
Abstract
The prognostic significance of early diagnosis and therapeutic intervention in inflammatory rheumatic diseases has been well documented. However, a shortage of rheumatologists often impedes this approach in clinical practice. Therefore, it is of importance to identify those patients referred for diagnosis who would benefit most from a specialist's care. We applied a telephone-based triage for appointment allocation during routine care. This retrospective, monocentric analysis evaluated the efficacy of our triage to identify patients with rheumatic disease with special regard to initial appointment category (elective, early arthritis clinic (EAC), or emergency appointment). Of the 1,782 patients assessed, 718 (40.3%) presented with an inflammatory rheumatic disease, and there were significant discrepancies between the appointment categories: elective 26.2%, EAC 49.2% (
Introduction
An extensive body of evidence indicates that early diagnosis and therapeutic intervention with consistent maintenance of remission, known as
Several guidelines, including those of the German Rheumatology Association (DGRh), recommend that a rheumatologist should see every patient with at least two swollen joints and no other explanatory diagnosis no later than 6 weeks following the onset of symptoms, and treatment with disease-modifying anti-rheumatic drugs (DMARDs) should begin no later than 12 weeks after the onset of symptoms.13–16 However, data from the German national database centers show that patients with RA consult a rheumatologist only an average of 1.1 years after the onset of symptoms, which means that DMARD treatment commences only after a considerable delay in most cases. 17
Various factors at patient level and at general practitioner and rheumatologist level delay the early initiation of specific immunomodulatory treatment.18–20 One particularly significant obstacle is that some patients may wait several months for an appointment with a rheumatologist in Germany, a symptom of inadequate capacity for rheumatologic diagnosis and treatment. The waiting time for first consultation with a rheumatologist in Germany was 5.74 ± 6.60 weeks (median 3.57; interquartile range (IQR) 1.72–7.81) in 2008. 21 The shortage of rheumatologic treatment capacity affects the diagnostic work-up of suspected cases of inflammatory rheumatic systemic diseases and the ability to maintain constant remission (the treat-to-target or tight control approach) during the patient's further care.22–25 This deficit is significantly intensified because patients with primary pain conditions or primary degenerative diseases of the musculoskeletal system often crowd the schedules of rheumatologists, who are then no longer available to diagnose and treat patients with inflammatory rheumatic systemic diseases.
Recent attempts to facilitate priority access to rheumatologic diagnostics and treatment were made for patients with strongly suspected inflammatory rheumatic disease by setting up early arthritis clinics (EACs). Various methods and approaches were used with varying degrees of success.26,27 The goal of this study was to develop a simple triage system that would enhance appropriate access of patients with rheumatic diseases to specialized medical care.
Materials and Methods
Our rheumatologic facility offers outpatient (>6,500 outpatient cases per annum) and inpatient care (academic teaching hospital) for adults, and it has a catchment area of approximately 100–150 km, which is mostly rural and corresponds to approximately 400,000 inhabitants. The digital patient files of 1,782 initial outpatient consultations between January 2015 and March 2016 were retrospectively analyzed. All patients were referred following consultation with a physician.
Appointments were scheduled after a simple telephone-based triage (Fig. 1) that was implemented as part of the clinical routine. There were three appointment categories to which the patients were allocated: elective initial appointment, EAC, and emergency appointment (Fig. 1A). Medical staff with several years of professional experience answered all telephone calls of patients referred for diagnosis. All patients had been previously seen by a doctor, usually a family doctor or an orthopedic specialist. On requesting an appointment, each patient was first asked during the appointment request whether he/she had already been diagnosed with an inflammatory rheumatic disease (list). If the answer was no, then he/she was asked about symptom duration (≤ or >6 months) and whether any abnormal laboratory findings specific to rheumatic disease were noted. If an appointment was requested by the referring practice itself, then an appointment in one of the three available categories was assigned solely based on the referring doctor's assessment of the case's urgency (Fig. 1B). Emergency appointments were given solely in response to an inquiry by a physician. The waiting time for an elective appointment was 12–16 weeks, 4–6 weeks for EAC, and no longer than 2 weeks for an emergency appointment. All patients were seen by a rheumatologist.

Triage algorithm for calls by a patient (A) or doctor (B).
Diagnoses were categorized as follows: noninflammatory (eg, osteoarthritis, fibromyalgia), RA, axial spondyloarthritis, peripheral spondyloarthritis, arthritis of other form (eg, arthritis urica, Lofgren's syndrome), inflammatory of other form (eg, polymyalgia rheumatica, autoinflammatory syndromes), connective tissue diseases, and vasculitis. Erythrocyte sedimentation rate (ESR) was ascertained using the Westergren method (normal value 6–11 mm during the first hour). Highly sensitive C-reactive protein (CRP) levels were measured using particle-enhanced immunonephelometry (F. Hoffmann-La Roche Diagnostics; normal value <0.5 mg/dL).
Data were assessed during routine care according to available recommendations and guidelines. No further inclusion or exclusion criteria were used. Data management and statistical analyses were performed for all data as appropriate using Microsoft Excel and SPSS, respectively.28,29 All performed inferential tests were two-tailed and considered statistically significant at
Results
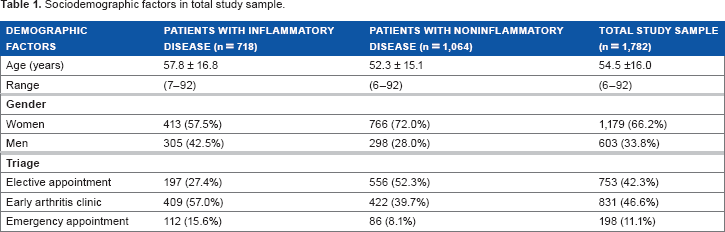
A total of 1,782 datasets were evaluated (Table 1). The percentage of inflammatory diagnoses in the entire collective was 40.3%. Inflammatory rheumatic disease was excluded in 59.7% of cases (Fig. 2).
Sociodemographic factors in total study sample.

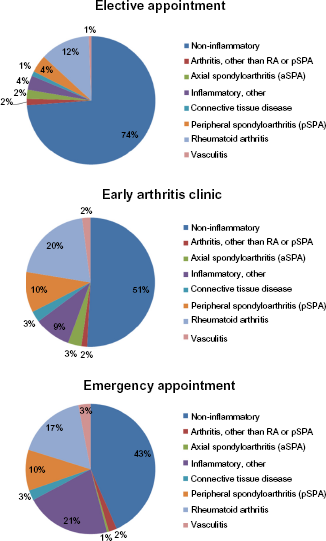
Diagnostic categories in the collective.
The percentage of inflammatory rheumatic diseases was 26.2% in the elective group, 49.2% in the EAC group, and 56.6% in the emergency group (Fig. 3). Significantly more patients with inflammatory rheumatic diagnoses (
Percentage of inflammatory vs. noninflammatory diagnoses in each appointment category (*
The percentage of cases in the diagnostic category “Inflammatory, other” in the emergency group (21.2%) was significantly higher than in the other two appointment categories, ie, EAC and elective. Of the emergency patients in this diagnostic category, 140 were diagnosed with polymyalgia rheumatica. RA was the most common inflammatory rheumatic diagnosis in the other two appointment groups. The higher percentage of inflammatory diagnoses in the EAC and emergency groups was reflected in the higher percentage of patients receiving specific treatment. Significantly more patients in the emergency group were treated with glucocorticoids than in the elective appointment group (

Percentage of patients receiving specific treatment in each appointment category (*
Of the patients with an inflammatory diagnosis, 56.5% exhibited a normal CRP count. However, the percentage of pathological CRP values was significantly higher in the emergency group than in the EAC and elective appointment groups (

Percentage of patients with elevated CRP (*
Binary logistic regression analysis revealed that 61.2% of all patients interviewed by triage were allocated to the correct (dichotomized) diagnostic category, ie, inflammatory or noninflammatory. The probability of a noninflammatory diagnosis being correctly predicted on the basis of telephone triage was 61.74% npv. The ppv was 56.56%. A total of 66.8% of patients were allocated to the correct category (inflammatory or noninflammatory) on the basis of CRP values alone, and 62.4% of patients were correctly allocated based on ESR values. A simultaneous inclusion of telephone-based triage and CRP values in the mathematical regression model resulted in 67.1% of patients being correctly allocated to the inflammatory or noninflammatory group (npv 68.0%, ppv 64.2%).
Discussion
Rheumatologic care in Germany is marked by a demand that far exceeds the diagnostic and therapeutic capacities available in this field. This increased demand of patients and referring physicians is the result of the considerable attention devoted to inflammatory rheumatic diseases by the media, the publicity work performed by patient associations, and the increased efforts by scientific organizations to educate referring physicians. However, data published by DGRh shows that the number of new consultants in the field of internal medicine specializing in rheumatology in Germany between 1991 and 2014 remained largely stagnant at between 35 and 71 per annum, which just compensates for physicians leaving the profession on demographic grounds. This means that the number of rheumatologists (including those specializing in orthopedic rheumatology) has essentially remained the same, with 1.56 rheumatologists per 100,000 inhabitants serving Germany's population in 2012 compared to 1.45 rheumatologists per 100,000 inhabitants in 2002. 30 This situation clearly undermines treatment concepts, such as the early diagnosis and initiation of treatment within three months (window of opportunity) and the consistent maintenance of remission (tight control, treat to target), despite the large body of scientific evidence supporting their effectiveness. These shortcomings support the need for strategies for the selection of patients referred for diagnosis to identify those patients who would benefit most from early diagnosis and therapeutic intervention.
The average time that elapses between the onset of symptoms and diagnosis in RA is currently 1.1 years, but this period has been shortened in recent years.17,26,31 In 2008, 198 internal-rheumatologic treatment facilities were questioned as part of a study conducted by the German Rheumatism Research Center, Berlin (DRFZ), and the Society of German Rheumatologists (BDRh); 19,908 patients (average age 55 ± 16 years, 67% women) were documented. 21 Family doctors referred the majority (79%) of these patients, and only 23% managed to see a rheumatologist within three months of their symptoms onset. A Belgian study has found that diagnosis was delayed an average of 10 weeks at the patient level, 4 weeks at the family doctor level, and 7 weeks at the rheumatologist level. 32 Only a minority of patients (21.6%) in that study were diagnosed within 12 weeks of the onset of symptoms. Various, mostly nonselective, approaches were used to shorten the time between symptom onset and the first visit to the family doctor. Concepts based purely on screening programs for the general population (eg, simple hand function tests, a Rheumatism Bus, and similar methods) or information on the Internet yielded a reliable diagnosis of RA only in 0.2%–1.5% of cases.33,34 Notably, a study conducted by Deane et al yielded a diagnosis of RA in only 1.5% of the 601 patients surveyed, and the percentage of subjects who tested positive for rheumatoid factor (RF) or anti-citrullinated peptide antibodies was 6.1%. A questionnaire-based screening of patients with a reliable diagnosis of psoriasis vulgaris, ie, a collective with a comparatively high pretest probability of psoriatic arthritis, led to an actual diagnosis of psoriatic arthritis in 10.1% of cases. 35 This study demonstrated that preselection at this level significantly increased the likelihood of the diagnosis of an inflammatory rheumatic disease. The next level refers to the period that elapsed between the patient contacting his family doctor and consultation with a rheumatologist. Many studies report that this period is particularly critical. Approximately 22% of patients consult their family doctors because of pain, and 50% of these patients have musculoskeletal complaints. 36 Therefore, it is initially understandable that not every patient is or must be referred to a rheumatologist immediately, and these patients generally see their family doctors up to four times before being referred. 37 Two studies explored the usefulness of medical information on the family doctor's referral slip in helping the rheumatologic institution stratify appointments. These studies used three categories of urgency, similar to our study. The ppv of inflammatory joint disease in patients referred by their family doctor as especially urgent cases was between 56.5% and 75%, which is comparable with our results.38,39 The percentage of inflammatory diagnoses in our collective data also conforms with current results from the EACs in Leiden and Groningen, which were calculated at 42% and 49%, respectively. 40 Although the referral system and the number of available rheumatologists certainly differ between countries and rheumatology units, the results seem to be comparable.
The rate of inflammatory diagnoses at our emergency clinic (56.6%) was significantly higher (
Graydon and Thompson 38 reported that 17% of the patients examined during routine care by a rheumatologist should have received earlier referrals. One major reason for the erroneous initial assessment of the urgency of these cases was incomplete information on existing diagnoses, symptom duration, and joint involvement in the referral document in more than 30% of cases. This finding confirms our own experience with the information provided in referral documents, which is frequently incomplete and varies considerably in quality. A total of 26.2% of patients in our elective referral cohorts also exhibited inflammatory rheumatic disease that would have qualified them for early appointments.
More complex appointment stratification systems comprise up to eight parameters, including family history, clinical findings, laboratory results (ESR, RF), and conventional X-ray findings. 40 The ppv of inflammatory rheumatic disease was just 49% with ≥3 of 8 abnormal parameters, and any added value is negated by the increased outlay compared to a ppv of 64.2% based on our triage and CRP count. The delegation of such a comprehensive procedure to the family doctor seems to be impracticable because of the limited time and financial resources available and the limited experience of most primary care physicians in evaluations of earlier undifferentiated stages of these diseases. The diversity of inflammatory rheumatic diseases precludes the delineation of a single set of parameters that could be easily implemented by family doctors to provide an equally good representation of all rheumatic diseases. 41
The so-called rapid access services use a completely different approach. These services involve a short, direct, symptom-based screening of all patients by an experienced rheumatologist without any preselection. If an inflammatory rheumatic disease is suspected, then another appointment is made to clarify the case in detail, or the patient is advised to consult other medical disciplines. The waiting time to see a rheumatologist for the first time was considerably shortened by this approach. 41 Puchner et al. 42 described a modification of the rapid access service model in which the patient's progress was checked six months later. The percentage of patients who experienced symptoms for less than 3 months was 43%. Suspected RA was subsequently confirmed in 93% of cases.
Unfortunately, we cannot make any statements on the value for correct appointment stratification of individual parts of the three-part triage (reliable diagnosis of inflammatory rheumatic disease already made, symptom duration, and unusual laboratory findings) because there was no separate differentiation of the criteria used to allocate the appointments. The value of the laboratory findings in detecting early stages of inflammatory rheumatic disease may be especially interesting in future studies. Notably, elevated CRP was found in 23.71%, 28.61%, and 42.31%, and accelerated ESR was found in 38.57%, 44.54%, and 52.75% of the elective referral, EAC, and emergency groups, respectively. Logistic regression analysis demonstrated that elevated CRP was even superior to the triage described here as a criterion for the allocating of patients to the inflammatory or noninflammatory groups. However, a high percentage (56.5%) of patients with a proven diagnosis of inflammatory rheumatic disease did not have elevated CRP values, which suggests that elevated CRP is unsuitable as a sole marker for rheumatologic consultations. Therefore, the combination of a triage, such as the method described here, and an elevated CRP count is likely the most effective criterion for allocation.
Patients with noninflammatory diseases, of course, should also receive a thorough investigation by a specialist and advice on the best possible care available. However, the rheumatologic care that is available cannot be expanded at will, and balancing this entitlement with the need for the earliest possible diagnosis and treatment of inflammatory rheumatic disease means that a triage is indispensable in the future. The concept presented in this work shows that three simple, delegable, standardized decision pathways to allocate appointments on the basis of a referral by a primary care physician may significantly increase the percentage of inflammatory rheumatic diagnoses in first-time patients and facilitate the implementation of current diagnostic and treatment recommendations.
Conclusion
Rheumatologic care in Germany and many other countries is marked by a demand that by far exceeds the diagnostic and therapeutic capacities available in this field. This shortage clearly undermines treatment concepts such as early diagnosis and initiation of treatment and consistent maintenance of remission. In the collective of referrals to our outpatient rheumatology clinic under routine conditions, only a total of 718 (40.3%) of the 1,782 patients assessed were diagnosed with an inflammatory rheumatic disease, and there were significant differences between the appointment categories in this regard. The applied telephone-based triage concept for appointment stratification helped to significantly increase the percentage of referred patients who were diagnosed with inflammatory disease and the percentage of referred patients who began a specific immunomodulatory treatment. According to our analyses, the combination of a triage and an elevated CRP count yields the highest predictive power regarding total correct group allocation.
Author Contributions
Conceived and designed the experiments: MF, APN. Analyzed the data: MF, AS. Wrote the first draft of the manuscript: MF. Contributed to the writing of the manuscript: MF, APN, MRK, AS. Agreed with manuscript results and conclusions: MF, APN, MRK, AS. Jointly developed the structure and arguments for the paper: MF, APN, MRK, AS. Made critical revisions and approved the final version: MF, APN, MRK, AS. All the authors reviewed and approved the final manuscript.
Footnotes
Acknowledgment
We thank Nadine Kaltenhauser for data entry.