
Abstract
We report this case of a 63-year-old woman who presented with progressive illness characterized by abdominal pain, weight loss, anorexia, generalized weakness, and fatigue. The patient was found to have obstructive jaundice with multiple mass lesions in the liver, spleen, and kidney on computed tomography scan of abdomen. She developed cholangitis, necessitating an emergent endoscopic retrograde cholangiopancreatography with biliary stenting and decompression. Later, she was found to have hepatic sarcoidosis on wedge biopsy of the liver. Extrinsic compression of biliary tree from mass effect of sarcoid granulomas with superimposed biliary sepsis is rare.
Keywords
Introduction
Sarcoidosis is a systemic disease of unclear etiology, characterized by the formation of noncaseating granulomas. It most commonly affects individuals between 20 and 40 years of age. 1 A distinct second peak in incidence is seen in women aged >50 years.2,3 Patients with sarcoidosis frequently present with bilateral hilar lymphadenopathy and pulmonary infiltration; they may also present with ocular and skin lesions. Most patients are asymptomatic or have nonpulmonary symptoms. Symptomatic patients may have symptoms such as cough, dyspnea, mild weight loss, or significant morbidity, including pulmonary hypertension, cor pulmonale, and respiratory failure. Extrathoracic involvement can occur in up to one-half of all patients with sarcoidosis, with liver being the most commonly involved after lymph nodes.1,4 However, symptomatic involvement of liver without any pulmonary manifestations is uncommon and occurs only in about 10% of patients. 5 The hepatic involvement in sarcoidosis is varied and ranges from intrahepatic cholestasis, with features of periductal fibrosis mimicking primary sclerosing cholangitis, to extrahepatic compression of biliary tree from adenopathy.6–8 Patients might also have a distinct hepatocellular and portal inflammation akin to chronic active hepatitis, while others present with sinusoidal congestion, particularly in zone 3. 9 We report a case of hepatic sarcoidosis that illustrates some of the above-mentioned histological features while presenting as septic cholangitis and extrahepatic biliary compression.
Case Report
A 63-year-old Hispanic woman, who was born and raised in the Dominican Republic, first presented to the emergency department with complaints of generalized weakness, fatigue, unintended weight loss, anorexia, progressively worsening abdominal pain, and fever of 5 days’ duration. She had sought medical care in the Dominican Republic for similar symptoms 2 months before the index admission when she was found to have biliary obstruction due to compression from infiltrative liver lesions of unclear etiology. She underwent endoscopic retrograde cholangiopancreatography (ERCP) with placement of a plastic stent within the common bile duct (CBD) at the time. Later, the patient underwent a laparoscopic liver biopsy, and a diagnosis of granulomatous hepatitis secondary to tuberculosis (TB) was made. She refused anti-TB therapy. She subsequently moved to the United States and had an admission at another institution, a week before our index admission, during which the plastic stent within the CBD was exchanged with a full-covered metal stent. She also had a history of essential hypertension and diabetes mellitus. On examination, vital parameters were as follows: a temperature of 101.2°F, pulse rate of 107 beats/minute, blood pressure of 86/51 mmHg. The patient was confused, not able to follow commands. Precordial examination showed normal heart sounds with no murmur, rub, or gallop. Examination of lungs showed bilateral air entry with no adventitious sounds. Abdomen was soft, with firm hepatomegaly and diffuse abdominal tenderness. Patient underwent endotracheal intubation with initiation of mechanical ventilation, broad-spectrum intravenous antibiotics, and vasopressor therapy.
Complete blood count showed hemoglobin of 7.7 g/dL, white cell count of 24.9 K/μL, and platelet count of 188 K/μL. Comprehensive metabolic panel showed the following results: sodium 133 mEq/L, potassium 3.3 mEq/L, bicarbonate 18 mEq/L, chloride 94 mEq/L, glucose 185 mg/dL, and serum creatinine 3.8 mg/dL. Liver function tests revealed 231 international units (IU)/L of alanine transaminase, 447 IU/L of aspartate transaminase, 373 IU/L of alkaline phosphatase (ALP), and 2.4 mg/dL of total bilirubin with a direct fraction of 2.1 mg/dL. Additional workup done for evaluation of abnormal liver enzymes, including viral hepatitis panels (hepatitis A, B, and C), antinuclear antibody, anti-smooth muscle antibody, anti-liver-kidney microsomal antibodies, anti-mitochondrial antibody were negative. A computed tomography (CT) scan of the abdomen showed cholelithiasis, an ill-defined soft tissue density within the porta hepatis surrounding the pancreatic head, celiac axis, and common hepatic artery (Fig. 1A), along with multiple hypodense lesions within the liver and spleen (Fig. 1B).

Ill-defined soft tissue density within the porta hepatis surrounding the pancreatic head, celiac axis, and common hepatic artery (
The patient underwent an urgent ERCP that revealed an inwardly migrated metallic biliary stent. The CBD was cannulated through the biliary stent and balloon sweeps were performed with removal of sludge (Fig. 2A). Resolution of biliary obstruction with flow of dark-colored bile was noted. A subsequent occlusion cholangiogram did not reveal any intrahepatic biliary strictures or dilation (Fig. 2B). Hemodynamic status of the patient improved significantly post-ERCP, at which time point she was weaned off both vasopressor therapy and mechanical ventilation. Jaundice resolved and liver enzymes, barring ALP, gradually normalized. ALP remained persistently elevated at levels >250 IU/L. A CT-guided targeted needle biopsy of liver lesions revealed mild to moderate ductular reaction without cholestasis, broad areas of perivenular fibrosis, and scattered foci of lobular necroinflanimation. No definitive diagnosis could be made with the biopsy specimen.

Metallic CBD stent filled with sludge (
The patient was discharged from the hospital and was subsequently admitted a few weeks later for an elective laparoscopic cholecystectomy. Laparoscopy revealed multiple, discrete pale-colored well-circumscribed lesions in the hepatic parenchyma (Fig. 3A). A wedge biopsy of the liver lesion was performed at the same time. The biopsy specimen revealed numerous non-necrotizing granulomas with epitheloid cells, multinucleated giant cells, and lymphocytes (Fig. 3B). Culture and staining for acid fast bacilli (AFB) were negative. Significant perivenular (zone 3) congestion and fibrosis were seen again (Fig. 3C). Patient was diagnosed as having extrapulmonary sarcoidosis with predominant hepatic involvement causing extrahepatic biliary obstruction and subsequent biliary sepsis.
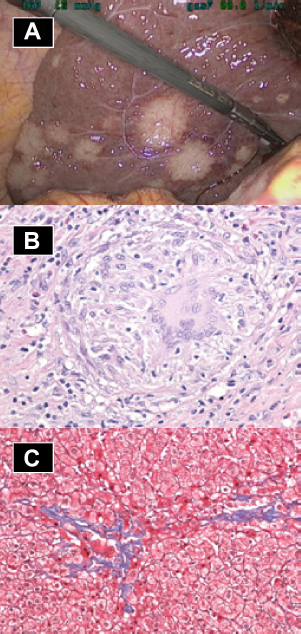
Multiple, discrete pale-colored well-circumscribed hepatic lesions seen during laparoscopy (
Discussion
Sarcoidosis is characterized by development of noncaseating granulomas in the involved organs. The prevalence and severity of sarcoidosis is highly heterogeneous across different races, with African Americans being most commonly affected.10,11 Data regarding prevalence of sarcoidosis in the Hispanic population are meager. There are multiple etiologies of hepatic granulomas of the liver, including autoimmune diseases such as sarcoidosis and primary biliary cirrhosis (PBC), infectious agents such as Mycobacterium tuberculosis, fungal infections including histoplasmosis and coccidiodomycosis, malignant lymphomas, and a wide variety of drugs.12–17 The likelihood of a disseminated fungal infection was considered as she had recently traveled to a known endemic area. The patient was not on any medication known to cause hepatic granulomas. In view of her constitutional symptoms and origin from a high-prevalence country, TB was also an important diagnosis to consider. However, biopsy findings of nonnecrotizing granulomas and negative AFB staining made TB unlikely. One of the most common causes of hepatic granulomas in the United States is sarcoidosis. It has been postulated that lack of screening modalities and competing diagnoses of infectious etiologies (including TB) might lead to underestimation of the burden of sarcoidosis in developing countries, as seen in our patient. 18
Abnormal elevation in liver function tests are found in a third of all patients, with ALP being the most commonly affected. 19 Bilirubinemia is unusual and happens in a setting of intrahepatic cholestasis, hepatocellular dysfunction, or, rarely, extrahepatic bile duct compression. 20 Enlarged lymph nodes are detected in approximately 30% of patients particularly in the porta hepatis, paraaortic region, and the celiac axis, and unlike lymphoma, the lymph nodes are typically smaller than 2 cm in diameter and more discrete rather than confluent. 21 Our case was unusual in its presentation, with extrahepatic biliary obstruction from porta hepatic lymphadenopathy leading to biliary sepsis. Biopsy also showed a concomitant hepatocellular injury pattern, a characteristic vascular pattern of sinusoidal and perivenular (zone 3) congestion but no intrahepatic cholestasis. Granulomas also showed the characteristic multinucleated giant cells not usually associated with other conditions such as PBC. 22 Radiological findings in this patient included multiple hypointense and hypoattenuating lesions in both liver and spleen on a contrast-enhanced CT of abdomen. These lesions represent coalesced sarcoid granulomas and can be seen in up to 15% of all patients with sarcoidosis. 23
Even though optimal therapy for hepatic sarcoidosis has not been validated, it has been thought that corticosteroid therapy might be useful in symptomatic patients with partial to complete response in up to two-thirds, including those with intrahepatic biliary strictures. 23 Utility of steroid-sparing immunosuppressive therapy with methotrexate has also been described.24,25 Sarcoidosis remains a rare indication of orthotropic liver transplantation. 26 To our knowledge, this case is among the very few cases that presented with sepsis from extrahepatic biliary obstruction from sarcoid lymphadenopathy.
Author Contributions
Conceived and designed the experiments: VG, RI, SS and HT. Wrote the first draft of the manuscript: VG, RI, HT. Contributed to the writing of the manuscript: SS, MN, AR, SS. Agree with manuscript results and conclusions: SC. Jointly developed the structure and arguments for the paper: VG, HT, SC. Made critical revisions and approved final version: SC. All authors reviewed and approved of the final manuscript.