
Abstract
Chronic myeloid leukemia (CML) is a myeloproliferative neoplasm characterized by the presence of the Philadelphia (Ph) chromosome resulting from the reciprocal translocation t(9;22)(q34;q11). The molecular consequence of this translocation is the generation of the BCR-ABL fusion gene, which encodes a constitutively active protein tyrosine kinase. The oncogenic protein tyrosine kinase, which is located in the cytoplasm, is responsible for the leukemia phenotype through the constitutive activation of multiple signaling pathways involved in the cell cycle and in adhesion and apoptosis. Avascular necrosis of the femoral head (AVNFH) is not a specific disease. It occurs as a complication or secondary to various causes. These conditions probably lead to impaired blood supply to the femoral head. The diagnosis of AVNFH is based on clinical findings and is supported by specific radiological manifestations. We reported a case of a 34-year-old Sudanese female with CML who developed AVNFH after receiving dasatinib as a second-line therapy. Though the mechanism by which dasatinib can cause avascular necrosis (AVN) is not clear, it can be postulated because of microcirculatory obstruction of the femoral head. To the best of our knowledge and after extensive literature search, this is the first reported case of AVNFH induced by dasatinib in a patient with CML.
Background
Chronic myelogenous leukemia (CML) is a chronic myeloproliferative disorder with an initially chronic course lasting for 3-5 years. It eventually transforms into accelerated or blastic phases, which are generally fatal. CML was one of the first diseases in which a specific chromosomal abnormality was identified, a t(9;22)(q34;q11) or Philadelphia (Ph) chromosome.
Avascular necrosis of the femoral head (AVNFH) occurs as a complicated traumatic or nontraumatic disorder. Most cases of AVNFH are nontraumatic and occur secondary to excessive corticosteroid use and alcohol abuse. 1 Other causes include coagulopathies, hemoglobinopathies (eg, sickle cell disease), chronic liver disease, gout, idiopathic hyperlipidemia, metabolic bone disorders, pregnancy, radiation, chemotherapy, smoking, systemic lupus erythematosus, and vasculitis syndromes. Intravascular coagulation appears to be the central event associated with nontraumatic AVNFH. 2 Coagulation may occur secondary to extravascular compression (eg, marrow fat enlargement), vessel wall injury (eg, chemotherapy, radiation), or a thromboembolic event (eg, fat emboli). In addition, ischemic insult to the femoral head may result in subchondral bone infarction. In this situation, weakened and unrepaired necrotic bony trabeculae fail under a compressive load, leading to subchondral collapse (eg, crescent sign), and ultimately, articular collapse. 3 Traumatic causes of femoral head avascular necrosis (AVN) include femoral neck fractures, hip dislocation, and slipped capital femoral epiphysis. 4
AVNFH can be presenting manifestation for a patient with CML. We did literature review and came with number of cases reporting AVNFH as an initial presentation of CML, illustrated in Table 1.
CML presenting with AVNFH.
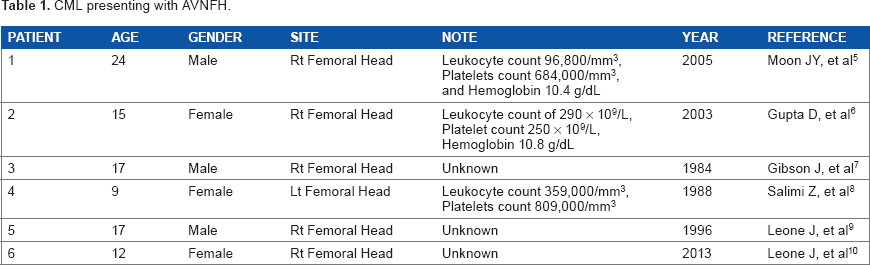
AVNFH has been reported as an initial presentation in few cases with CML by many authors (Table 1).
Case Presentation
A 34-year-old Sudanese female with the diagnosis of CML was started on imatinib as a first-line therapy, but she failed the first-line therapy as per European Leukemia Net guidelines 2010. She was referred to the hematology service at the National Center for Cancer Care & Research (NCCCR) for further evaluation. Her clinical examination was unremarkable, and her work-up was repeated, including a complete blood count, cytogenetics, and BCR/ABL by PCR plain radiograph before treatment was available and she was reported as normal. Her work-up revealed a chronic phase of CML in failing first-line therapy. She was started on dasatinib 100 mg PO once daily as a second-line therapy with which she achieved CHR, CCYR, and MMR at 18 months. After 18 months on therapy with dasatinib, she presented with severe pain in her left groin with limping. Her complete blood count (CBC) was within normal limit—WBC 6000, Hb 13 g/dL, and Plts 235,000. Her peripheral smear reported as normal, and her disease revaluated at the molecular level and showed major molecular response. Radiological evaluation, including pelvic radiography (see Fig. 1A and B) and magnetic resonance imaging (MRI) showed grade 3-4 AVNFH (see Fig. 2A-E).

(A) Plain radiography (anteroposterior (AP) view of both hip joints) and (B) pelvic radiography (close oblique view of the left hip).
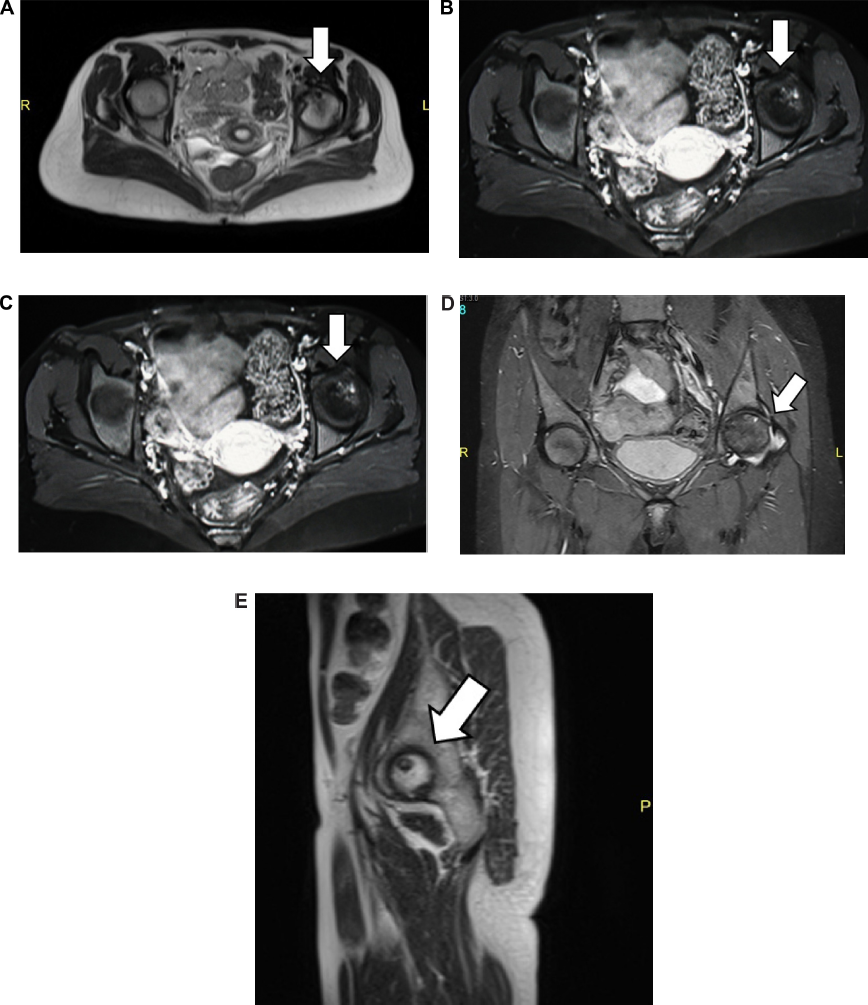
MRI of both hip joints: (A) axial view of the T2WI sequence, (B) axial view of the T1WI sequence post-contrast (gadolinium DTPA) intravenous administration, (C) coronal view of the T2WI sequence, (D) coronal T2 STIR sequence, and (E) sagittal view of the left hip joint T2WI sequence.
She underwent total hip replacement, which was successful.
Discussion
AVNFH is a recognized complication for a group of traumatic and nontraumatic disorders. The incidence of AVNFH in CML is not identified. This is because of the limited number of reports and absence of prospective studies evaluating this issue in this situation. In addition, whether the disease itself and/or the treatment encourage the development of AVNFH is not known. Post-contrast material-enhanced MRI with its inherent high spatial resolution capabilities is considered an excellent diagnostic tool for detecting and staging of femoral head AVN. It is considered the preferred method for diagnosis of occult AVN, since it is more sensitive than bone scan or plain films. Owing to the high incidence of bilateral AVN, MRI may pick up AVN in opposite asymptomatic hip. An AVN lesion is typically a well-demarcated epiphyseal area of altered and variable signal intensity (Figs. 1 and 2). In its early stages, T2-weighted images and STIR short tau-inversion recovery can help in detection of necrotic tissue in some unusual AVN lesions that mostly showed ill-delimited edema-like marrow changes.11,12 MRI has 90-100% sensitivity for symptomatic disease. In some cases, contrast-enhanced MRIs may increase diagnostic confidence by showing homogeneous hypervascularization in bone marrow edema lesions and by depicting hypovascular marrow areas in AVN lesions. Also the MRI can discriminate between the AVN and transient marrow edema.11,13 Sequential and follow-up MRI is considered valuable in the assessment of equivocal femoral head lesions, especially in its early stages where the findings are usually trivial.12,13
Treatment historically has passed through two eras. The era of interferon: there is a limited data that interferon alfa 2a can cause AVNFH. There are no reports in the literature about AVNFH with other therapeutic uses of interferon alfa. Therefore, the occurrence of AVNFH in patients with CML on interferon treatment may be the result of an interaction between CML and interferon alfa therapy. Interferon alfa can inhibit angiogenesis, which may cause AVN, and the stress of weight bearing may make the femoral head, particularly, vulnerable. 14 The second era for CML treatment started with using tyrosine kinase inhibitor (TKI) Table 3. Few cases of AVNFH have been reported at disease presentation (CML) as well as with the use of first-generation TKIs imatinib (Glivec®). Though the mechanism by which dasatinib can cause AVN is not clear, it can be postulated because of micro-circulatory obstruction of the femoral head.
Patients treated with interferon-alfa.

Patients treated with TKIs.

Era of Interferon-alfa 15 AVN in CML patients treated with interferon. Table 2 illustrates that patients with CML developed AVNFH while on interferon alfa.
Conclusion
The above mentioned review of literature states that six patients with CML presented with AVNFH as the initial presentation prior to any therapy, five in the era of interferon and two in the era with TKIs, and one with imatinib and the other with dasatinib treatment. There are two issues to be considered: either the condition is rare or there is underreporting of this side effect. Observational studies with proper reporting are required to accurately measure the incidence of this complication, which could significantly affect patients’ safety and quality of life.
Author Contributions
Conceived and designed the experiments: MAY. Analyzed the data: MAY, AHM. Wrote the first draft of the manuscript: MAY, AHM. Contributed to the writing of the manuscript: MAY, AHM. Agree with manuscript results and conclusions: MAY, AHM, AJN, ATS, HE, SFM, DSM, SE, DRA, HLGG, RMH, MAM, SK, NAD, AE. Jointly developed the structure and arguments for the paper: MAY, AHM. Made critical revisions and approved final version: MAY, AHM, AJN, ATS, HE, SFM, DSM, SE, DRA, HLGG, RMH, MAM, SK, NAD, AE. All authors reviewed and approved of the final manuscript.