
Abstract
Background
Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver disease and one of the most common indications for liver transplantation in adults. There are conflicting data regarding characteristic findings of PSC disease on endoscopic retrograde cholangiography (ERCP). We undertook this study to clarify whether there is a specific pattern of involvement of the biliary tract in patients with PSC and to evaluate features of PSC disease on ERCP in order to be able to manage this disease better.
Methods
This retrospective study included 45 patients admitted to Taleghani Hospital in 2004-2010 and diagnosed to have PSC on the basis of typical cholangiographic findings in combination with clinical and laboratory data. Patients suspected to have secondary sclerosing cholangitis were excluded. Demographic and clinical data were recorded, along with cholangiographic findings and the frequency of large duct and small duct PSC.
Results
Forty-five patients of mean age 34.8 (range 15-66) years were included. Twenty-nine patients (64.4%) had inflammatory bowel disease, and the frequency of large duct PSC and small duct PSC was 93.4% and 6.6%, respectively. The intrahepatic ducts alone were involved in 11 (24.4%) patients and the extrahepatic ducts were involved in 14 (31.1%), with 17 (37.7%) patients having both intrahepatic and extrahepatic PSC. Three (6.6%) patients did not have bile duct involvement on ERCP, and their disease was diagnosed by liver biopsy as small duct PSC. The most common type of cholangiographic feature of intrahepatic duct involvement was type 2, found in 15 (33.3%) patients, with type 3 being the most common type of extrahepatic duct involvement and detected in 16 (35.5%) patients.
Conclusion
Our study demonstrates that the most common PSC finding on ERCP is involvement of both the extrahepatic and intrahepatic bile ducts, with small duct PSC being less common than large duct PSC.
Keywords
Introduction
Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver disease and one of the most common indications for liver transplantation in adults. PSC is characterized by recurrent fever, pain, and jaundice, resulting from fibrosing and inflammatory obstruction of the bile ducts.1–3 Diagnosis of PSC is based on typical cholangiographic findings in the setting of consistent clinical, biochemical, serologic, and histologic findings, after exclusion of secondary causes of sclerosing cholangitis. Endoscopic retrograde cholangiography (ERCP) is considered the gold standard for establishing a diagnosis of PSC and provides a method for tissue sampling that is unavailable with other imaging modalities, and additionally provides a means for palliative measures.4,5
Both the extrahepatic and intrahepatic bile ducts are abnormal in approximately 75% of patients. The intrahepatic ducts alone are involved in 15%-20% of cases.6–9 Abnormalities of the extrahepatic biliary tree in the absence of intrahepatic involvement are less common.10,11 The cystic duct and gallbladder may be involved in up to 15% of cases, but may not be visualized well on routine cholangiography. 12 Pancreatic duct irregularities similar to those seen in chronic pancreatitis may occasionally be noted.13,14
The frequency of diagnosis of PSC has increased dramatically in the last 20 years. This increase likely reflects increased clinical awareness and use of ERCP We conducted this study to investigate the frequency of large duct and small duct PSC and the characteristic hepatic and extrahepatic bile duct findings on ERCP. 2
Methods
In this retrospective study, we identified 221 patients who were admitted to the Department of Gastroenterology at Taleghani Hospital in 2004-2010 with a diagnosis of sclerosing cholangitis. Of these, 45 patients were diagnosed to have PSC by a gastroenterologist experienced in ERCP, based on typical cholangiographic findings in combination with clinical and laboratory data with or without magnetic resonance cholangiopancreatography and liver biopsy. Patients with suspected secondary causes of sclerosing cholangitis due to choledocholithiasis, cholangiocarcinoma, lymphoma, pyogenic cholangitis, chronic pancreatitis, congenital abnormalities, or primary biliary cirrhosis were excluded. Demographic and clinical information, all cholangiographic findings, and the frequency of large duct and small duct PSC were recorded. Cholangiographic findings were reviewed retrospectively. The severity of bile duct strictures was scored using a classification system validated for PSC patients 15 (Table 1). Ethical approval was obtained for the use of human subjects in this research.
Ductal scoring system.

Results
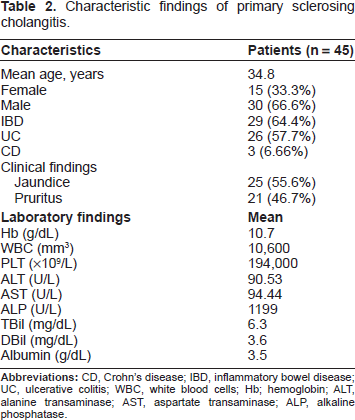
A total of 45 patients were included. Mean age was 34.8 (range 15-66) years. Fifteen patients (33.3%) were female and 30 (66.6%) were male. Twenty-nine (64.4%) patients had inflammatory bowel disease, 57.7% as a result of ulcerative colitis and 6.6% because of Crohn's disease. Forty-three patients were nonsmokers, and cirrhosis was detected in eight (17.8%) patients and gallstones in 13 (28.9%). Nine (20%) patients had undergone partial colectomy and two (4.4%) p had had total colectomy.
Among these patients, 46.7% had pruritus and 55.6% had jaundice. In one patient with inflammatory bowel disease, PSC was diagnosed before the onset of inflammatory bowel disease. Demographic characteristics and laboratory values are shown in Table 2.
Characteristic findings of primary sclerosing cholangitis.
The frequency of large duct PSC was 93.4%. The intrahepatic ducts alone were involved in 11 (24.4%) patients and the extrahepatic ducts were involved in 14 (31.1%), with 17 (37.7%) patients having both intrahepatic and extrahepatic PSC. Three (6.6%) patients did not have bile duct involvement on ERCP and their disease was diagnosed by liver biopsy as small duct PSC.
The most common type of cholangiographic feature of intrahepatic duct involvement was type 2 in 15 (33.3%) patients, and type 3 was the most common type of extrahepatic duct involvement detected in 16 (35.5%) patients. Characteristic ERCP findings for bile duct strictures are shown in Table 3.
Characteristic endoscopic retrograde cholangiography bile duct stricture findings.

Discussion
PSC is often seen in association with inflammatory bowel disease, and visualization of the biliary tract is essential for confirmation of a diagnosis of PSC. Increased physician awareness and accessibility of ERCP allow earlier recognition of the disease in the asymptomatic stage.2,16
In most cases of PSC, multifocal bile duct strictures alternating with normal caliber bile ducts or dilated bile duct segments are found throughout the intrahepatic and extrahepatic biliary tree and are responsible for the beaded cholangiographic appearance characteristic of the disease. 17 The strictured segments are usually short, annular, or band-like in appearance, although longer confluent strictures may be seen in more advanced disease. In addition, Craig et al found that type and location of bile duct involvement can be a prognostic factor because high-grade intrahepatic bile duct strictures (greater than 75% narrowing) and diffuse intrahepatic strictures are associated with a 19% decrease in three-year survival. 18 Kaplan et al reported 0.92 cases per 100,000 and 0.15 cases per 100,000 person-years for an annual incidence of large duct PSC and small duct PSC, respectively, indicating that small duct PSC is less common than large duct PSC. 19
In our study, the frequency of large duct PSC and small duct PSC was 93.4% and 6.6%, respectively. In the literature, both extrahepatic and intrahepatic bile duct involvement is reported in approximately 75% of cases, with intrahepatic duct involvement alone in 15%-20% of cases.6–9 Abnormalities of the extrahepatic biliary tree in the absence of intrahepatic involvement are reported to be less common,9,10 which is concordant with our findings. However, 37.7% of our cases had both intrahepatic and extrahepatic duct involvement, which is less than reported elsewhere.
The literature also suggests that the extrahepatic ducts are normal and the changes are confined to the intrahepatic and proximal extrahepatic ducts in about 20% of cases, but we detected a 24% frequency of intrahepatic biliary involvement and a 31.1% frequency of extrahepatic biliary tree abnormalities. 20 However, there was a relative small number of patients in our study and we did not include an appropriate control group, so further studies with larger sample sizes and appropriate controls are required.
Conclusion
Our study demonstrates that the most common ERCP finding for PSC is involvement of both the extrahepatic and intrahepatic bile ducts, with small duct PSC being less common than large duct PSC.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Publish with Libertas Academica and every scientist working in your field can read your article
“I would like to say that this is the most author-friendly editing process I have experienced in over 150 publications. Thank you most sincerely.”
“The communication between your staff and me has been terrific. Whenever progress is made with the manuscript, I receive notice. Quite honestly, I've never had such complete communication with a journal.”
“LA is different, and hopefully represents a kind of scientific publication machinery that removes the hurdles from free flow of scientific thought.”
Available to your entire community free of charge
Fairly and quickly peer reviewed
Yours! You retain copyright