CD19 (LE-CD19, Dako), CD20 (L26, Dako), CD22 (RFB4, Novocastra), CD23 (1B12, Novocastra), CD25 (4C9, Novocastra), CD30 (Ber-H2, Dako), CD34 (QBEnd/10, Novocastra), CD45 (2B11+ PD7/26, Dako), CD56 (123C3, Dako), terminal deoxythymidylate transferase (TdT) (SEN28, Novocastra), epithelial membrane antigen (EMA) (E29, Dako) and anaplastic lymphoma kinase (ALK) (ALK1, Dako) were performed. Flow cytometry was performed in those patients that exhibited bone marrow and peripheral blood involvement by tumor. TCR gene rearrangement was detected using the polymerase chain reaction (PCR) on DNA extracted from paraffin embedded fresh tumor or on peripheral blood since 2003.24–27
Statistical Analysis
Kaplan-Meier analysis was utilized for generating survival curves. Survival was calculated from the time of diagnosis until death or the date of the last follow-up (censor time). Death was used as an endpoint regardless of cause. For long-term survivors, life span was calculated as the time between the diagnosis and the date of the last follow-up (censor time). The Mantel-Hanzel and log-rank tests were used for comparison of survival rates between various groups of patients. Survival differences were considered significant when P-values for all three tests were <0.05.
Results
We identified 291 patients with T- or NK-cell lymphomas that were evaluated in the Department of Chemotherapy, Hematological Diseases and Intensive Therapy at the Federal Research Hematology Center of Russian Academy of Medical Sciences between 2000-2008. Subsequent analysis led to exclusion of several patients due to changes in diagnosis or lack of an adequate follow-up. Three patients were re-classified as B cell lymphomas, 5 with lymphogranulomatosis and one with berylliosis. The use of TCR gene rearrangement has helped to exclude reactive lymphoid disorders and improve the diagnostic accuracy. A total of 27 cases, including 12 patients whose diagnosis was confirmed, but were subsequently treated at other institutions, were also excluded from the analysis. The final analysis was conducted on a group of 264 patients. Thus, from a total of 2477 patients with a diagnosis lymphoma treated at our institution, 10.6% had T- or NK-cell lymphomas, 1,168 (68.2%) had B-cell lymphomas, and 532 (21.5%) had Hodgkin's Disease. The clinical presentation and final pathologic diagnosis are presented in Table 1 and Figure 1.

Venn diagram, frequency of T- and NK-cell lymphoma subtypes seen at the Federal research Hematology Center of the russian Academy of Medical Sciences 2000-2008.
The group of 264 patients with T- or NK-cell lymphomas included 128 men and 136 women, a male to female ratio of approximately 1:1, which differs from previous reports that demonstrated a male predominance of T-cell lymphomas.10,28 This difference may be attributed to the overall decline in male life expectancy in Russia to 65, the lowest in Europe by 2008 according to the European “Health for All” Database (HFA-DB). A younger age at diagnosis was also apparent in our series with an overall median age of 49 years (16-87 years). Specific lymphoma subtypes and their frequencies are shown in Table 1. The most frequent subtypes were T-cell large granular lymphocyte leukemia (22.7%) and mycosis fungoides (17.8%). Cutaneous T-cell lymphomas (CTCL) accounted for 29.2% of cases with Sézary syndrome (SS) seen in 7.6% of patients. A relatively small number of PTCL-NOS (8.3%), ALK-negative ALCL (8.7%) and ALK-positive ALCL (5.3%) were seen. Precursor T-cell lymphoblastic lymphoma (T-LBL) accounted for 11.4% of cases. Extranodal lymphomas that included hepatosplenic T-cell lymphoma and other rare extranodal NK/T-cell lymphomas accounted for a combined total of 9.1% of diagnoses. Other rare forms included CD30+ primary cutaneous anaplastic large cell lymphoma (3.8%), adult T-cell leukemia/lymphoma (2.3%) and T-cell prolymphocytic leukemia (1.1%). Interestingly, no cases of blastic NK-cell lymphomas, aggressive NK-cell leukemia or subcutaneous panniculitis-like T-cell lymphoma were observed.
Thirty nine patients (19.1%) presented with stage I/II disease. The remaining 165 patients (80.9%) had stage III or IV disease at presentation, and were often admitted in serious condition for hospital care. Median overall follow up for the entire group was 40 months (range, 1-282 months).
One hundred eighty four patients (69.7%) were treated during their illness with different chemotherapeutic regimens or single agents (Supplemental Table 1). Seventy-three of these patients achieved a CR with a median duration of 38 months (7-101 months). Eleven of these patients subsequently relapsed. Thirty-six patients achieved a PR. The remaining 75 (40.7%) had SD. Most of these patients had CTCL or T-LGL. These patients received either single agent chemotherapy or were followed without treatment. Overall, from 264 patients, 80 patients are known to have (30.3%) died of disease. Kaplan-Meier survival estimates for all patients with T- and NK-cell lymphomas are presented in Figure 2A and B.

Kaplan-Meier survival for patients with T- and NK-cell lymphomas. (A) Kaplan-Meier survival estimates for patients with T-cell leukemia and extranodal lymphomas (N = 170). (B) Kaplan-Meier survival estimates for patients with nodal and lymphoblastic T-cell lymphomas (N = 94).
Specific Diseases
Cutaneous T-Cell Lymphoma (Ctcl)
Seventy-seven patients from a total of 264 had CTCL. Of these, 47 (17.8%)-presented with classical mycosis fungoides, 20 (7.6%) with Sézary syndrome and 10-(3.8%) with CD30+ primary cutaneous ALCL and other rare forms. Skin biopsies showed typical epidermotrophic infiltration of the skin by abnormal T-cells. On immunohistochemical staining most of the lymphocytes in mycosis fungoides and Sézary syndrome were CD2+, CD3+, CD43+ and CD4+, and CD8-, CD7-, CD30- and ALK-. However, in 20% of cases the immunophenotype also showed loss of CD4 expression as previously reported by. 29 Among these CTCL patients, the diagnosis was made with difficulty in three cases. These patients were initially classified as ALCL, but were subsequently re-classified as having transformed MF. Characteristics and survival and are shown on Figure 1 and summarized in Table 1.
Mycosis Fungoides (Mf)
Among 77—patients with cutaneous T-cell lymphoma, 47 had MF. Of these, 25 were male and 22 female with a median age of 53 years (21-86 years). Twenty-four were stages I/II and 23 patients were stages III/IV. All patients received treatments appropriate for their disease stage. For stage I/II patients, the following therapies were utilized: psoralen with ultraviolet-A (PUVA) phototherapy, alpha-interferon, denileukin difititox, bexarotene, or single agent methotrexate or cyclophosphamide. Patients that relapsed or presented with stage III/IV disease received combination chemotherapy with CHOP-like regimens, fludarabine or cladribine. Eleven patients died. The median observation time for all MF patients was 85 months (5-282 months).
Sézary Syndrome (SS)
Twenty patients presented with SS. This group included 12 males and eight females with median age of 54 years (21-89 years). All had stage III/IV disease and received a variety of treatments that included alpha-interferon, bexarotene, single agent chlorambucil or fludarabine, alemtuzumab, biweekly alemtuzumab-CHOP (A-CHOP-14), or MACOP-B. The median survival of Sézary patients was 75.3 months (12-126 months) (Fig. 1 and Table 1).
CD30+ Primary Cutaneous Anaplastic Large Cell Lymphomas (Alcl) and other Rare Cutaneous T-Cell Lymphomas
We had ten patients (3.8%) with other primary cutaneous T-cell lymphomas. This group included 5 males and 5 females with a median age of 40 years (20-70 years). Four patients had CD30+ primary cutaneous anaplastic large cell lymphoma and six patients were diagnosed with primary cutaneous CD8+ epidermotropic cytotoxic T-cell lymphoma. 30 Five patients were stage IV at diagnosis. These patients were treated with alpha-interferon, radiotherapy, or combination chemotherapy including MACOP-B or A-CHOP-14. Four stage IV patients died within the time of observation and the remaining 6 had a PR and continue to be observed. The median follow up for patients in this group is 61 months, with a median survival of 58.6 months (5-105 months).
Peripheral T-Cell Lymphoma, Not Otherwise Specified (Ptcl-Nos)
PTCL-NOS was diagnosed in 22 patients that included 12 men and 10 women with a median age 43 years (20-67 years). Two patients had stage II disease at diagnosis, and the remaining 20 patients had stage III/IV disease. In addition to generalized infiltration of lymph nodes, these patients often had hepa-tosplenomegaly (11 patients), anterior mediastinum and mediastinal lymph nodes (10 patients), bone marrow (7 patients), and the lungs, pleura, pericardium, soft tissue (2 patients each), as shown in Table 1.
Microscopic analysis showed diffuse infiltration of lymph nodes and various organs with abnormal T-cells with a highly variable number of medium and large cells with non-uniform nuclei. Immunophenotyping showed CD3+ staining of the cell membrane, and variable staining for CD2, CD5, CD4, CD45RO, and the lack of CD30 expression or immature T-cell markers, such as TdT and CD1a. Four patients expressed the CD8 co-receptor, and the remaining tumors were CD4-positive. A clonal T-cell receptor rearrangement was detected in 17 of 22 patients (77.2%).
Seventeen patients were treated with CHOP-like regimens including CHOP, A-CHOP-14 ProMACE-CytaBOM, and ESHAP. Four patients received the intensive eight drug BFMT-93 (GMALL 05/93) protocol. 31 A CR was achieved in 13 of 22 patients. Six patients died of progressive disease. Nine of 17 patients treated with a CHOP-like regimen achieved a CR; however, all four patients receiving the BFMT-93 protocol in which thymic irradiation was administered during second induction cycle achieved a CR. The median follow up in this group was 26 months with median survival of 54.9 months (2-76 months).
Anaplastic Large Cell Lymphoma Alk-Negative (Alcl Alk-)
Twenty-three patients were confirmed with ALCL ALK-, including 12 males and 11 females with a median age of 43 years (21-70 years). Three patients had stage IIB disease, and 20 patients were stages III/IV. Most presented with symptomatic disease. In addition to generalized infiltration of lymph nodes, hepatosplenomegaly (10 patients), anterior mediastinum (12 patients), other extranodal locations were observed (Table 1). Pathological examination of lymph nodes revealed anaplastic cells with large eccentric nuclei and abundant cytoplasm. Immunophenotyping confirmed expression of CD30 with variable expression of CD45, CD3 and CD43. The majority of these cases were CD4+.
Twelve of these patients were initially treated for Hodgkin's disease or other types of lymphoma at other institutions with ABVD, BEACOPP, Dexa-BEAM, ProMACE-CytaBOM, or CHOP. Subsequent review led to a change in the diagnosis to CD30+ ALCL ALK-. A CR was achieved with the initial treatment in six patients. Two patients subsequently relapsed. Eleven of the 23 ALCL ALK—patients received treatment with a modified NHL-BFM-90 protocol,32,33 and nine patients achieved a CR. Three of these patients relapsed and subsequently died of disease. A total of 10 patients died within 1-20 months. The follow up time in this group ranged from 1 to 58 months. Median survival for these patients was 24 months.
Anaplastic Large Cell Lymphoma, Alk-Positive (Alcl Alk+)
Fourteen patients were diagnosed with ALCL ALK+ including 7 males and 7 females with a median age of 30 years (16-65 years). One patient had stage IIB disease; the remaining 13 patients were stages III or IV, and usually presented with symptomatic disease. In addition to generalized infiltration of lymph nodes, hepatosplenomegaly (6 patients), involvement of anterior mediastinum (3 patients), muscle, soft tissue, subcutaneous tissue, skin, pleura (3 patients each) and other extranodal locations were observed (Table 1).
On microscopic examination these tumors showed high proliferative activity identified by Ki-67 staining of nearly 100%. Clonal rearrangement of T-cell receptor was detected in 46%. All were ALK+. They received treatment with a modified NHL-BFM-9032,33 protocol previously used for aggressive B-cell lymphomas and adapted for use in pediatric ALCL. Complete responses were achieved in 13 of 14 patients and these were maintained for a median of 24.0 months (8-77 months). One patient died during the first course of therapy, and another patient subsequently relapsed with lymphomatous meningitis and died. At a median follow-up of 34.5 months, the median survival has not been reached.
Angioimmunoblastic T-Cell Lymphoma (Aitl)
AITL was diagnosed in five female patients (1.9%) median age of 60 years (50-76 years) that presented with enlarged lymph nodes, hepatosplenomegaly (5 patients), bone marrow infiltration (4), anterior mediastinal adenopathy (3), and B symptoms, elevated ESR, and polyclonal hypergammaglobulinemia were seen in all. On lymph node biopsy, large “blastlike” tumor cells with pale cytoplasm were present. A reactive background was also observed consisting of follicular dendritic cells, macrophages, epithelioid histiocytes, and reactive plasma cells. In one patient on weekly methotrexate and prednisone, the disease remained stable for a period of two and half years. The second patient achieved a CR following treatment with the NHL-BFM-90 regimen and involved field radiation therapy. Three patients were treated on the BFMT-93 protocol; however, two patients required interruption of chemotherapy due to prolonged granulocytopenia. They continued treatment with thalidomide, methotrexate and 6-mercaptopurine. These patients achieved a CR.
Extranodal T-Cell Lymphomas
This pathology accounted for 24 patients (9.1%) who presented with variable sites of tumor infiltration and are considered as a single group. Median age at presentation was 54 years (26-73 years). Thirteen patients were male and 11 were female. Two of the patients had stage II disease, and the remaining presented with stage III/IV disease.
Sinonasal and Extranasal Nk/T Cell Lymphomas
Of 10 patients, infiltration of the mucosa of nasopharynx was documented in three patients. Involvement of soft tissues was observed in two patients, and the mediastinum, lungs, and pleura and other organs were involved in five patients.
Hepatosplenic T-Cell Lymphoma (Hstl)
Fourteen patients were diagnosed with HSTL. The patients lacked lymphadenopathy, but had hepatosplenomegaly (all 14 patients), bone marrow (6 patients), and all had B-symptoms. Two patients with HSTL presented in critical condition and died before therapy could be initiated.
Patients with extranodal lymphomas were treated with CHOP-like regimens including, MACOP-B and A-CHOP-14, FMC or the intensive NHL-BFM-90 regimen. In cases with bone marrow infiltration and cytopenia, immunosuppressive therapy was initiated and splenectomy was performed. A CR was achieved in 10 patients, two patients relapsed, and 12 patients died. Median duration of follow up was 55 months and median survival was 66.9 months (1-136 months).
T and Nk-Cell Leukemias
T-cell large granular lymphocyte leukemia (T-LGL) and chronic lymphoproliferative disorder of NK cells (CLPD-NK) were diagnosed in 60 patients (22.7%) that included 21 males and 39 females with a median age 52.5 years (17-74 years). CLPD-NK was diagnosed in five patients and T-LGL was diagnosed in 55 patients. Enlargement of the liver was present in 29 patients. Clinical features also included infiltration of the bone marrow in 44, hemocytopenias in 36, polyarthritis in 8, and chronic low-grade fever in 7 patients.
T-Cell Large Granular Lymphocyte Leukemia
Three T-LGL variants were observed: (1) Twenty-nine patients with an immunophenotype characterized as CD3+, CD8+, CD56- and CD16-; (2) Nineteen patients had a T-cell immunophenotype that was variably CD3+, CD8+, CD57+ and CD16+; and (3) five patients whose T-cells were CD3+, CD4+ and CD8+ (double-positive), and CD57+. No significant clinical distinctions were observed among patients with these variants, but the third variant was more often associated with hepatosplenomegaly and lymphocytosis.
Thirty-six T-LGL patients were treated with various agents including single agent cyclophosphamide, methotrexate, cyclosporine A, alpha-interferon, alemtuzumab or corticosteroids. Twelve patients with persistent cytopenias underwent splenectomy with temporary improvement of blood counts. Nineteen patients had stable disease. None of the patients achieved a CR, but disease stabilization was observed in some patients for up to 3 years after splenectomy. Four patients died from infectious complications and three died from various adenocarcinomas (stomach, ovary, and lung). Another four patients died with an aplastic bone marrow syndrome. The median follow up time was 37.5 months (8-195 months). After 5 years, the median survival has not been reached in this group of these patients.
Chronic Lymphoprolyferative Disorder of Nk Cells (Clpd-Nk)
Five patients were diagnosed with CLPD-NK. The NK-cell immunophenotype consisted of variable levels of expression of CD2, CD56 and CD16 and the absence of CD3 and CD8. This group included one man and four women with a median age of 48 years (23-60 years). Splenomegaly was present in two patients and two patients had polyarthritis. Ganulocytopenia was present in three patients and it was associated with an increase frequency of infections and inflammatory complications. Median duration of follow up was 75 months (30-213 months) in this group. One patient received treatment with low dose methotrexate with limited response.
Data on three patients with T-cell prolymphocytic leukemia (T-PLL) and on six patients with HTLV-1-asociated adult T-cell leukemia/lymphoma are shown in the Table 1. One patient achieved a CR with chemotherapy, but subsequently relapsed and died of infectious complications.
T-Cell Lymphoblastic Lymphoma (T-Lbl)
There were 30 cases of T-LBL that included 17 males and 13 females with a median age 33 years (17-71 years). These tumors demonstrated cytoplasmic, but not cell surface staining for CD3, expression of CD1a and CD10, lack of CD4 and CD8, and expression of terminal deoxynucleotidyl transferase (TdT). In addition to lymph node involvement, involvement of the anterior mediastinum (14 cases), pleura (5 cases), pericardium (6 cases), bone marrow (8 cases), hepatosplenomegaly (15 cases), and other sites were observed (Table 1). Almost a half of these patients were initially assigned a diagnosis of PTCL and treated with CHOP-like chemotherapy. Four patients achieved a CR and 5 patients progressed and died. Twenty-one patients were treated with the BFMT-93 regimen. Sixteen achieved a CR and three subsequently relapsed. Five patients failed to respond to treatment and rapidly progressed and died. Three patients refused treatment and five patients continue on treatment at this time. The median survival for this group is 59.3 months (1-172 months).
Discussion
T- and NK-cell leukemias and lymphomas are a heterogeneous group of lymphoid neoplasms that account for less than 10% of total lymphomas reported in North America and Western Europe. In contrast, these disorders represent nearly one-third of lymphomas reported in Southern Asia highlighting their marked geographical variability.12,13 Recent updates using the revised WHO classification confirm higher overall incidence in South West China, Thailand and Central Asia,10,28,34,35 as compared to those reported from European populations, such as Italy. 36 Previously, little was known about the relative frequencies and outcomes of the various subtypes of T- and NK-cell lymphoma in European Russia. In our series of 264 unselected patients available for follow up studies, we found some significant differences from those reported in other series. Specifically, we observed an equal proportion of affected men and women, in contrast to the male predominance in reports from Western European, North America and Asia.10,28 We also observed younger median age of onset, and both results may reflect demographic differences in the Russian population. Secondly, we had a higher proportion of patients with PTCL, likely because our Center is known for treating patients with later stages of this disease. Third, we report only five cases of angioimmunoblastic T-cell lymphoma. In contrast, other series report frequencies of AITL of up to 25%1,15 and over 20% of Russian patients had T-LGL, as compared to a 2%-5% reported in North American and European series.15,16 The reasons for these differences are unclear although the incidence of T- and NK-cell leukemias and lymphomas are known to have significant geographical variations based etiology and possibly genetic predisposition. Interestingly, Gluzman and coworkers reported an unusually high number of cases of T-LGL in workers involved in clean-up operation after the 1986 accident in the Chernobyl nuclear reactor. 37 What role this increase played in the cases seen at our Center is uncertain.
Of the initial 291 cases identified, 10 patients (3.5%) underwent a significant change in diagnosis after the review, which it is similar to the frequency of changes reported by others.15,16,20 We encountered difficulties in verification of some specific subsets, such as in differentiation of T-cell lymphoblastic lymphomas from PTCL. Additional tools for more precise separation of precursor (immature) T-cell lymphomas from mature T-cell lymphomas are needed and will require further studies.
Our series confirms the favorable prognosis of indolent disorders such as CTCL and T-LGL. In both of these diseases, stage-specific treatments led to improvements in patient's quality of life, but did not prolong survival. The median survival has not been reached in these groups as of submission of this manuscript. The poor outcome of PTCL with borderline features that may represent transitional forms often characterized by infiltration of mediastinum, is also a common pattern of relapse and resistance to CHOP-like regimens. These features lead us to consider alternative, more aggressive treatments for these patients. Published results suggested that an improved outcome could be achieved in PTCL using a regimen that has been previously used to treat acute T-cell leukemias, BFMT-93 (GMALL). 31 In 2003, we began using this regimen for high grade PTCL and PTCL with mediastinal involvement. All four patients treated with this regimen achieved durable complete responses. Most ALK- ALCL also have an aggressive course with fatal outcomes when treated with standard CHOP-like combination therapies. 38 Our results in a small number of ALK—ALCL patients using the BFM-9032,33 also demonstrated high rate of complete responses. Thus, we propose that these regimens need to be studied in a larger cohort of these patients.
In conclusion, our experience at the Russian National Center for Hematology using the revised WHO classification of T- and NK-lymphomas demonstrated a number of significant differences in the relative proportions of the various subtypes of T- and NK-cell leukemias and lymphomas from published series from Western Europe and North America. We also saw differences in the sex ratio and age distribution of occurrence. Based on our limited experience, we propose that patients with PTCL-NOS, ALK—ALCL and AITL may benefit from more aggressive regimens, such as BFMT-93 or BFM-90, previously used in patients with acute T-cell lymphoblastic leukemia.31,32,33,39 New therapeutic agents, monoclonal antibodies and targeted therapies with antitumor activity in specific T-cell lymphomas have recently become available, which highlights the importance of assigning an accurate diagnosis to these diseases.40–42
Abbreviations
ALCL, anaplastic large cell lymphoma; AILT, angioimmunoblastic T-cell lymphoma; ALK, anaplastic lymphoma kinase; ATLL, adult T-cell leukemia/lymphoma; C-ALCL, cutaneous anaplastic large cell lymphoma; CLPD-NK, chronic lymphoproliferative disorder of NK cells; CT, computerized tomography; CTCL, cutaneous T-cell lymphoma; ESR, erythrocyte sedimentation rate; HSTL, hepatosplenic T-cell lymphoma; HTLV-1, human T-cell lymphotropic virus-1; MF, mycosis fungoides; NHL, non-Hodgkin's lymphoma; PCR, polymerase chain reaction; PTCL, NOS, peripheral T-cell lymphoma, not otherwise specified; SS, Sézary syndrome; TdT, terminal deoxynucleotidyl transferase; T-LBL, T-cell lymphoblastic lymphoma; T-LGL, T-cell large granular lymphocyte lymphoma.
Author Contributions
Conceived and designed the experiments: YEV, IBK, NES-K, RSS, IAV, LGA, AIV. Analysed the data: YEV, BVZ, JCM, DSM, LV, NES-K. Wrote the first draft of the manuscript: YEV, JCM, LV, NES-K. Contributed to the writing of the manuscript: YEV, JCM, LV, NES-K. Agree with manuscript results and conclusions: YEV, IBK, NES-K, RSS, IAV, YVS, LGA, DCM, JCM, AIV. Jointly developed the structure and arguments for the paper: YEV, JCM, LV, NES-K. Made critical revisions and approved final version: YEV, LV, NES-K. All authors reviewed and approved of the final manuscript.
Funding
This work was supported, in part, by the federal support to the Hematology Center of Russian Academy of Medical Sciences, Moscow, Russia, and the NIH intramural program at the Center for Cancer Research, National Cancer Institute, Bethesda, MD, USA.
Disclosures and Ethics
There are no conflicts of interest and no disclosures to be reported.
Footnotes
Supplementary Table
Combination chemotherapeutic regimens used to treat T-cell lymphomas. To compare with previously published regimens see References.31–33,39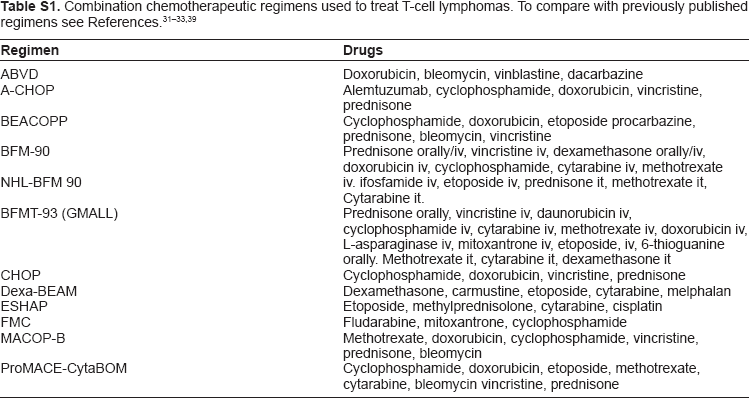
Regimen
Drugs
ABVD
Doxorubicin, bleomycin, vinblastine, dacarbazine
A-CHOP
Alemtuzumab, cyclophosphamide, doxorubicin, vincristine, prednisone
BEACOPP
Cyclophosphamide, doxorubicin, etoposide procarbazine, prednisone, bleomycin, vincristine
BFM-90
Prednisone orally/iv, vincristine iv, dexamethasone orally/iv, doxorubicin iv, cyclophosphamide, cytarabine iv, methotrexate
NHL-BFM 90
iv. ifosfamide iv, etoposide iv, prednisone it, methotrexate it, Cytarabine it.
BFMT-93 (GMALL)
Prednisone orally, vincristine iv, daunorubicin iv, cyclophosphamide iv, cytarabine iv, methotrexate iv, doxorubicin iv, L-asparaginase iv, mitoxantrone iv, etoposide, iv, 6-thioguanine orally. Methotrexate it, cytarabine it, dexamethasone it
CHOP
Cyclophosphamide, doxorubicin, vincristine, prednisone
Dexa-BEAM
Dexamethasone, carmustine, etoposide, cytarabine, melphalan
ESHAP
Etoposide, methylprednisolone, cytarabine, cisplatin
FMC
Fludarabine, mitoxantrone, cyclophosphamide
MACOP-B
Methotrexate, doxorubicin, cyclophosphamide, vincristine, prednisone, bleomycin
ProMACE-CytaBOM
Cyclophosphamide, doxorubicin, etoposide, methotrexate, cytarabine, bleomycin vincristine, prednisone
Acknowledgments
The authors wish to thank Dr. Elaine S. Jaffe for help in reviewing difficult cases in order to verify the accuracy of classification.