
Abstract
After the problems associated with the non-selective 5-HT4 receptor agonists cisapride and tegaserod, the 5-HT4 receptor is now beginning to come in from the cold. Thus, prucalopride is now the first of a new class of drug defined by selectivity and high intrinsic activity at the 5-HT4 receptor. Prucalopride has been developed for treatment of chronic constipation rather than constipation-predominant irritable bowel syndrome (IBS). This follows the trend of first evaluating new gastrointestinal (GI) prokinetic drugs in disorders where disrupted GI motility is known to exist, rather than in a functional bowel disorder where changes in motility are uncertain. If prucalopride is not progressed towards the IBS indication, it has at least shown the way for other selective 5-HT4 receptor agonists. Most notable among these is TD-5108 (velusetrag), also characterized by good selectivity at the 5-HT4 receptor, high intrinsic activity and efficacy in patients with chronic constipation.
Keywords
Introduction
5-HT4 receptor agonists have been available since the introduction of metoclopramide in 1964. This drug, which is also an antagonist at dopamine D2 receptors and at 5-HT3 receptors, is still widely used around the world. Its success led to the development of alternative molecules which were not D2 receptor antagonists (thereby removing the adverse events of akathisia and extrapyramidal movement disorders) and prucalopride is the latest of these developments.
1
However, unlike its predecessors, prucalopride differs in two vitally important ways:
Prucalopride is selective for the 5-HT4 receptor. In other words, it is the first of its class to have been profiled against the large range of 5-HT receptors which are now known to exist. Many of these receptors (including the 5-HT4 receptor itself) were not known when metoclopramide was introduced or when the second generation of 5-HT4 receptor agonists was being developed. Some of the latter have since been found to interact with other 5-HT receptors, likely to oppose the prokinetic benefits of 5-HT4 receptor agonism. As an agonist, prucalopride also seems to have a high intrinsic activity at the 5-HT4 receptor. Surprisingly, some of the earlier compounds have a low intrinsic activity at this receptor, contributing to poor clinical efficacy.
It is, therefore, extraordinary that it has been 36 years since the introduction of metoclopramide and 14 years since the identification of the 5-HT4 receptor, before the first selective 5-HT4 receptor agonist has been developed for clinical use. The difficult journey is not however, complete. Thus, although prucalopride may be the first oral compound to be approved for the treatment of severe chronic constipation (“for the symptomatic treatment of chronic constipation in women in whom laxatives fail to provide adequate relief”) in all 27 member states of the European Union (EU), it is not available in the rest of the world.
Here we review the pharmacology of prucalopride and compare the profile of this molecule with both its predecessors and its competitors. We also look at the clinical need for a drug which stimulates intestinal motility, before describing the clinical trials which led to the successful registration of prucalopride within the EU. Finally, we look ahead, to try and judge the future of this molecule.
Mechanisms of Action of prucalopride and other 5-HT4 Receptor Agonists
Actions mediated by 5-HT4 receptors
Prucalopride increases gastrointestinal (GI) motility because it activates 5-HT4 receptors. In the intestine, functionally-active 5-HT4 receptors are located on the motor and sensory nerves of the enteric nervous system (ENS), on the smooth muscle of the intestine and on the epithelial cells lining the mucosa and on the enterochromaffin cells (Fig. 1). However, there are some species differences in the pattern of this distribution so, wherever possible, the following discussion focuses on studies using human isolated intestine.
Distribution of 5-HT4 receptors in the intestine. Functionally-active receptors have been identified on enterochromaffin cells (1), epithelial cells lining the mucosa (2), on the circular smooth muscle (3) and within the enteric nervous system on intrinsic primary afferent neurons (IPANs) (4) and the excitatory and inhibitory motor nerves projecting to the circular and longitudinal muscle (5) (see text for references). The diagram does however, represent a ‘generic’ view of this distribution and there are small differences between different species and between the small and large bowel.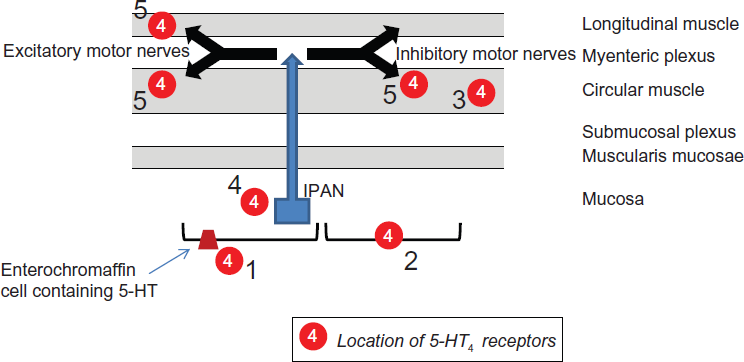
Perhaps the best studied are the functions of the 5-HT4 receptors expressed within the ENS. Here, 5-HT4 receptor activation facilitates motor neurotransmission in a relatively long-lasting manner. This has been demonstrated using the circular muscle of the human colon, where 5-HT4 receptor activation facilitates both cholinergic 2 5 and nitrergic3,4 motor nerve function, thereby promoting both the ascending excitatory and the descending inhibitory nerve components of the peristaltic reflex. A similar action has also been shown for the cholinergic neurons innervating the longitudinal muscle of the human colon. 6 Studies with human isolated small intestine have not yet been carried out although animal studies suggest a similar ability to facilitate cholinergic transmission. 7 Studies with mice, rats and guinea-pigs also indicate that 5-HT4 receptor activation will stimulate the intrinsic primary afferent neurons (IPANs) of the ENS; 8 to date, the role of the 5-HT4 receptor in modulating human IPAN function is unknown. The distribution of 5-HT4 receptors within the ENS of the intestine is, therefore, ideally placed to enable 5-HT to promote peristalsis and hence, intestinal propulsion. This property may be further facilitated by a direct ability of 5-HT4 receptor agonists to relax the circular muscle of the human colon, a function reported by some investigators 9 12 but not observed by others.3,4 In the human rectum, 5-HT4 receptor binding sites were distributed to the muscle and not the myenteric plexus. 13 Perhaps muscle relaxation in the lowest part of large bowel facilitates the ability of 5-HT4 receptor agonists to promote defecation.
The 5-HT4 receptor is also expressed on epithelial cells lining the mucosa and when activated, stimulates secretion of chloride ions (Cl–) into the lumen and reduces NaCl absorption. The change in electric potential attracts sodium into the lumen across tight junctions between the cells, creating an osmotic gradient for water to be drawn into the lumen. 14 This activity has been demonstrated in human small intestinal mucosa, in which movement of Cl– is measured as a change in polarity (Ussing chamber technology), but has not been observed in the human sigmoid colon. 15 17 Thus, whilst increased water within the small intestine is likely to promote the peristaltic reflex by mechanical stimulation, further stimulating movement of contents into the colon, this influence will be lost within the colon, given the huge ability of this organ to absorb water. Nevertheless, 5-HT released from the mucosa of human colon is reported to stimulate secretory function by activating sensory nerves sensitive to inhibition by capsaicin or hexamethonium. 18 For the reason given above, the effects of this action on the movement of colonic contents and/or on any side-effects of diarrhoea are unknown. In rodents, 5-HT4 receptors are not expressed by secretomotor neurons. 8
Finally, 5-HT4 receptors may act as autoreceptors on human enterocromaffin cells from the small intestine, which when activated, inhibit the release of 5-HT. 19 The significance of this action in the mechanisms by which 5-HT4 receptor agonists promote intestinal motility is not clear.
5-HT4 receptor splice variants
At least 8 different splice variants of the human 5-HT4 receptor (a G protein-coupled receptor positively coupled to cAMP) are created by alternative mRNA splicing at the intracellular, C-terminal end of the protein. 20 These variations present a theoretical mechanism whereby the receptor can couple to different downstream effector mechanisms in different cell-types. 21 However, it is difficult to prove this idea as it implies that tissue-dependent efficacy for 5-HT4 receptor agonists is dependent on tissue-dependent variations in distributions of splice variants and/or on their coupling to downstream signalling mechanisms; experiments involving recombinant receptor expression in secondary host cells must therefore be treated with caution until proven to translate to native tissues. Evidence to date suggests that most tissues with 5-HT4 receptors express the 5-HT4(b) and 5-HT4(a) isoforms, but only the human intestine has so far been found to express low levels of the 5-HT4(d) isoform; 22 in recombinant systems, the 5-HT4 receptor agonist, 5-HT3 receptor antagonist and GI prokinetic agent renzapride behaved as a full agonist at the 5-HT4(d) isoform but as a partial agonist at the 5-HT4(g) isoform. 23
Prucalopride as a 5-HT4 receptor agonist
Prucalopride shows high affinity for the human 5-HT4(a) and 5-HT4(b) receptor isoforms (Ki values in radioligand binding assays were 2.5 and 8 nM respectively) and high selectivity for the 5-HT4 receptor, compared with 40 non-5-HT receptors, ion channels, transporters and other sites (Ki values >2000 nM or more usually >10000) and compared with all other human 5-HT receptors (Ki >10000), including 5-HT2B, except the 5-HT3 receptor where the Ki value was >3000 nM; different functional assays are consistent with this profile of selectivity. 24 The intrinsic activity in models of enteric nerve function (relative to 5-HT) has not been assessed 24 but in human isolated colon, prucalopride has subsequently been shown to increase cholinergic and nitrergic motor nerve function, with greater efficacy than tegaserod. 3 Against the channel encoded by the human ether-à-go-go related gene (hERG), expressed in HEK293 cells, prucalopride was found to inhibit activity only at relatively high concentrations (IC50 4.1 μM). 25 In humans, prucalopride is excreted largely unchanged in the urine and to a lesser extent, in the faeces. 26
An interesting characteristic of the 5-HT4 receptor is that although the receptor is expressed within a number of different tissues, where it can be demonstrated to be functionally-active (including cardiac muscle and certain neurons within the brain),27,28 5-HT4 receptor agonists are most effective as GI prokinetic agents, without clinically significant actions in other organs (see discussion on the clinical actions of prucalopride, below). To address this issue, the operational model of agonism was used to assess the effects of prucalopride and other 5-HT4 receptor agonists on porcine gastric and cardiac tissues. 29 These experiments suggested that 5-HT4 receptors within the ENS are more efficiently coupled to their effector mechanisms, relative to the cardiac receptors. This conclusion is consistent with a number of observations which show that selective 5-HT4 receptor agonists have high intrinsic activity (relative to 5-HT) in assays measuring the ability to facilitate cholinergic function in isolated GI tissues, but low intrinsic activity in assays using other tissues expressing the receptor, including cardiac muscle. In addition, the ability of prucalopride to facilitate cholinergic function in the pig isolated stomach appeared to be long lasting and not subject to the rapid desensitization observed using pig atrium. 30 The result is that when 5-HT4 receptor agonists are given as drugs, they increase GI motility without necessarily influencing functions in other tissues. The explanation is unclear but one possibility is that variations in distributions of COOH-terminal splice variants of the 5-HT4 receptor endow different coupling efficiencies and/or desensitization liabilities. These data provide an attractive hypothesis although considerable uncertainty remains. 31
Comparison with earlier 5-HT4 receptor agonist drugs
Non-selective and/or low-efficacy 5-HT4 receptor agonists.

The clinical context
Chronic constipation is certainly common with prevalence rates of up to 28% being reported in the US;
39
constipation is at least twice as common in women as in men and its occurrence increases with advancing age, particularly after age 65.
39
41
While constipation may be associated with or caused by many underlying disease entities and a long list of pharmacological agents, we will confine our discussion to those in whom there is no obvious or detectable primary cause for their constipation: functional constipation, also referred to as chronic idiopathic constipation and commonly found in the literature under the heading of chronic constipation (CC). Nowadays, clinical trial entry criteria for CC, as for other so-called functional gastrointestinal disorders, are usually governed by the Rome criteria, whose most recent iteration, Rome III, defined functional constipation as a symptom complex which must include ≥2 of the following:
Straining,∗ Lumpy or hard stools,∗ Sensation of incomplete evacuation,∗ Sensation of anorectal obstruction/blockage,∗ Manual maneuvers to facilitate defecation (eg, digital evacuation, support of the pelvic floor),∗ <3 defecations/week.
Furthermore, each of the symptoms denoted by an asterisk must occur in relation to ≥25% of defecations. In addition, loose stool should rarely be present without the use of laxatives and there must be insufficient criteria for the diagnosis of constipation-predominant irritable bowel syndrome (IBS-C). 42
Chronic idiopathic constipation is traditionally divided into two broad categories, slow-transit constipation (colonic inertia) and ‘outlet-type’ constipation, also referred to as defecatory dysfunction and anismus. 43 In terms of symptom associations, the former would typically manifest as infrequent stools, the latter as some difficulty associated with the act of defecation. While this distinction is attractive from the pathophysiological point of view, such a clear separation is often difficult, if not impossible, in clinical practice. Indeed, it is commonplace to find patients complain of symptomatology suggestive of both disorders, ie, infrequent stool frequency combined with straining and/or a sensation of incomplete evacuation, for example. These distinctions have important therapeutic implications given that prokinetic agents, the focus of this review, would be expected to have their greatest impact among those with delayed transit and that colectomy, the most drastic intervention that one may contemplate in the management of constipation, should be considered only among those with severe refractory colonic inertia. Furthermore, colectomy should not be contemplated in any patient where symptoms and/or the clinical evaluation suggest the presence of pelvic floor or other “outlet” problems. Because of the limitations of symptoms in predicting underlying dysfunction, and the consequent likelihood that slow transit and defecatory dysfunction may coexist in any given patient the results of a therapeutic intervention which was targeted at, say slow transit, must be interpreted with caution.
Irritable bowel syndrome (IBS) is one of the most common disorders encountered in modern medicine; community surveys in Western Europe and North America suggesting a prevalence of around 10% in the adult population.44,45 It should be stressed, in addition, that IBS appears to be common world-wide regardless of geography or socioeconomic status. There is no single specific diagnostic test for IBS; its definition relies, therefore, either on the exclusion of diseases that may share its symptomatology in whole or in part, or on the application of symptom-based criteria whose integrity has been validated in cross-sectional and longitudinal studies. The cardinal symptoms of IBS are abdominal pain/discomfort and bowel dysfunction; typically, these are interrelated such that, for example, an affected patient may report that his or, more likely, her, symptoms worsen when constipated, only to be relieved once a bowel movement has been achieved. In clinical research, most studies apply the definitions enshrined in the Rome criteria, whose third iteration (Rome III) was released in early 2006 and defined IBS as:
Recurrent abdominal pain or discomfort (an uncomfortable sensation not described as pain) at least 3 days per month in the last 3 months associated with 2 or more of the following:
improvement with defecation, onset associated with a change in frequency of stool, onset associated with a change in form (appearance) of stool.
These criteria should have been fulfilled for the last 3 months with symptom onset at least 6 months prior to diagnosis. 42
IBS is sub-typed based on predominant bowel habit at the time of presentation as:
IBS-D, where diarrhea is the predominant bowel habit, IBS-C, where constipation predominates; and defined as, hard or lumpy stools (scored as 1 or 2 on the Bristol Stool Form Scale) ≥25% of defecations and, in conjunction, loose or watery stools (scored as 6 or 7 on the Bristol Stool Form Scale <25% of defecations, IBS-M (mixed), where both diarrhea and constipation occur, and, IBS-U (unclassified), where the subject does not fit into one of the above categories.
Currently, IBS lacks an objective test or biomarker to confirm or refute the diagnosis, monitor progress or evaluate response to treatment; this remains a major obstacle to progress. As individual IBS symptoms are very non-specific and may occur in a host of other clinical conditions, the potential for diagnostic confusion is considerable. Even when taken collectively, as in the Rome criteria, the potential for diagnostic overlap persists unless the criteria become overly restrictive and this is of special relevance to the potential for overlap between IBS-C and CC. Where, indeed, does IBS-C end and CC begin? Right now this is a value judgment and is based on how much pain and discomfort one is prepared to accept in a patient with constipation. It will be the experience of every clinician that many patients with constipation complain of bloating, distension and abdominal discomfort, cardinal symptoms of IBS, it is the opinion of this author that it is only the degree or prominence of these symptoms that differentiates IBS-C from CC; a differentiation that often seems arbitrary, if not impossible, in clinical practice. It should come as no surprise that many of the therapeutic classes that demonstrate efficacy in CC are then evaluated in IBS-C.
Motility in constipation and irritable bowel syndrome
While defecatory dysfunction is thought to be due to dysfunction at the level of the pelvic floor and, thus, is not a colonic motor disorder per se, slow-transit constipation is presumed to reflect a primary disorder of colonic motility. In support of this presumption, these patients who, by definition, have slow colonic transit, have been shown to demonstrate a variety of motor abnormalities on manometric studies of the colon. Foremost among these and the one that has been adopted for use in clinical testing, is slow transit through the entire colon or in segments of the colon.
In clinical practice, colon transit is most usually measured using the radio-opaque marker technique. 46 This approach has been shown to provide, not only an accurate and reproducible assessment of overall colonic transit, but has also been shown to facilitate separation of colonic inertia from “outlet” problems. In this way, treatment strategies can be more accurately planned.
More accurate and dynamic assessments of colon transit, including the determination of transit within segments of various segments of the colon can be obtained from radio-isotopic approaches. Though these methodologies have been largely confined to a few centers, they have been widely used in the initial assessment of potentially colo-kinetic drugs in clinical research protocols.47,48
More direct assessments of colonic motor function can be obtained by manometry. However, colonic manometry presents formidable challenges foremost among these being that of positioning the catheter assembly in the first place and ensuring that it retains its position throughout the period of study. Furthermore, patterns of colonic motility are poorly defined and subject to tremendous variation between normal individuals, not to mention in disease states. While the absence of the most recognizable pressure wave pattern, the high amplitude power contraction (HAPC), during a recording period of appropriate duration, as well as following exposure to adequate stimulation, has been proposed as being of diagnostic value among children and both a reduced frequency and amplitude of HAPCs and an impaired colonic motor response to food and exercise have been reported among adults with CC, there is at present no consensus with regard to the utility of colonic manometry in clinical practice in the adult patient49,50 and the role of this modality in drug development has been very limited.
A condition such as IBS, whose definition rests exclusively on the interpretation of symptoms, is certain to encompass a heterogeneous population whose constituents may ultimately be found to have different causes. Not surprisingly, the search for a unifying hypothesis to explain all IBS has proven unfruitful. Several phenomena undoubtedly contribute to symptom genesis, including disordered bowel motility (“spasm”), increased bowel sensitivity (visceral hypersensitivity or hyperalgesia), altered cerebral processing of gut events, environmental stressors and intrinsic psychopathology. 51
While a variety of abnormal electromyographic and motor patterns have been described in the various parts of the gastrointestinal tract in IBS, the specificity of any of these for IBS remains unclear 52 and interest has shifted to the role of colorectal sensation in the pathogenesis of symptoms in IBS. 53
Current treatment options
There is currently a great need for new, efficacious and safe GI prokinetic drugs. 54 Since the withdrawal of tegaserod, lubiprostone is now the only alternative which is available for prescription in either constipation or constipation-predominant IBS. The drug is currently only available in the USA for treatment of chronic idiopathic constipation and for female patients with constipation-predominant IBS in women (http://www.sucampo.com/products.html). It needs to be stressed that the approved doses of lubiprostone for chronic constipation and constipation-predominant IBS are quite different: 24 mcg twice a day for the former and 8 mcg twice a day for the latter. As a consequence, rates for nausea, the most prevalent side effect, have averaged 8% in the C-IBS trials, in contrast to 29% in the CC studies.
Lubiprostone is effective because it activates ClC-2 chloride channels, stimulating chloride efflux into the lumen. As a consequence, water moves into the lumen to soften stools, improve the frequency of bowel movements and stool consistency, reducing the severity of the constipation. 55 The ClC-2 channel is expressed on the luminal surface of the epithelial cells lining the gut, but also exists outside the gut, most notably in the lung. Lubiprostone works as a drug because it is poorly absorbed following oral administration, so its effects are mediated locally within the intestine but not at ClC-2 channels outside the gut. Interestingly, lubiprostone was derived from the structure of prostaglandin E1 and retains an ability to activate prostaglandin EP receptors. 56 Further work is now needed to determine if the latter activity can explain the ability of lubiprostone to cause nausea in up to 31% of patients, 57 and contribute to the reason why lubiprostone carries a pregnancy category C label.
prucalopride for constipation
In healthy volunteers, scintigraphic studies using the radioisotpic technique developed at the Mayo Clinic,47,48 demonstrated that prucalopride accelerates whole gut and colonic transit but not gastric emptying or small bowel transit. 58 Among patients with constipation, on the other hand, the very same authors using the exact same scintigraphic technique found that prucalopride in doses of 2 or 4 mg daily accelerated whole gut, gastric, small bowel and colonic transit in constipated patients. 59 Importantly, prucalopride does not appear to adversely affect a number of parameters of anorectal motor function or impair rectal sensation in either healthy volunteers or constipated patients. 59 62 In studies of colonic motility, prucalopride have been shown to be stimulatory.63,64
Given the profile of pharmacological effects in vivo described above, it should come as no surprise that the major clinical focus of prucalopride has been in constipation.63,65–67 Indeed, each of the three major studies of prucalopride in man has been in CC.65–67 For reasons related to the transfer of the drug from one company to another, these trials have only been published recently even though they were actually designed and completed some time ago. These three trials, which became pivotal in terms of regulatory submission, featured a randomized, placebo-controlled, parallel group design. The major inclusion criterion was the presence of CC, defined as two or fewer spontaneous complete bowel movements (SCBM) per week for ≥6 months prior to screening plus any one of the following: hard/very hard stools, a sensation of incomplete evacuation, or straining during defecation with at least 25% of bowel movements. After a 2 week baseline period, eligible patients were randomized to either placebo, 2 mg or 4 mg of prucalopride for 12 weeks. The primary endpoint, in each study, was the proportion of patients passing ≥3 spontaneous complete bowel movements (SCBM) per week during the 12 weeks of the trial, based on an intention to treat analysis. All three trials (which assessed 620, 641, and 713 patients, respectively) demonstrated a significant increase in the proportion of patients achieving ≥3 SCBMs per week compared with placebo. Response rate ranged from 19.5%-31% with 2 mg prucalopride, 24%-28% with 4 mg, compared with 9.6%-12% with placebo. Clinically relevant and statistically significant improvements were also demonstrated in a number of secondary endpoints including satisfaction with bowel function, perception of constipation severity, and patient-assessed symptom scores. A validated, disease specific quality of life instrument (PAC-QOL), 68 but not a generic quality of life instrument (SF-36), showed significant improvements with prucalopride. 65 67 These benefits were supported in smaller studies of CC62,63 as well as in studies of special populations, the elderly, 69 those with severe, refractory constipation, 70 opioid-induced constipation 71 and constipation related to spinal cord injury. 72 To date there is very limited data on the impact of prucalopride on motility disorders affecting other parts of the gastrointestinal tract 73 and it is certainly too early to assess its potential usefulness in disorders such as gastroparesis, intestinal pseudo-obstruction, functional dyspepsia and, most importantly, C-IBS.
Given the cardiac adverse history that led to the withdrawal of certain non-selective 5-HT4 agonists, cisapride and tegaserod, considerable attention has been paid to the safety profile of prucalopride and to its cardiac toxicity, in particular.
The relationship between cisapride and cardiac adverse events has been delineated in great detail and has been shown to involve the ability of this drug to block the human ether-á-go-go-related gene (hERG), which encodes the rapidly activating delayed rectifier K+ current and is important in cardiac repolarization. 74 As a consequence, the QTc was prolonged and the susceptibility to arrhythmias such as torsades de pointes increased. A number of sudden deaths were reported.
The situation with respect to the cardiovascular toxicity of tegaserod is less clear. An analysis of data collected from 29 clinical studies involving over 18,000 patients demonstrated adverse cardiovascular events in 13 of 11,614 patients treated with tegaserod (a rate of 0.11%) compared with 1 of 7,031 patients treated with placebo (a rate of 0.01%). 75 In contrast, a very recent matched cohort study conducted using a large health insurance database from the US and involving 52,229 patients treated with tegaserod and 52,229 matched individuals who were not, failed to identify an increased risk for either cardiac events or stroke among those treated with tegaserod. 76 Thus, the true relationship between tegaserod and any adverse cardiovascular outcomes remains uncertain and the pathogenesis of any association unclear. There is a suggestion that tegaserod, acting perhaps through a 5-HT2 rather than 5-HT4 receptors, may promote platelet aggregation; 77 the relationship of this observation to any observed clinical events is unclear.
Turning to the experience to date with prucalopride; in the pivotal studies, which collectively represent the largest experience with the drug, the most common treatment associated adverse events were headache (25%-30% prucalopride; 12%-17% placebo), nausea (12%-24%; 8%-14%), abdominal pain or cramps (16%-23%; 11%-19%) and diarrhea (12%-19%; 3%-5%). 65 67 The majority of these adverse events occurred within the first 24 hours of treatment and were transient. Where reported, the prevalence of serious adverse events were similar for placebo and prucalopride.65,66
Of critical importance given the aforementioned experience with cisapride, prucalopride has not been found to interact with the hERG potassium channel in clinically-relevant concentrations.25,78 Furthermore no significant hemodynamic or clinically relevant electrocardiographic changes were detected in healthy control studies 79 nor were they detected in any of the major clinical trials.65–67,80 In a smaller study in a relatively high-risk population (eighty-nine elderly nursing home residents, of whom 80% had a prior history of cardiovascular disease) no significant hemodynamic or electrocardiographic changes were detected. Furthermore, instances of prolongation of the QTc interval were not more common among patients treated with prucalopride. 81 The data with regard to the hERG channel and QT interval prolongation are certainly re-assuring; however, given that adverse cardiac event with other serotonergic agents were detected only following the exposure of large numbers of patients, it seems wise to retain a watching brief for such events in relation to prucalopride as it becomes more widely used.
Future competition for prucalopride
This includes other 5-HT4 receptor agonists reported to be in various stages of development. These compounds have varying degrees of selectivity32,82,83 but among those reporting selectivity for the 5-HT4 receptor are naronapride (ATI-7505) 84 and velusetrag (TD-5108), 85 the latter recently reporting good tolerance and efficacy in a four week clinical trial in patients with chronic idiopathic constipation. 86 The developers of each molecule must now be working towards ways of differentiating their compounds from prucalopride. An alternative to 5-HT4 receptor agonists is provided by the peptide linaclotide (MD01100), which is a selective agonist at the guanylate cyclase C (GC-C) receptor. 87 Linaclotide is currently in development for idiopathic constipation and cIBS (http://ironwoodpharma.com/aboutus.php). GC-C receptors are expressed on the luminal surface of intestinal epithelial cells 88 and are normally activated by the guanylin family of endogenous peptides. 89 Activation opens the cystic fibrosis transmembrane conductance regulator to secrete chloride and bicarbonate ions into the lumen of the intestine, followed by an increase in fluid secretion, a decrease in colonic fluid absorption and increased GI transit. 90 Interestingly, linaclotide has recently been shown to exert anti-nociceptive activity in rodent models of visceral pain; this effect was absent in GC-C null mice. 91 Exactly how GC-C receptors are involved in the mechanisms of pain is now the subject of speculation and requires further examination. In women with constipation-predominant IBS, linaclotide may increase colonic emptying and stool frequency, as well as abdominal pain/discomfort and global assessments (using a rating scale).92,93 Linaclotide does not achieve systemic exposure after oral administration, so these effects occurred in the absence of serious adverse events.
Conclusions
The 5-HT4 receptor has had a difficult adolescence, receiving a tarnished reputation over the non-selective actions and poor intrinsic activity of drugs such as cisapride and tegaserod. In some parts of the pharmaceutical industry it then appeared logical to move away from gastrointestinal science and look for alternative opportunities within the “drug discovery process”, particularly in less mature areas of biology (which by definition, start with less ‘baggage'). A few others took time to understand the problem and the result is the delivery of a new class of drug, exemplified by prucalopride and defined by selectivity and high intrinsic activity at the 5-HT4 receptor.
For prucalopride and also for lubiprostone, it is significant that the first indication is for the treatment of chronic constipation, rather than constipation-predominant IBS. This trend towards first evaluating the effects of new drugs which change GI motility in disorders where disrupted GI motility is known to exist (rather than in functional bowel disorders where changes in motility are uncertain), seems likely to increase the success rate for GI drug development. It will be a great pity if prucalopride is now not progressed towards the C-IBS clinical population (for reasons associated with poor patent life and mixed ownership of the drug), but perhaps it has shown the way for other 5-HT4 receptor agonists. Most notable is TD-5108 (velusetrag), also characterized as a molecule with good selectivity at the 5-HT4 receptor, high intrinsic activity and most recently, clinical evidence of efficacy in patients with chronic constipation.
Footnotes
Acknowledgments
GJS is supported through a skills gap award from the Medical Research Council. EMMQ is supported in part through a grant from Science Foundation Ireland to the Alimentary Pharmabiotic Centre at University College Cork.
This manuscript has been read and approved by all authors. This paper is unique and not under consideration by any other publication and has not been published elsewhere. GJS is currently in receipt of a research grant from GlaxoSmithKline and is a member of the IBS advisory board for SK Life Science Inc. EMMQ is a member of the advisory board for Movetis. The authors confirm that they have permission to reproduce any copyrighted material.