
Abstract
Background:
This study investigated the safety of endoscopic sphincterotomy in patients undergoing antithrombotic treatment.
Methods:
From January 2014 to December 2016, a single-center retrospective study was conducted. Of the 80 patients with naïve papilla receiving antithrombotic treatment who underwent endoscopic sphincterotomy, 76 patients were retrospectively analyzed. We divided the participants into two groups as follows: 45 patients who discontinued antithrombotic treatment (discontinuation group) and 31 patients who continued antithrombotic treatment (continuation group). We evaluated the safety of endoscopic sphincterotomy in patients with naïve papilla who received antithrombotic treatment.
Results:
The percentage of patients requiring emergency endoscopic retrograde cholangiopancreatography in the continuation group was significantly higher than that in the discontinuation group (55% vs 11%; p = 0.001). The incidence of adverse events did not differ significantly between the two groups. Neither bleeding nor perforation occurred in either group. The length of hospital stay did not differ significantly between the two groups.
Conclusions:
Endoscopic sphincterotomy in patients undergoing antithrombotic treatment may be safe if the guidelines for gastroenterological endoscopy in patients undergoing antithrombotic treatment are followed.
Keywords
Introduction
In recent years, the number of patients with cerebrovascular disease and cardiovascular disease has increased due to the aging population. Antithrombotic agents, including antiplatelet agents and anticoagulants, are used to reduce the risk of thromboembolic events. However, withdrawal of antithrombotic agents may lead to various consequences, some of which may be serious. Therefore, it is necessary to consider not only the bleeding risk associated with antithrombotic treatment but also the thromboembolism risk associated with antithrombotic treatment withdrawal.
In Japan, the guidelines for gastroenterological endoscopy in patients undergoing antithrombotic treatment (JGES GL) were published in 2012. 1 Furthermore, a supplemental version of the guidelines was published in 2017 following the availability of various direct oral anticoagulants (DOACs). Endoscopic sphincterotomy (EST) is classified in gastroenterological endoscopy as having a high risk of bleeding. JGES GL recommends that aspirin can be continued in patients with a high risk of bleeding if the risk of thromboembolism is high.
Few reports have been published regarding EST in patients undergoing antithrombotic treatment. Therefore, the aim of this study was to investigate the safety of EST in patients undergoing antithrombotic treatment.
Methods
This retrospective study was conducted at Showa University Hospital and was approved by the Medical Ethics Committee of the facility. The study was registered with the University Hospital Medical Information Network (UMIN) Clinical Trials Registry (000030031). We obtained written consent for the procedure from all patients before the endoscopic treatment.
Patients
From January 2014 to December 2016, a total of 1597 patients underwent endoscopic retrograde cholangiography (ERCP)-related procedures at our institution. Eighty of the 433 patients with naïve papilla underwent antithrombotic treatment. Following the exclusion of those with an altered gastrointestinal anatomy (n = 4), we analyzed the remaining 76 patients receiving antithrombotic treatment who underwent EST.
We retrospectively divided the participants into two groups: 45 patients who discontinued antithrombotic treatment (discontinuation group) and 31 patients who continued antithrombotic treatment (continuation group) (Figure 1).
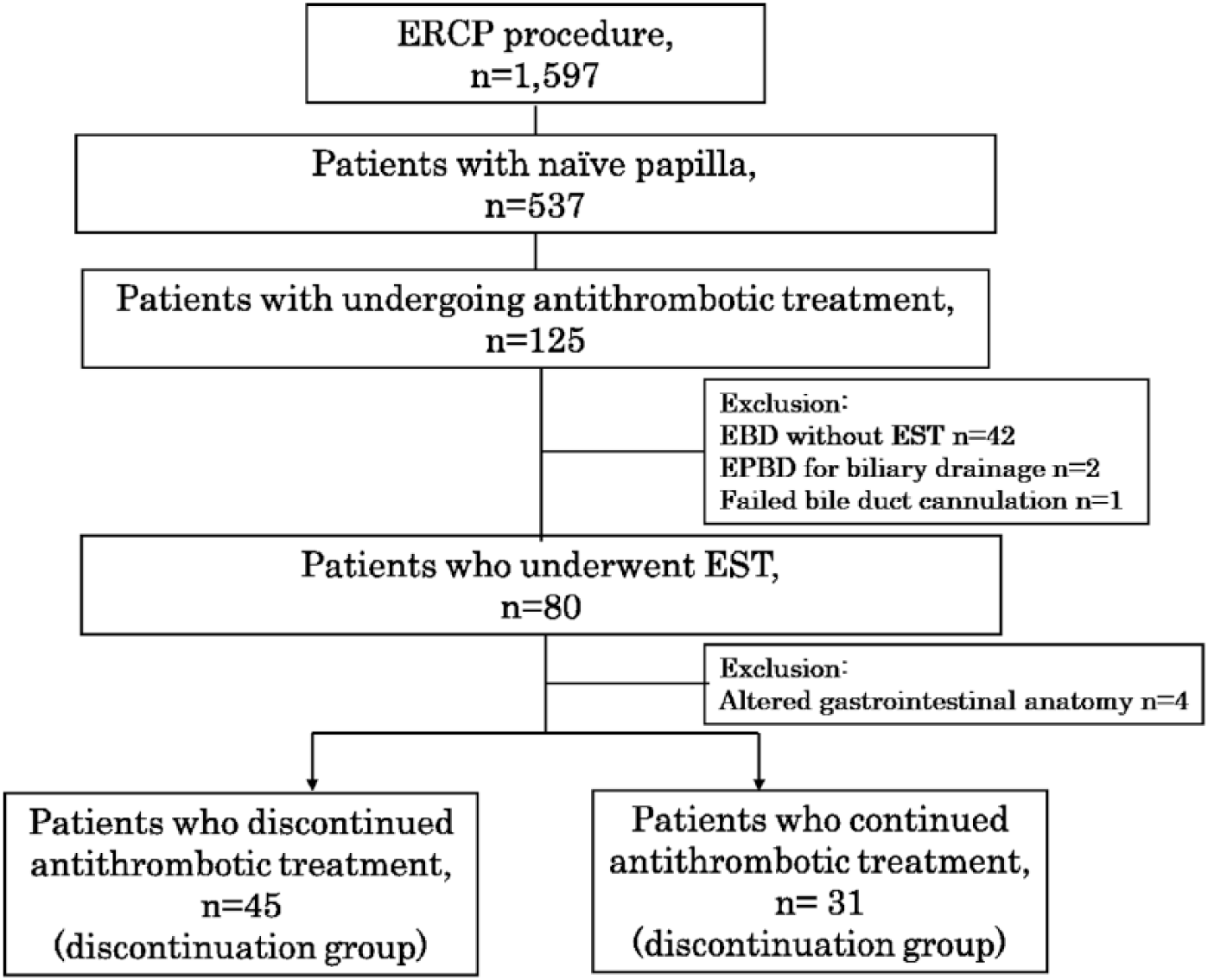
Flow Diagram.
Devices
A duodenoscope (JF – 260 V; Olympus Medical Systems Corp., Tokyo, Japan) was used for ERCP. The following equipment was used for the treatment: a sphincterotome with a tip length of 7 mm and a cutting wire with a length of 20 mm (Autotome RX44; Boston Scientific, Natick, MA, United States), a 0.035-inch guidewire (Jagwire; Boston Scientific), and a 5-Fr pigtail nasobiliary drainage catheter (Create Medic Co. LTD., Tokyo, Japan) or the 7-Fr 10 cm double pigtail stent delivery system Through Pass (Gadelius Medical K.K., Tokyo, Japan) as a drainage catheter or stent.
EST procedure
All ERCP procedures were performed by professional endoscopists. ‘Professional endoscopists’ are defined as endoscopists with a specialist qualification in Japan Gastroenterological Endoscopy Society. All patients submitted written consent before undergoing ERCP after understanding the risks and benefits of the procedures. The patients with stable vital signs received ERCP under sedation with benzodiazepines, pentazocine or pethidine. Benzodiazepine was used as a sedative agent, and pentazocine or pethidine was used as an analgesic when ERCP was performed. At that time, no analgesic or sedative agents were used for patients who had disturbed consciousness due to septic shock.
We performed wire-guided cannulation for selective bile duct cannulation and EST with a small- or medium-sized incision of the papilla of Vater. The size of EST was similar in all patients. EST was performed in Endocut mode, and an Erbotom ICC 200 (ERBE Elektromedizin GmbH, Tubingen, Germany) was used for the procedure. In the Endocut mode settings, the influence of the three currents is set to an output limit of 120 W, and the forced coagulation current is set to an output limit of 30 W. All patients were intravenously injected with a protease inhibitor [gabexate mesilate (600 mg) or nafamostat mesilate (60 mg)] for approximately 12 h (starting immediately after the ERCP procedure). A 5-Fr pancreatic duct stent was inserted to prevent post-ERCP pancreatitis when bile duct cannulation was performed by the pancreatic duct guide wire technique or pancreatic sphincter precutting. In this study, nonsteroidal anti-inflammatory drugs were not used to prevent post-ERCP pancreatitis.
For patients who required endoscopic biliary drainage (EBD), a 5-Fr drainage catheter or a 7-Fr 10 cm double pigtail stent was inserted based on the judgment of the endoscopist. Emergency ERCP was defined as ERCP within 48 h from the onset of acute cholangitis (AC), cholecystitis, or biliary pancreatitis.
Off period for antithrombotic agents in the group with a high risk of bleeding according to JGES GL
The off period for antithrombotic agents conformed to the Japanese guidelines for gastroenterological endoscopy in patients undergoing antithrombotic treatment. 1
Aspirin monotherapy can be continued in patients at high risk for thromboembolism. For patients with a low risk of thromboembolism, it is recommended that aspirin be discontinued for 3–5 days. It is also clearly stipulated that non-aspirin antiplatelet agents should be discontinued in JGES GL. Thienopyridine derivatives should be discontinued for 5–7 days. Replacing these agents with aspirin or cilostazol is recommended for patients with a high risk of thromboembolism during the drug withdrawal period. Warfarin or dabigatran should be replaced with heparin. After the withdrawal of warfarin, it should be confirmed that the prothrombin time-international normalized ratio is <1.5 before the procedure. DOAC should be withdrawn on the procedure day. Patients with more than 2 types of antithrombotic agents should be discontinued from one or more of drugs to meet this requirement.
Outcome measures
The primary outcome of this study was the incidence of adverse events associated with EST in patients undergoing antithrombotic treatment. Secondary outcomes were the time to resumption of antithrombotic agents and length of hospital stay.
Bleeding complications were classified as follows: mild bleeding was defined as cases of hemoglobin reduction <3 g with no need for transfusion; moderate bleeding was defined as patients requiring less than 4 units of transfusion without angiographic intervention or surgery; and severe bleeding was defined as patients requiring more than 5 units of transfusion or additional intervention. 2 Post-ERCP pancreatitis was defined as a case in which the serum amylase level was 3 times the upper limit of normal or higher with abdominal pain lasting more than 24 h after ERCP. Contrast-enhanced computed tomography (CE-CT) was performed as necessary, and the CE-CT grade was confirmed. The time to resumption of antithrombotic agents was based on the judgment of the physician.
Statistical analyses
We expressed continuous variables as medians with interquartile ranges (IQRs). Statistical analyses were performed using JMP version 12 (SAS Institute Inc., Cary, NC, United States). The data were analyzed using the Mann–Whitney U and χ2 tests. Differences at P < 0.05 were considered significant.
Results
Patient characteristics
The patient characteristics are shown in Table 1. There were no significant differences between the groups regarding age, sex, etiology, common bile duct diameter, periampullary diverticulum, or the Charlson Comorbidity Index. 3 The percentage of patients with AC in the continuation group was significantly higher than that in the discontinuation group (58% vs 18%; p = 0.003). The percentage of patients with acute cholecystitis in the continuation group was significantly higher than that in the discontinuation group (16% vs 2%; p = 0.027).
Patient Characteristics.

CBD, common bile duct; IQR, interquartile range.
Mann-Whitney U test.
χ2 test.
Number of antithrombotic agents
The number of antithrombotic agents used by the patients is shown in Table 2. The percentage of patients using 1 anticoagulant in the discontinuation group was significantly higher than that in the continuation group (27% vs 7%; p = 0.004).
Number of Antithrombotic Agents.

χ2 test.
Emergency ERCP
The percentage of patients who underwent emergency ERCP in the continuation group was significantly higher than that in the discontinuation group (55% vs 11%; p = 0.001) (Table 3).
Clinical Outcomes.
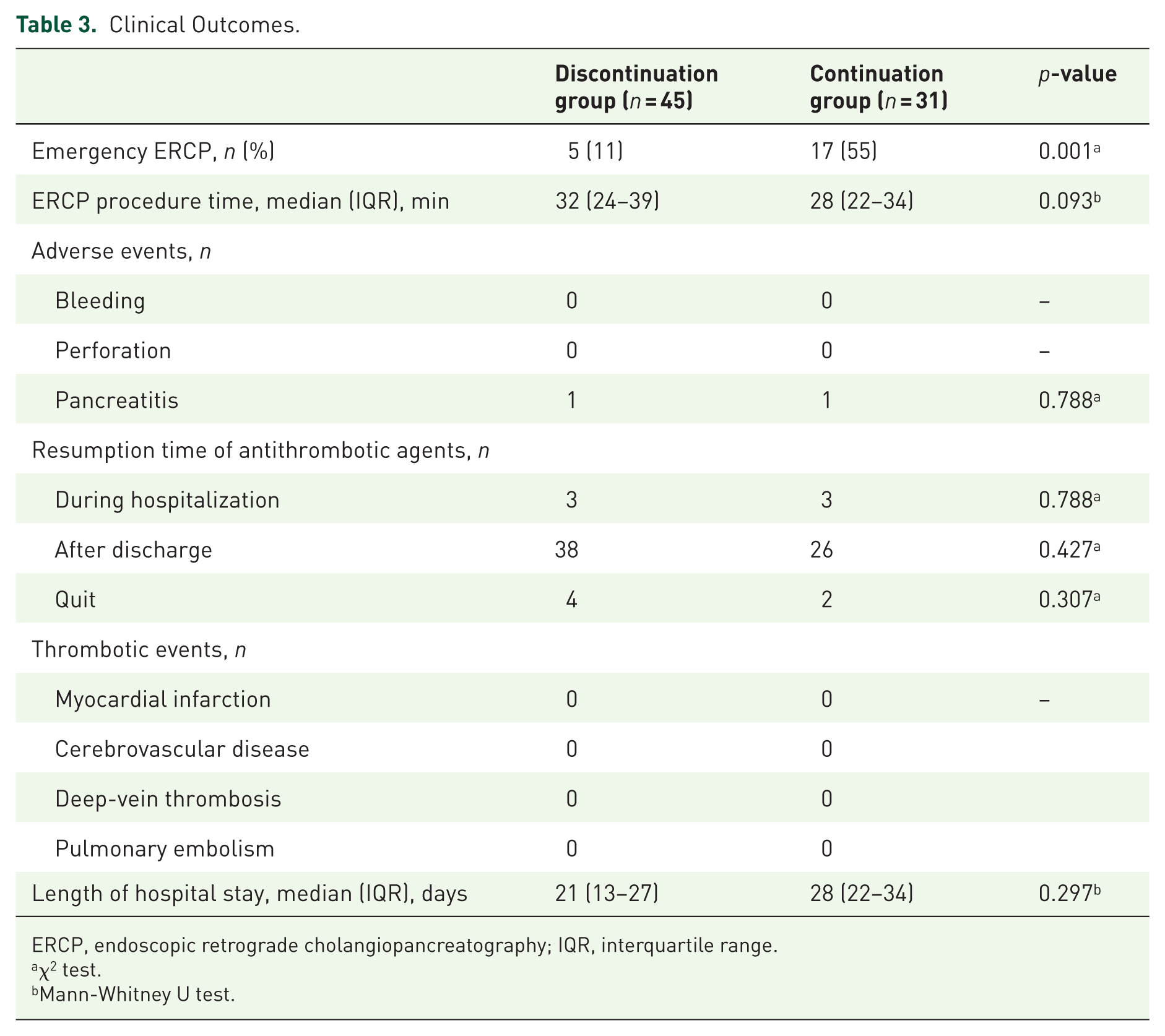
ERCP, endoscopic retrograde cholangiopancreatography; IQR, interquartile range.
χ2 test.
Mann-Whitney U test.
Adverse events
The incidence of adverse events was not significantly different between the two groups. Neither bleeding nor perforation occurred in either group. Post-ERCP pancreatitis occurred in 1 patient in both groups (Table 3).
Time to resumption of antithrombotic agents
The time to resumption of antithrombotic agents did not differ significantly between the two groups (Table 3).
Duration of hospital stay
There was no significant difference in hospital stay duration between the 2 groups, 21 (13–27) versus 28 (22–34) days for the discontinuation and continuation groups, respectively, p = 0.297, (Table 3).
Thrombotic events during the hospital stay
No incidence of thrombotic events or exacerbation of comorbidity was observed during hospital stay between the two groups (Table 3).
Discussion
This study suggests that EST in patients undergoing antithrombotic treatment can prevent adverse events if the guidelines for gastroenterological endoscopy in patients undergoing antithrombotic treatment are followed.
In recent years, the aging population has increased both in developed and developing countries. Antithrombotic therapy has been increasingly used to reduce the risk of thromboembolic events in patients with cerebrovascular disease and cardiovascular disease.
In Japan, the JGES GL was published in 2012, 1 and a supplemental version of the guidelines was published in 2017 because various DOACs had become available since then. Antithrombotic agents include antiplatelet agents such as aspirin and thienopyridine derivatives as well as anticoagulants such as warfarin, heparin, dabigatran and DOACs. Endoscopic examination and treatment procedures were classified into four categories: diagnostic gastroenterological endoscopy without biopsy, endoscopic mucosal biopsy, gastroenterological endoscopy with a low risk of bleeding, and gastroenterological endoscopy with a high risk of bleeding. EST is classified under gastroenterological endoscopy with a high risk of bleeding. JGES GL recommends that aspirin can be continued in patients with a high risk of bleeding if the risk of thromboembolism is high. A previous article reported that withdrawal of aspirin significantly increased the risk of cerebrovascular disease [odds ratio (OR): 3.4; 95% confidence interval (CI): 1.08–10.63, p < 0.005]. 4 Therefore, it is important to consider not only the bleeding risk associated with antithrombotic treatment but also the thromboembolism risk associated with discontinuing antithrombotic treatment.
In the current American Society of Gastrointestinal Endoscopy guidelines, EST is classified as a procedure to be performed in patients with a high risk of bleeding. 5 In the current European Society of Gastrointestinal Endoscopy guideline, EST is classified as a high-risk procedure. 6 Each GL recommends that aspirin is tolerable, whereas thienopyridines, warfarin and DOAC must be discontinued before EST.
Recently, several retrospective studies have been published on EST-related bleeding in patients taking antithrombotic agents. Hussain and colleagues 7 reported that antiplatelet agents do not affect bleeding associated with EST (OR: 0.41; 95% CI: 0.13–1.31). Hamada and colleagues reported that the continuation or discontinuation of the antiplatelet agent did not have a statistically significant effect on severe bleeding after EST [OR: 0.67 (95% CI: 0.21–2.11) and OR: 1.25 (95% CI: 0.90–1.74) in the continuation and discontinuation groups, respectively]. However, anticoagulant continuation significantly increased severe EST-related bleeding compared to anticoagulant discontinuation [1.6% vs 0.8% (OR: 1.70, 95% CI: 1.10–2.63) for the continuation and discontinuation groups, respectively; p = 0.016]. 8
Ikarashi and colleagues reported a large-scale study of bleeding after EST. The study included 27% of patients undergoing antithrombotic treatment. As a result, the incidence of delayed bleeding after EST was 2.7%. Hemodialysis, heparin replacement, and early hemorrhage were significant clinical factors of delayed bleeding after EST in the multivariable analysis. 9
Emergency ERCP is often needed for AC, based on the Tokyo Guidelines for the management of AC (TG13). 10 Biliary drainage must be performed immediately in patients with mild and moderate AC with antibiotic therapy failure. Patients with severe AC are most likely to require organ support, and biliary drainage should be conducted after hemodynamic stabilization has been achieved. 11 Our institution’s policy is that patients with moderate and severe AC undergo emergency EBD. Even for mild AC patients, emergency EBD is performed if there is high fever (>38°C) or severe abdominal pain. If patients have bleeding tendency or take more than two antithrombotic agents, endoscopic papillary balloon dilation (EPBD) is recommended as an alternative to EST. During this study, there were two cases who continued multiple antithrombotic agents and they performed EPBD for biliary drainage.
This study shows that the use of EST in patients undergoing antithrombotic treatment can prevent adverse events if the guidelines are followed. The percentage of patients who underwent emergency ERCP in the continuation group was significantly higher than that in the discontinuation group because the continuation group included many patients with AC or cholecystitis. However, the incidence of adverse events did not differ significantly between the two groups. In particular, there was no adverse bleeding event in either group.
Recently, some articles have reported on the bleeding risk associated with DOACs. Nagata and colleagues 12 reported that the incidence of postprocedural bleeding was higher in warfarin users than in DOAC users (12.0% vs 9.9%; p = 0.002). Thus, the conclusions regarding the bleeding risk associated with DOACs vary, and it is necessary to further evaluate these differing conclusions with additional multicenter randomized controlled trials.
The length of hospital stay did not differ significantly between the two groups because the continuation group often continued the treatment for AC or cholecystitis with antimicrobial agents after emergency ERCP.
During this study, there was one case of failed bile duct cannulation who continued 3 antithrombotic agents. In this case, percutaneous transhepatic gallbladder drainage was performed because of severe cholangitis and cholecystitis. Fortunately, no bleeding was observed in this case.
The limitations of this study are that it was based in a single center and had a retrospective design and a small number of patients. In this study, EST in patients who took aspirin monotherapy may be permitted if the guidelines consider the comorbidities. In some cases, EST could be performed for patients who took aspirin and warfarin in the therapeutic range without serious bleeding event. Based on this study, we should consider the safety of EST for patients who take multiple antithrombotic agents without withdrawal. Fortunately, bile duct cannulation succeeded except for one case in this study. However, bile duct cannulation may not be successful for all patients. This is one of the limitations of this study. It is necessary to confirm the safety of EST with additional multicenter randomized controlled trials in patients undergoing antithrombotic treatment.
Conclusion
EST in patients undergoing antithrombotic treatment may be safe if the guidelines are followed for gastroenterological endoscopy in patients undergoing antithrombotic treatment.
Footnotes
Contributors
Yamamiya A and Kitamura K designed the study; Kitamura K, Yamamiya A, and Ishi Y collected the data; Yamamiya A analyzed the data and drafted the manuscript; Kitamura K, Yamamiya A, Ishii Y, Mitsui Y, and Yoshida H contributed to the design and interpretation of the study.
Ethical approval
The study was approved by the Medical Ethics Committee of Showa University Hospital.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.