
Abstract
Treatment with Anti-Tumor Necrosis Factor (anti-TNF) therapy has become a mainstay of therapy for patients with CD who are unresponsive to conventional medical management. Currently there are three anti-TNFα antibodies that have been approved by the US Food and Drug Administration for the treatment of CD, namely infliximab, adalimumab and certolizumab pegol (CZP). Several double blind placebo controlled trials determined that CZP is effective as induction and maintenance treatment in adult patients with CD regardless of their prior exposure to other anti-TNFα antibodies. This review discusses the efficacy of CZP and adherence to therapy with anti-TNFα antibodies in patients with CD.
Introduction
Crohn's Disease (CD) is a chronic inflammatory disorder of the gastrointestinal tract characterized by focal, asymmetric, transmural inflammation of uncertain etiology and of an unpredictable course. The clinical presentation of CD is characteristically manifested by repeated cycles of active and quiescent disease of definable patterns according to disease location and types (inflammatory, fibrostenotic and fistulizing).1,2 The prevalence and incidence of CD in the United States is estimated to be 50 per 100,000 and 5 per 100,000 annually, respectively. 3 The treatment regimen is individualized based on disease activity, location and behavior taking into the account the balance between medications and their side effects and prevention of complications. The treatment of CD remains empirical and the disease is not curable since no clear etiology of CD disease has been yet elucidated.
Our current ability to predict the course of CD is also not well established. Munkholm et al in their population-based cohort study from Scandinavia 4 demonstrated that among all patients treated with 5-aminosalicylic acid (5-ASA) agents and corticosteroids (CS), 13% of patients will achieve complete remission, 20% of patients will experience annual relapse and 67% will have a combination of relapse and remission within the first 8 years after initial diagnosis. Less than 5% of patients will have a continuous course of active disease. Another population-based cohort based in Olmsted County, Minnesota, which was conducted prior to the routine use of anti-Tumor Necrosis Factor α (anti-TNFα) agents, confirmed that a representative patient with CD would be expected to spend 24% of the time in medical remission without medications, 41% of the time in post-surgical remission without medications, 27% of the time in medical treatment with 5-ASA derivatives and 7% of the time having disease activity requiring treatment with corticosteroids or immunomodulators. 5
Although CD has been recognized as having a chronic relapsing course, it is evident that the majority of patients remain in clinical remission at any particular time. However it is recognized that the majority of patients will progress from inflammatory to complicated fistulizing or penetrating disease over time. The cumulative risk for the development of a CD-related fistula has been estimated to be 33% at 10 years and 50% after 20 years based on a population based cohort study form Olmsted County, MN. 6 Therefore the treatment strategies for CD must target lifelong management, addressing both short-term and long-term aspects of the disease and are guided by the disease location, severity, associated complications and concurrent therapy taken by the patients. These treatment strategies consist of a sequential (“step up”) approaches ranging from the first line agents such as 5-ASA, controlled released corticosteroids (budesonide) and antibiotics all used to treat mild to moderate active CD to the second line with oral prednisone and the third line with conservative use of immunomodulators (azathioprine (AZA), 6-mercaptopurine and methotrexate) and further biological therapy (infliximab, adalimumab, CZP and natalizumab). Recently, 5-ASA has been critically analyzed for treatment of patients with CD and is suggested to be no more effective than placebo. 7 However, recent data suggest that early initiation of combined treatment with immunomodulators and anti-TNFα agents (infliximab) (“top down”) was more efficacious than conventional management with CS followed by AZA and then infliximab 8 in prior anti-TNFα and anti-metabolite naïve patients. The ultimate goal of therapy is to induce and maintain clinical remission.
Therapy with anti-TNF a antibodies has become a mainstay of treatment for patients with CD who are unresponsive to conventional medical management. Currently there are three anti-TNFα agents that have been approved by the U.S. Food and Drug Administration (FDA) in the treatment of CD, namely infliximab, adalimumab and CZP. Infliximab (Remicade) is administered intravenously whereas adalimumab (Humira) and CZP (CZP) (Cimzia) are administered subcutaneously. Treatment with infliximab consists of an initial loading regimen with three initial infusions at the dose of 5 mg/kg at week 0, 2 and 6 followed by every 8 week maintenance schedule. 9 Treatment with adalimumab (administered subcutaneously) consists of initial loading dose of 160 mg (given either in four doses of 40 mg each within 1 day or in two daily doses of 40 mg each over two consecutive days) followed by 80 mg dose given two weeks later with initiation of maintenance treatment after additional 2 weeks at dose 40 mg every 2 weeks. 10 Treatment with CZP is initiated with an initial loading dose of subcutaneous injection of 400 mg at weeks 0, 2 and 4 followed by maintenance treatment every 4 weeks. 11 CZP was approved in April 2008 by the US Food and Drug Administration and is currently approved for reducing signs and symptoms of CD and for maintaining clinical response in adult patients with moderate to severe activity of the disease with inadequate response to conventional therapy. 12
Anti-TNFα therapy (infliximab, adalimumab and CZP) was found to be significantly more efficacious than placebo in inducing remission at week 4 with a total mean difference in effect between anti-TNFα agents and placebo of 11% (95% CI 6%-16%, P < 0.001) based on the results of a meta-analysis of fourteen randomized placebo controlled trials that included a total of 3995 patients with CD. 13 These biologic medications were also significantly superior over placebo in maintaining remission at weeks 20 through 30 with total mean difference in effect between active and placebo arms of 23% (95% CI 18%-28%, P < 0.001) among patients who responded to an open-label induction with either infliximab, adalimumab or CZP followed by randomized placebo controlled maintenance treatment. 13
This review discusses the efficacy of CZP and adherence to anti-TNFα therapy with a particular focus on CZP in patients with CD.
Clinical Trials
The efficacy of CZP was evaluated in two dose-response Phase II (n = 384)14,15 and two Phase III (The Pegylated Antibody Fragment Evaluation in CD Disease: Safety and Efficacy 1 (PRECiSE 1) and PRECiSE 2)16,17 (n = 1330) randomized placebo controlled trials in adult patients with moderate to severe CD (Table 1).
The first Phase II trial (n = 92) assessed efficacy of CZP over 12 weeks period after single 30-minute intravenous infusion of either CZP (CDP870) (1.25 mg/kg, 5 mg/kg, 10 mg/kg or 20 mg/kg) versus placebo. 14 The primary endpoint was clinical response (decrease in Crohn's Disease Activity Index (CDAI) score at least by 100 points when compared to baseline) at week 4. 14 CZP demonstrated similar efficacy to placebo in achieving primary endpoint (60% for 5 mg/kg, 58.8% for 10 mg/kg, 47.8% for 20 mg/kg vs. 56% for placebo). 14 Similarly, no difference between any dose of CZP and placebo was observed with respect to secondary endpoints (clinical response, remission, CDAI score decrease by ≥70 points, C-reactive protein (CRP) levels at weeks 2, 8, 12). 14 On the other hand, CZP given at 10 mg/kg was significantly more efficacious than placebo in inducing remission at week 2 (47.1% vs. 16%, P = 0.041). 14
The second Phase II 12-week trial (n = 292) evaluated efficacy of CZP administered subcutaneously (100 mg, 200 mg or 400 mg) or placebo. 15 Treatment with CZP was not superior over placebo as assessed at the primary study endpoint (clinical response at week 12) with the response rates among active drug arm of 36.5% (100 mg), 36.1% (200 mg) and 44.4% (400 mg) and in the placebo arm of 35.6%. 15 However, CZP was superior to placebo in achieving clinical response at week 2 (100 mg, 200 mg and 400 mg), 4 (200 mg and 400 mg), 8 (100 mg and 400 mg)and 10 (400 mg) with the highest rates for 400 mg dose at any analyzed. 15 In addition, CZP was superior to placebo in inducing clinical remission at week 4 (100 mg, 200 mg and 400 mg) and week 8 (100 mg and 400 mg) but not week 12. 15 Treatment with the highest dose of CZP (400 mg) was superior to placebo in achieving primary (53.1% vs. 17.9%, P = 0.005) and secondary endpoints in patients with high baseline levels of CRP (≥10 mg/L) but not in those with low baseline CRP levels in post-hoc analysis. 15 Based on these findings it was proposed that the efficacy of CZP over placebo might not have been demonstrated due to the high placebo response rate in the large cohort of patients with low baseline level of CRP. 15
The latter findings were taken into consideration in the Phase III 26-week PRECiSE 1 trial (Table 1). 16 Patients in this trial (n = 660) were stratified based on low (<10 mg/L) or high (≥10 mg/L) baseline CRP levels and then randomized to subcutaneous injections of either CZP 400 mg or placebo given every 2 weeks through week 4 and then every 4 weeks through week 26. 16 CZP was found to be significantly more efficacious in achieving the primary endpoint (at least 100 point decrease in CDAI score at week 6 and both weeks 6 and 26 in a cohort of 302 patients with high baseline CRP levels) with rates of 37% vs. 26% (wk 6, P = 0.04) and 22% vs. 12% (both wk 6 and 26, P = 0.05). 16
Randomized double blind placebo controlled trials of CZP in induction and maintenance of remission in patients with moderate to severe Crohn's disease.

In an overall cohort treatment CZP was superior to placebo in achieving clinical response at week 6 (35% vs. 27%, P = 0.02) and both weeks 6 and 26 (23% vs. 16%, P = 0.02). 16 On the other hand, no significant difference was found between the active arm and placebo arm with respect to achieving remission at any time point among all patients (wk 6: 22% vs. 17%, P = 0.17; both wk 6 and 26: 14% vs. 10%, P = 0.07) or patients with high baseline CRP level (wk 6: 22% vs. 17%, P = 0.29; both wk 6 and 26: 13% vs. 8%, P = 0.24). 16 Concomitant use of immunosuppressants or CS, previous infliximab therapy or smoking status did not influence the response rates at the aforementioned time points. 16 The presence of antibodies to CZP were detected in 8% of CZP-treated patients with a 4% rate in CZP-treated patients who also received immunosuppressive agents and with 10% rate in CZP-treated patients who did not receive concomitant immunosuppressive agents. 16
The subsequent PRECiSE 2 trial (Table 1) observed that CZP was superior to placebo in maintaining response and clinical remission in responders to induction therapy with CZP. 17 Among patients who received an open-label induction therapy with 3 single doses of 400 mg CZP given subcutaneously every 2 weeks 64% (428/668) responded (at least 100 point decrease in CDAI score vs. baseline score). 17 These patients were stratified according to baseline CRP levels (≥10 vs. <10 mg/L) and randomized to receive subcutaneously either CZP 400 mg or placebo administered every 4 weeks through week 24 with follow-up through week 26. 17 Therapy with CZP was superior to placebo in maintaining response to treatment through week 26 in patients with baseline high C-reactive protein levels (primary end point) (n = 213, 62% vs. 34%, P < 0.001) and in the intention to treat population (n = 425, 63% vs. 36%, P < 0.001). 17 CZP was also significantly superior to placebo in achieving clinical remission at week 26 in the cohort with high baseline CRP (42% vs. 26%, P = 0.01) and in all patients in the intention to treat population (48% vs. 29%, P < 0.001). 17 Antibodies to CZP were detected in 18% of patients receiving placebo maintenance therapy and in 8% of patients receiving continuous CZP treatment (P-value not reported). 17 Among those who received concomitant immunosuppressive agents the rates of detectable antibodies to CZP were 2% in CZP maintenance arm and 8% in placebo maintenance arm. 17 On the other hand, the rates of patients with detectable antibodies to CZP in those not treated with immunosuppressants were 12% in CZP arm and 24% in placebo arm. 17 A recent detailed analysis of a cohort of 108 patients with fistulizing CD that participated in the PRECiSE 2 trial 17 showed that 58 (53.7%) of them achieved clinical response to induction therapy with CZP at week 6 and were subsequently randomized to receive further maintenance with either CZP (n = 28) or placebo (n = 30). 18 The complete fistula healing rate was achieved at week 26 in 36% of CZP-treated and in 17% of placebo-treated patients (P = 0.038). 18 However, using the PRECiSE 2 trial 17 pre-specified definition of fistula closure (closure of ≥50% of fistulas at any two consecutive post-baseline visits at least 3 weeks apart) there was no difference between CZP and placebo arms with respect to percentage of patients achieving fistula closure (54% vs. 43%, P = 0.069). 18
An additional analysis of randomized maintenance trial data from PRECISE 2 highlighted that CZP-treated patients with shorter duration of CD (less than 1 year) had higher response rates at week 26 when compared to those CZP-treated subjects with longer duration of CD (≥5 years) (89.5% vs. 57.3%, P < 0.05). 19 However, CZP-treated patients with both short (<1 year) and long (≥5 years) duration of CD had significantly higher response (89.5% vs. 37.1%, P < 0.01 and 57.3% vs. 32.7%, P < 0.001, respectively) and remission (68.4% vs. 37.1%, P < 0.05 and 44.3% vs. 23.5%, P < 0.001, respectively) rates than placebo recipients at week 26. 19 The factors that independently predicted maintenance of response to CZP at week 26 identified by logistic regression were shorter (<2 years) vs. longer duration of CD (82.1% vs. 58.5% P < 0.006), absence vs. presence of prior intestinal resection (67.5 vs. 51.6%, P < 0.027), infliximab-naïve status vs. prior exposure to infliximab (68.7% vs. 44.2%, P < 0.002), and no corticosteroid use vs. corticosteroid use at baseline (65.7% vs. 57.3%, P < 0.001). 19 Although the PRECiSE 2 trial demonstrated that the efficacy of CZP is higher in patients receiving this agent as the first-line biologic when compared to infliximab-exposed individuals a post-hoc analysis of PRECiSE 2 data showed that patients with CD may benefit from treatment with CZP regardless of prior use of infliximab when compared to those treated with placebo. 20 CZP was significantly more effective than placebo as maintenance therapy at week 26 in both infliximab-exposed (response: 44.2% vs. 25.5%, P = 0.018; remission: 32.7% vs. 13.7%, P = 0.008) and in infliximab naïve patients (response: 68.7% vs. 39.6%, P < 0.0001; remission: 52.8% vs. 33.3%, P < 0.001). It should be noted however that the superiority of CZP over placebo was more distinct in infliximab naïve patients. 20 These interesting observations however require future validation in a large prospective placebo controlled trials.
All patients who completed 26-week PRECISE 2 trial were offered open label extension treatment with CZP given at 400 mg s.c. dose every 4 weeks for 54 weeks (PRECiSE 3 trial). 21 The PRECiSE 3 trial included 141 patients who received CZP (PRECiSE continuous group) and 100 patients who received placebo (PRECISE 3 drug interruption group) in prior PRECiSE 2 trial. 21 Among patients who were either in response or remission at PRECiSE 3 baseline (week 26 of PRECISE 2) the rates of sustained response (reduction in Harvey-Bradshaw Index score ≥3 from baseline for all visits) and remission (HBI score ≤4 for all visits) were similar between continuous and drug interruption arms at 26 weeks (sustained response: 74.4% vs. 79.7%, respectively; sustained remission: 72.8% vs. 73.5%, respectively) and 54 weeks (sustained response: 66.1% vs. 63.3%, respectively; sustained remission: 62.1% vs. 63.2%, respectively) of PRECiSE 3 trial. 21 On the other hand, patients in the drug interruption arm had a greater incidence of adverse events related to CZP than those receiving CZP continuously (32% vs. 23.4%, P-value not reported). 21 Therefore it has been suggested that continuous administration of CZP should be recommended due to its effectiveness and more favorable safety profile. 21
All patients who relapsed (increase in CDAI ≥ 70 points above baseline or higher than baseline at week 6 of PRECiSE 2 trial with an absolute CDAI score ≥ 350 points) and decided to withdraw before week 26 of PRECiSE 2 trial were offered an open-label extension study (PRECISE 4). 22 Patients (n = 124) enrolled in the PRECiSE 4 study were separated into either the continuous (n = 49) or drug interruption (n = 75) arm based on whether they received CZP or placebo maintenance following CZP induction during the PRECiSE 2 trial. 22 Patients who relapsed on CZP maintenance therapy received a single dose of CZP 400 mg s.c. whereas those who relapsed after CZP interruption received three reinduction doses of CZP 400 mg s.c. 2 weeks apart with subsequent maintenance administration every 4 weeks up to week 52. 22 CZP was equally efficacious in continuous and drug interruption treatment arms with 63.3% and 65.3% response (reduction in Harvey-Bradshaw Index score ≥3 from baseline) rates at week 4, respectively and 54.8% and 59.2% further maintaining this response at week 52, respectively. 22 The remission rates (HBI score ≤4) at week 4 were 28.6% and 44% among those treated with CZP continuously and with prior intermission, respectively with sustained respective remission rates at week 52 of 64.3% and 54.5%. 22 Patients with CD experiencing disease relapse on CZP maintenance therapy following initial response to induction with CZP may benefit from administration of an additional dose of CZP. Similarly, those with recurrence of CD after CZP discontinuation may achieve improvement in their symptoms after reinduction of CZP. 22
A phase IIIb WELCOME trial (26-Week open-label-induction, double-blind-maintenance, placebo-controlled trial Evaluating the clinical benefit and tolerability of CZP induCtiOn and Maintenance in patients suffering from CD with prior loss of response or intolErance to infliximab) assessed the efficacy of CZP in treatment of patients with active CD and prior loss of response or hypersensitivity to infliximab. 23 An open-label induction with CZP administered s.c. at the dose 400 mg at weeks 0, 2 and 4 in 539 patients resulted in 62% response (decrease in CDAI ≥ 100 points from baseline) and 39.3% remission (CDAI ≤ 150 points) rates at week 6. 23
There were 329 patients who responded to CZP induction at week 6 who entered a double-blind maintenance part of the WELCOME trial that compared the efficacy of CZP 400 mg maintenance treatment administered either every 2 weeks (n = 161) or every 4 weeks (n = 168) from week 6 through week 26. 23 Both maintenance regimens displayed comparable rates of sustained response (36.6% vs. 39.9%, respectively P = 0.55) and remission (30.4% vs. 29.2%, respectively, P = 0.81) at the end of the trial (week 26). 23
A recent randomized double blind placebo controlled 6-week trial (Table 1) evaluated the efficacy of CZP in 439 adult patients with active CD and no prior exposure to anti-TNF therapy. 24 Patients were randomly assigned to either a single s.c. dose of CZP 400 mg or placebo given at 0,2 and 4 weeks with subsequent assessment of clinical remission (CDAI ≤ 150 points) at week 6. 24 Overall, there was no statistical difference in remission rates at week 6 between CZP and placebo groups (32% vs. 25%, P = 0.174). 24 However, among patients with baseline CRP ≥ 5 mg/L treatment with CZP resulted in a statistically significant difference in remission rates at week 6 when compared to placebo (P = 0.031). 24 Certain demographic and baseline disease characteristics such as age ≤40 years, male sex, CRP ≥ 10 mg/L, disease located in colon or in ileum and colon, no prior surgical resection, disease duration less than baseline mean, increased clinical disease activity (CDAI ≥ 300 points) were associated with a statistically significant 2-3 fold higher rates of clinical remission with CZP versus placebo. 24
Recent data from a Swiss, prospective, questionnaire-based phase IV study of 60 clinical practice based-patients who received induction and maintenance treatment with CZP 400 mg demonstrated 70% and 67% response (decrease of HBI score ≥3 points vs. baseline) rates and 40% and 36% remission (HBI ≤ 4 points) rates at week 6 and week 26, respectively. 25 In addition, 36% and 55% of patients had complete fistula closure at week 6 and 26, respectively. 25 Among treated patients 88% and 67% continued CZP beyond week 6 and week 26, respectively. 25
Adherence to Anti-TNF Agents in CD
Adherence has been defined as the degree to which the patient follows medication intake and other doctor's recommendations.26,27 The term adherence is currently preferred over the term compliance since it underlines the equal role of both patient and the doctor in their relationship whereas the term compliance underlines only the greater power of the doctor.26,27 According to the World Health Organization patient's adherence to treatment determines the success of given therapy. 28 On the other hand, the adherence to treatment in patients with chronic disorders in developed countries has been estimated to be at 50%. 28 Levy and Feld grouped patients' reasons of patients' non-adherence to gastroenterology medical management into either lack of adequate skills or knowledge to comply with prescribed treatment (inadequate or poor information about prescribed medications), lack of patients' belief that prescribed treatment is helping them or the lack of support from the patients' environment (financial or employment situation, situation at household not allowing to comply with treatment, difficulties with transportation) (Table 2). 27 In order to increase patients' adherence physicians should understand that their recommendations for patients have to include clear explanations of rationale for treatment, why adherence to prescribed regimen is crucial to therapeutic success, review of therapeutic assignments given during past visits (homework) including discussion of any difficulties patients may have encountered, attempt to address them and praise success (Table 3). 27 Levy and Feld suggested 10 recommendations addressing the reasons for nonadherence (Table 4). They underline the crucial role of the proper physician-patient contact in establishing the pattern of patient's adherence. Although Levy and Feld published their recommendations in 1999 when anti-TNFα agents were emerging for treatment of CD their recommendations may be also applied to medications administered intravenously or subcutaneously in order to increase patient's adherence. For example, quality of the physician/patient relationship and patient's trust in physician's recommendations certainly would lead to increased adherence to any medication that is warranted.
Reasons patients give for nonadherence.

Structuring the treatment session.

Adherence recommendations.

Reprinted by permission from Macmillan Publishers Ltd: [American Journal of Gastroenterology] (Levy RL, Feld AD. Increasing patient adherence to gastroenterology treatment and prevention regimens. Am J Gastroenterol. 1999;94:1733-42), copyright (1999). 27
The major goal of treatment of CD is to induce and maintain disease in remission. It has been demonstrated that remission in patients with CD is associated with reduced hospitalizations and surgeries, increased employment and improved quality of life. 29 This is why it is important to determine factors associated with adherence and factors associated with nonadherence to anti-TNFα agents in order to improve adherence if patient does not adhere or to maintain adherence if patient adheres to prescribed regimen.
Until now and at the time of writing this manuscript, there have been no published studies on the adherence to CZP in patients with CD. Therefore the adherence to therapy with CZP is unknown in patients with CD. However, there are some data available on adherence to other anti-TNFα agents in CD, namely infliximab and adalimumab. There have been only two studies that evaluated the adherence of infliximab30,31 and one study that assessed adherence to adalimumab 32 in patients with CD.
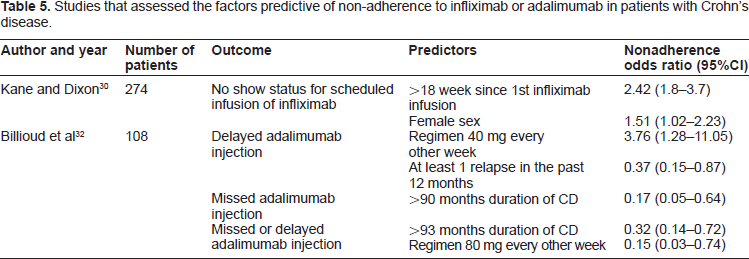
Two studies assessed factors predictive of nonadherence for infliximab 30 and adalimumab using multivariable models 32 (Table 5). In their first study Kane et al collected data from outpatient databases that included 274 patients with CD who were scheduled to receive 1185 infusions with infliximab within 17 month period. 32 The Authors defined non-adherence as patient no-show without prior rescheduling of appointment by the patient. 30 The observed non-adherence rate was 4% (48/1185) and a female sex and time from the initial infliximab infusion greater than 18 weeks were found to increase risk of non-adherence 2-fold. 30
Studies that assessed the factors predictive of non-adherence to infliximab or adalimumab in patients with Crohn's disease.
In an attempt to assess the impact of the adherence to infliximab on health care costs in patients with CD an analysis of the Integrated Health Care Information Service National Managed Care Benchmark Database including medical histories of over than 25 million patients enrolled in managed care within the US was performed and identified 571 patients with CD who were receiving infliximab maintenance treatment over the 4 year time period (at least four consecutive infusions) within the first year after the initial infusion. 31 Non-adherence was defined as less than 7 infusions during the first year of treatment. 31 Its rate was found to be 34.3% and it was associated with nearly 3-fold increase in an all-cause hospitalizations (OR = 2.7; P < 0.001) and 2.5-fold increase in CD-related hospitalizations (OR = 2.5, P < 0.001). 31 In addition, non-adherence to infliximab was also associated with increased by 73% adjusted total medical costs excluding infliximab cost (P < 0.001), by 115% adjusted all-cause hospitalization cost (P < 0.001) and by 29% adjusted all-cause outpatient cost excluding infliximab cost (P < 0.001) when compared to adherence to infliximab. 31 Similarly, non-adherence to infliximab was associated with increased by 90% adjusted CD-related medical cost excluding infliximab cost, by 115% adjusted CD-related hospitalization cost and by 43% adjusted outpatient cost excluding infliximab cost when compared to adherence to infliximab (P < 0.001). 31
A group of French researchers performed a 21 month prospective observational multicenter study of adherence to adalimumab in patients with CD. 32 Non-adherence was defined as either delay or miss of at least one injection of adalimumab within 3 months prior to the study. 32 Among 108 patients with CD 49 (45.4%) of them were non-adherent to adalimumab injection with 16 patients (14.8%) missing at least one of injection and 33 patients (30.6%) delaying at least one injection. 32 The reasons for non-adherence were forgetfulness (24.6%), infection (24.6%), travel (20%), intentional non-adherence (10.8%), pharmaceuticals supply problems (9.2%), side effects (7.7%), pregnancy (1.5%) and hospitalization due to CD (1.5%). 32 Overall, duration of disease greater than 93 months and adalimumab injection 80 mg every other week were negatively associated with injection delay or miss. 32 The injection regimen of adalimumab at the dose of 40 mg every other week was associated with nearly 4-fold increase in injection delays whereas the presence of at least one relapse within last 12 months was a negative predictor of a delayed injection. 32 Duration of CD greater than 90 months was negatively associated with missed injection. 32
Conclusions
Current evidence strongly suggests that CZP is an effective therapy for patients presenting with moderate to severe CD in anti-TNFα naïve patients as well as in patients with secondary loss of response or intolerance to infliximab. CZP has expanded the spectrum of anti-TNFα agents available for the treatment of patients with CD. Patients with increased serum markers of inflammation (CRP) belong to the subset of patients in whom CZP is of particular benefit. Studies have demonstrated CZP to be an effective for induction and maintenance therapy in patients with CD and improving health-related quality of life for these patients.33,34 Future studies on large number of patients are warranted to evaluate the efficacy of CZP in the setting of clinical practice.
There have been no published studies that assessed adherence to CZP in patients with CD. There are limited data on adherence to other anti-TNFα therapies, infliximab and adalimumab. Future studies are needed to determine factors associated with patient adherence to CZP. Treatment with CZP is associated with improvement in quality of life and lessened work impairment in patients with CD. At this moment, health care professionals should be encouraged to follow ten adherence recommendations presented in Table 4 to attempt to increase patient adherence to medications and regimens. Patients should be encouraged to adhere to treatment with CZP not only due to its efficacy in maintaining clinical remission in CD but also because of improvement in quality of life and reduction of work impairment. Future studies should determine what factors are associated with non-adherence to CZP and also other anti-TNFα agents. This would allow us to make evidence-based steps necessary to increase patients' compliance.
Potential Conflict of Interest Declaration
Wojciech Blonski: No conflict of interest to declare. Anna M. Buchner: No conflict of interest to declare. Gary R. Lichtenstein: Abbott Corporation, Consultant; Alaven, Consultant, Research; Bristol-Myers Squibb, Research; Centocor Orthobiotech, Consultant; Research; Elan, Consultant; Ferring, Consultant, Research; Meda Pharmaceuticals, Consultant; Millenium Pharmaceuticals, Consultant; Pfizer Pharmaceuticals, Consultant; Proctor and Gamble, Consultant, Research; Prometheus Laboratories, Inc., Consultant, Research; Salix Pharmaceuticals, Consultant, Research; Santarus, Consultant; Schering-Plough Corporation, Consultant; Shire Pharmaceuticals, Consultant, Research; UCB, Consultant, Research; Warner Chilcotte, Consultant, Research; Wyeth, Consultant.
Author Contributions
Analysed the data: WB, AB, GRL. Wrote the first draft of the manuscript: WB. Contributed to the writing of the manuscript: WB, AB, GRL. Agree with manuscript results and conclusions: WB, AB, GRL. Jointly developed the structure and arguments for the paper: WB, AB, GRL. Made critical revisions and approved final version: GRL. All authors reviewed and approved of the final manuscript. WB, AB, GRL.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.
Supplementary Data
A video abstract by the authors of this paper is available. video-abstract7613.mov
Publish with Libertas Academica and every scientist working in your field can read your article
“I would like to say that this is the most author-friendly editing process I have experienced in over 150 publications. Thank you most sincerely.”
“The communication between your staff and me has been terrific. Whenever progress is made with the manuscript, I receive notice. Quite honestly, I've never had such complete communication with a journal.”
“LA is different, and hopefully represents a kind of scientific publication machinery that removes the hurdles from free flow of scientific thought.”
Available to your entire community free of charge
Fairly and quickly peer reviewed
Yours! You retain copyright