
Abstract
Objective
To investigate clinical effectiveness of prednisolone (PSL) and cyclosporin A (CyA), particularly continuous intravenous administration of the latter, in patients with interstitial pneumonia (IP) associated with polymyositis/dermatomyositis (PM/DM).
Methods
We reviewed the clinical findings and therapeutic outcomes of patients with PM/DM who had received PSL and CyA (PSL + CyA, n = 21 for DM and 2 for PM) or the former alone (n = 12 for DM and 7 for PM). All patients receiving PSL + CyA had active IP.
Results
Fifteen of the 21 DM patients receiving PSL + CyA showed favorable therapeutic outcomes of IP (recovery group), while the remaining 6 died of respiratory failure (death group). Before treatment PaO2 in room air and %VC were significantly lower, and the total CT score was significantly higher in the death group than in the recovery one. Continuous intravenous administration of CyA was performed in 6 patients for severe IP requiring oxygen therapy, and of these 2 showed complete recovery from it.
Conclusions
Coadministration of PSL and CyA, particularly continuous intravenous infusion of the latter, from the early phase of illness may be a potent therapeutic option for PM/DM patients with decreases in PaO2 and %VC and/or a high total CT score suggestive of a poor prognosis.
Keywords
Introduction
Polymyositis (PM) and dermatomyositis (DM) are autoimmune inflammatory systemic disorders primarily targeting skeletal muscles with or without skin involvement. Several recent reports have demonstrated obvious differences in flow cytometry of circulating peripheral blood and immunohistochemistry of skeletal muscles between PM and DM,1–3 but both disorders are similar with regard to showing an important role of activated T-lymphocytes in the pathogenesis. 4 To control the disease activity of PM and DM via suppression of activated T-lymphocytes, calcineurin inhibitors, such as cyclosporin A (CyA) and tacrolimus, have recently been used for treatment of refractory cases unresponsive to corticosteroid alone, particularly in patients with progressive interstitial pneumonia (IP) in which many CD8-positive cells are frequently detectable in both the alveolar wall and bronchoalveolar fluid.5–7 Additional use of calcineurin inhibitors in these cases may be able to promote early recovery, save life and also reduce corticosteroid-induced adverse events.1,8–11
In the present study we retrospectively investigated the clinical outcomes of prednisolone (PSL) and CyA in acute IP complicating PM/DM in order to clarify therapeutic efficacy and adverse effects. We postulate that additional use of CyA to corticosteroid, particularly continuous intravenous administration of the former in the early phase of illness, may be a potent therapeutic option for PM/DM patients associated with IP probably showing a poor prognosis.
Patients and Methods
Patients
We studied 9 patients with PM (8 women and 1 man; mean age 65 ± 15 years, range 28 to 81) and 33 patients with DM (20 women and 13 men; mean age 52 ± 17 years, range 15 to 83) who had been admitted to our hospital from January 2002 to August 2010. The diagnoses of PM and DM were made according to the classification criteria proposed by Bohan and Peter. 12 None of the patients had received any treatment prior to admission to our hospital, and presented with some of the clinical manifestations and laboratory data suggestive of active disease, such as muscle weakness, skin symptoms and increases in serum creatine kinase (CK). Sixteen of the DM patients were compatible with clinically amyopathic DM (CADM) with regard to showing typical skin symptoms, including heliotrope rash, Gottron's sign and ulcerations, with no or little muscle involvement. 13 No patients had either malignancy on intensive systemic survey or obvious renal dysfunction on routine laboratory examinations. Other clinical information, such as C-reactive protein (CRP) and autoantibodies, was obtained from their medical records. The Local Ethical Committee approved this study.
Clinical Assessment of IP
We assessed pulmonary involvement in the patients using the following indices: chest X-ray, high resolution computed tomography (HRCT), arterial oxygen pressure (PaO2) in room air, serum KL-6 and respiratory function tests, including a percent vital capacity (%VC) and a percent diffusing capacity for carbon monoxide (%DLco). HRCT was performed using LightSpeed VCT VISION (GE Healthcare Japan; Hino, Japan), with 2-mm collimation at 15-mm intervals at end inspiration from the lung apices to the bases. All images were reconstructed with a high-spatial frequency algorithm, and photographed at window widths of –1500 H.U. and window levels of –600 H.U. To discover interstitial changes in lungs, we focus upon the following CT findings:14,15 (1) nodular opacities: (2) bronchial dilatation and wall thickening, including consolidation around bronchovascular bundles: (3) reticular opacities, including honey-comb changes: (5) linear opacities and (6) increased lung opacities. When the patients with at least one of these CT findings showed clinical symptoms, such as non-productive cough and exertional dyspnea, with impaired respiratory function, particularly decreases in PaO2 (<80 mmHg),%VC (<80%) and/or % DLco (<70%), associated IP was regarded as active. To assess IP, we selected 6 transverse CT images taken at the levels of the upper and lower portions each of the aortic arch, the hilus and the lower lobe. Two raters blinded to the clinical information (YS and MM) evaluated the HRCT images focusing the above-mentioned 6 CT findings suggestive of IP, and used the visual estimation method described by Kinoshita et al. 14 Each CT slice level was divided into 4 areas according to a horizontal and a vertical line drawn by a rater, and scored in a semiquatitative manner as follows: 0 = absent; 1 = less than 25% involved; 2 = 25%–50% involved; 3 = 50%–75% involved; and 4 = greater than 75% involved. The final judgment was reached by consensus of the 2 raters. Right and left lungs were evaluated separately, and the sum was expressed as the total CT score. HRCT was serially performed before and after treatment.
Treatment
PSL was started at a dose of approximately 1.0 mg/kg/day in all of the patients soon after the diagnosis of PM/DM. We added CyA to PSL when active IP was evident (PSL + CyA). CyA was orally given twice a day initially at a dose of 75 mg, which was later controlled to keep the trough concentration between 100 and 150 ng/mL. Continuous intravenous administration of CyA was performed when oral intake of it was difficult because of critical care for respiratory failure, such as oxygen therapy with or without mechanical ventilatory support. CyA was started at 0.17 mg/kg/hr, the blood concentration was checked at least twice a day, and in order to keep it at 250–350 ng/mL the administration speed of CyA was controlled. The dose of CyA was reduced at the development of renal dysfunction.
Statistics
To determine statistical differences between PSL alone and PSL + CyA in PM/DM and also those between recovery and death groups in DM, Mann-Whitney's U and Chi-square for independence tests were employed. Wilcoxon's signed rank test was used for evaluating alterations of the total CT score. The results were expressed as mean ± standard deviation, and a P-value less than 0.05 was regarded as statistically significant. Commercially available statistics software was used for data analysis (StatView for Macintosh, Abacus Concepts, Berkeley, CA, USA and Excel for Windows, Microsoft, Redmond, WA, USA).
Results
Clinical Profiles and Laboratory Findings before Treatment
CyA was added to PSL (PSL + CyA) in 21 patients with DM, including 11 with CADM, and 2 with PM, all of whom showed active IP on or after admission. Possibilities of infection were excluded on the basis of blood examinations, including serum antibodies to infectious agents, and analyses of bronchoalveolar lavage fluid in all of these patients. Twelve DM patients, including 5 with CADM, and 7 with PM were treated only with PSL (PSL alone). Among them 1 DM and 2 PM patients revealed mild consolidation around bronchovascular bundles and/or honey-comb changes on CT, which were regarded as old and inactive IP based on the lack of clinical symptoms with well-preserved respiratory function. Comparison of clinical profiles and laboratory data on admission between PSL alone and PSL + CyA is shown in Table 1. There was no significant difference in the initial dose of PSL between PSL alone and PSL + CyA. Among the clinical symptoms of DM, arthralgia and ulcerative skin lesions were significantly more frequent in PSL + CyA (P < 0.0001 and P < 0.001, respectively) than in PSL alone. No significant difference was seen in laboratory data between the 2 groups except for CRP in the DM patients, which showed a significantly higher value in PSL + CyA than in PSL alone (P < 0.01). The total CT score in DM showed a significantly higher level in PSL + CyA than in PSL alone (P < 0.0001).
Comparison of clinical profiles and laboratory data on admission between PSL alone and PSL + CyA.

Number of patients with amyopathic dermatomyositis,
Values in patients with non-amyopathic dermatomyositis.
Therapeutic Outcomes
Fifteen of the 21 DM patients receiving PSL + CyA (recovery group) showed favorable therapeutic outcomes of IP, including complete recovery, and no serious adverse events except for mild pneumocystis pneumonia in 2. The remaining 6 patients receiving PSL + CyA (death group) died of respiratory failure due to active IP despite methylprednisolone pulse therapy and other intensive immunomodulatory treatment, such as plasma exchange and high-dose intravenous cyclophosphamide. Three of the 6 patients had CADM. The total CT scores of each patient before and after starting coadministration of PSL and CyA are shown in Figure 1. All DM patients in the recovery group showed decreases or at least no increase in the total CT score from 1 month after starting coadministration of PSL and CyA. There were significant decreases in the total CT scores 1, 3, 6 and 12 months after starting coadministration of PSL and CyA compared with before (P < 0.05). All DM patients in the death group showed increases in the total CT score suggestive of worsening of IP even after starting coadministration of PSL and CyA, and died within approximately 3 months after admission. In PM 2 patients received PSL and CyA, and both recovered from active IP without serious adverse events, although the total CT score in 1 remained at a slightly high level owing to inactive interstitial sequellae 12 months after starting this treatment. No patients receiving PSL alone showed any life-threatening complications.

The total CT score before and after treatment in the PSL + CyA group.
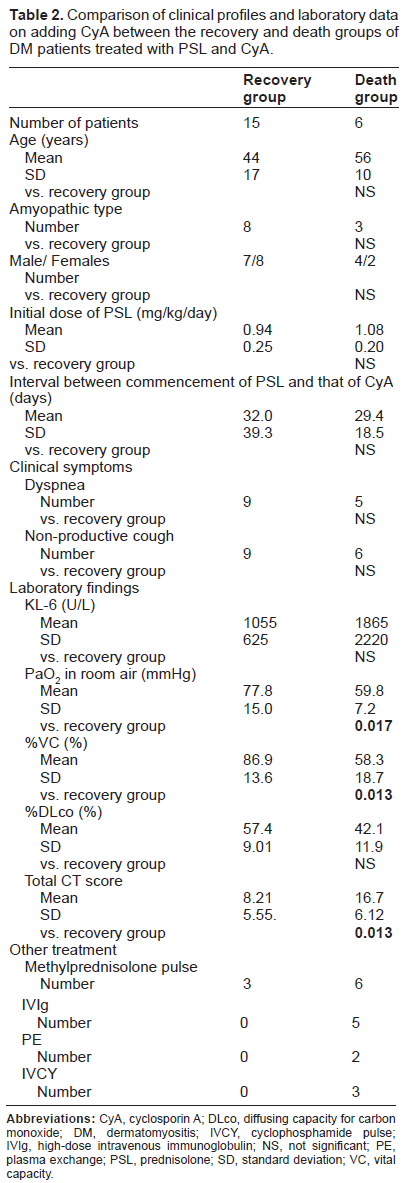
To investigate clinical indices predicting therapeutic outcomes in IP complicating PM/DM, we compared clinical symptoms and laboratory data on adding CyA in the death group with those of the recovery one (Table 2). PaO2 in room air and %VC were significantly lower in the death group than in the recovery one (P < 0.05). The death group showed lower % DLco compared with the recovery one, but no statistical difference was present. The total CT score was significantly higher in the death group than in the recovery one (P < 0.05). There was no significant difference in clinical symptoms, such as non-productive cough and dyspnea, KL-6, initial dose of PSL or the interval from commencement of PSL to that of CyA between the death and recovery groups. Other treatments, such as methyprednisolone pulse therapy and high-dose intravenous immunoglobulin, were more frequently performed in the death group than in the recovery one in order to avoid worsening of respiratory failure.
Comparison of clinical profiles and laboratory data on adding CyA between the recovery and death groups of DM patients treated with PSL and CyA.
Continuous Intravenous Administration of CYA
Continuous intravenous administration of CyA was performed in 6 DM patients, including 2 with CADM. Clinical profiles and therapeutic outcomes of these patients are summarized in Table 3. All of the patients required oxygen therapy on or after admission because of severe dyspnea and non-productive cough with low levels of PaO2 in room air, %VC and %DLco, although respiratory function tests could not be performed in some of them. The duration of continuous intravenous administration of CyA was 7 to 15 days (mean 12.5 ± 3.3 days), and the interval between admission to our hospital and commencement of this treatment was 0 to 44 days (mean 9.2 ± 17.3 days). Three patients started to receive continuous intravenous administration of CyA right after admission to our hospital because of rapidly progressive respiratory failure, and of these 2 (patients 5 and 6) completely recovered from IP. After reaching stable general status the administration route of CyA was changed from intravenous to oral in both patients. As a representative case the clinical course of patient 6 is shown in Figure 2. IP quickly improved in parallel with a decrease in serum CK and an increase in SaO2 after starting continuous intravenous infusion of CyA and methylprednisolone pulse therapy followed by PSL. The administration route of CyA was successfully changed from intravenous to oral 2 weeks after admission. Nevertheless, the remaining 1 (patient 4), who had already shown consciousness disturbance due to hypoxia on admission, showed improvement of IP only when the blood concentration of CyA was raised to 450 ng/mL or higher. Renal dysfunction ascribable to CyA quickly worsened, and the patient died of respiratory failure during tapering continuous intravenous infusion of this drug.
Clinical profiles of patients treated with continuous intravenous administration of CyA.

Discussion
In the present study we reviewed the clinical profiles of PM/DM patients who had received coadministration of CyA and PSL in order to treat associated active IP. All of the patients receiving PSL + CyA, therefore, had active IP, while those receiving PSL alone did not. Considering that the PSL + CyA group showed a significantly higher frequency of ulcerative skin lesions and arthralgia than PSL alone before treatment, DM associated with active IP may have a systemic inflammatory process affecting visceral organs, such as vasculitis, in the background, as shown in the previous report. 16 A significantly higher level of CRP in PSL + CyA than in PSL alone also supports the possible presence of systemic vasculitis in DM associated with active IP.
Oral administration of immunosuppressive agents, particularly CyA, is often employed for treatment of acute IP complicating DM in addition to PSL and methylprednisolone pulse therapy9,17,19 In the present study 15 DM patients in the recovery group showed quick decreases or at least no increase in the total CT score after starting coadministration of CyA and PSL. Nevertheless, oral CyA has been reported to sometimes fail to sufficiently avoid deterioration of IP, resulting in unfavorable outcomes even if this drug is started from the early phase of illness. 20 In the present study 6 DM patients died of respiratory failure due to acute IP despite administration of oral CyA. Among them 4 patients showed an evident delay in commencement of CyA, but in the remaining 2 both PSL and oral CyA were started almost simultaneously right after admission to our hospital in good general status with relatively low values of the total CT score. One possible cause of the unfavorable outcome is that IP was rapidly progressive. In other words, IP may have become irreversible and extensive before CyA extended immunosuppressive action. The other possible cause is that blood concentrations of CyA were not high enough to suppress the disease activity of IP. We raised the administration dose of oral CyA within several days after commencement in these 2 patients in order to keep the trough concentration between 100 and 150 ng/mL, but IP quickly worsened during this period. Oral CyA suppresses autoreactive T cells in conjunction with an increase in blood concentrations after absorption from the gastrointestinal tract. As many exogenous factors, such as food and drugs, can affect the therapeutic efficacy of oral CyA by readily modifying its absorption and metabolism, continuous intravenous administration is often employed for treatment of rejection in organ transplantation21,22 and inflammatory bowel disorders, including ulcerative colitis.23,24 In the present study 6 DM patients with active IP received continuous intravenous administration of CyA because of respiratory failure requiring oxygen therapy with or without mechanical ventilatory support. Four patients showed extensive and probably irreversible damage in both lungs at commencement of the continuous intravenous administration of CyA, finally resulting in death, while the remaining 2 received this treatment from admission to our hospital, and quickly recovered from IP. These results suggest that the continuous intravenous administration of CyA may be a potent therapeutic option in IP complicating DM, particularly in the early phase of illness, with regard to its capability of quickly elevating the blood concentration and stabilizing it.


The clinical course of patient 6, showing a decrease in CK and an increase in SaO2 during continuous intravenous infusion of CyA and methylprednisolone pulse therapy followed by PSL. The administration route of CyA was successfully changed from intravenous to oral 2 weeks after admission.
With continuous intravenous administration of CyA both therapeutic effects and adverse events, such as renal dysfunction, depend on its blood concentration. For therapeutic efficacy the appropriate blood concentration with continuous intravenous infusion has been reported to be approximately 2.55-times as high as the trough level with oral administration. 22 Considering that the appropriate trough level of CyA in the oral administration is 80–150 ng/mL, therefore, the blood concentration should be kept at approximately 200–380 ng/mL in continuous intravenous infusion. In the present study we controlled the administration speed of CyA in order to keep the blood concentration at 250–350 ng/mL. In the term of safety, adverse events ascribed to CyA have been reported to be dependent on the length of continuous intravenous administration but not on the blood concentration at 300–500 ng/mL.23,25,26 To reduce the possibility of adverse events, therefore, we need to switch the continuous intravenous infusion of CyA to oral administration as soon as possible after reaching stable general status. In the present study 2 patients showed successful transition from continuous intravenous infusion of CyA to oral administration in at most 2 weeks. Renal dysfunction with or without skin eruptions occurred in 2 patients, and of these it rapidly worsened in 1 because the blood concentration of CyA had to be maintained at 450 ng/mL or higher for 10 days in order to treat IP.
According to several recent reports the presence of autoantibodies to CADM-140 in serum and hyperferritinemia are strongly relevant to poor prognosis in IP complicating PM/DM.27,28 At the present time, however, the anti-CADM-140 antibody remains commercially unavailable. To discover other clinical factors suggestive of poor prognosis, we investigated whether or not there was a difference in laboratory data, respiratory function and the total CT score between the death and recovery groups of DM associated with IP. No significant difference was seen in laboratory data, including KL-6, but PaO2 and %VC were significantly lower and the total CT score was significantly higher in the death group than in the recovery one. Respiratory function tests showed a lower level also in %DLco in the death group than in the recovery one, although there was no statistical difference. These results suggest that respiratory function, such as PaO2, %VC and %DLco, may be useful as clinical indices predicting a poor prognosis. The continuous intravenous administration of CyA is probably adequate for DM patients with active IP who show malfunction in respiratory function tests from the early phase of illness.
In conclusion, coadministration of oral CyA with PSL is effective for IP complicating PM/DM, but its efficacy is sometimes insufficient, particularly in rapidly progressive cases. To more consistently and quickly suppress the disease activity of IP, the continuous intravenous administration of CyA might be a potent therapeutic option. Further prospective study of a larger set of patients is necessary in order to clarify the clinical usefulness of this treatment.
Author Contributions
Conceived and designed the experiments: Y. Shimojima, WI, MM. Analysed the data: Y. Shimojima, NK, KT, MM. Wrote the first draft of the manuscript: Y. Shimojima. Contributed to the writing of the manuscript: MM, SI. Agree with manuscript results and conclusions: Y. Shimojima, WI, MM, NK, KT, Y. Sekijima, SI. Jointly developed the structure and arguments for the paper: Y. Shimojima, WI, Y. Sekijima, NK, KT, MM. Made critical revisions and approved final version: WI, MM. All authors reviewed and approved of the final manuscript.
Funding
This work was supported by grant from Mitsubishi Tanabe Pharma and the Health and Labour Sciences Research Grant on Intractable Diseases (Neuroimmunological Diseases) from the Ministry of Health, Labour and Welfare of Japan.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.