
Abstract
Introduction
Pancreatic carcinoma affecting the uncinate process is a challenging surgical condition. Several considerations affect the management plan, including the need for vascular resection and the ability to achieve a clear margin.
Methods
The data of 19 patients who had curative resection for pancreatic adenocarcinoma of the uncinate process were reviewed. Operative mortality and morbidity, and disease-free survival (DFS) were calculated.
Results
The study population included 13 male and 6 female patients with a mean age of 55 years. Nine patients (47.4%) had stage I disease, seven patients (36.8%) had stage II disease, and three patients (15.8%) had stage III disease. A total of 12 patients had Whipple procedure and 7 patients had total pancreatectomy. In total, there were 9 R0 and 10 R1 resections. Operative mortality rate was 10.5% (2/19), postoperative leakage rate was 21.1% (4/19), and wound sepsis rate was 21.1%. Median DFS was 19.2 months. Survival was superior in the Whipple procedure group than in the total pancreatectomy group (median survival 19 months vs 4 months, respectively). Vascular resection and retroperitoneal safety margin status did not affect disease relapse.
Conclusion
Non-metastatic pancreatic adenocarcinoma of the uncinate process should be offered R0 or R1 resection whenever technically feasible.
Introduction
Pancreatic carcinoma is an aggressive cancer with dismal prognosis. In the US, it is estimated that there will be 46,420 new cases and 39,590 deaths in 2014. The disease accounts for 7% of all cancer mortality in the US, and the five-year survival rate is 6%. 1 In Egypt, pancreatic cancer accounts for 2% of all cancers, with an age-adjusted incidence of 3.2/100,000, which is roughly half of the US incidence rate. 2 Survival rates for pancreatic cancer patients in the US have improved significantly in recent decades, from 2% in 1975-1977 to 6% in 2003-2009. 1 Refinement in the pancreaticoduodenectomy procedure is probably responsible for much of this effect.3–6
Surgical resection remains the only hope for long-term survival,3,5,7 and resectable cases have a five-year survival rate of 14.6%. 8 Thus, pancreatic cancers are broadly categorized as resectable, borderline resectable, and advanced. Borderline resectable cancers abut but do not encase one of the nearby vascular structures, such as the portal vein or the superior mesenteric vessels. 8 The latter are intimately related to the uncinate process of the pancreas. Hence, a tumor located in the uncinate process involves the superior mesenteric vein (SMV) or artery early in its course. Many authors believe that the abovementioned anatomical complexity does not preclude surgical resection of early uncinate carcinoma,9,10 and some argue that tumor abutment on the superior mesenteric/portal venous confluence does not predict poor outcome. 11 Recently, there has been much interest in widening the scope of resection in pancreatic uncinate carcinoma.9,10 We undertake this study to investigate whether this approach can be applied in middle-volume center practice.
Methods
This report presents a retrospective analysis of prospectively collected data of patients presenting to Mansoura University Cancer Center in Egypt with pancreatic adenocarcinoma originating in or extending to the uncinate process. Non-adenocarcinoma pathology and patients who were offered palliative surgery or no surgery were excluded from the analysis. All clinical procedures were conducted in accordance with the guidelines of the ethics committee of the Faculty of Medicine, Mansoura University, and after obtaining the written informed consent of the patients. This is a retrospective study and IRB approval was not required. This study complies with the principles of the Declaration of Helsinki. Recorded parameters included patient presenting symptoms, degree of clinical and biochemical jaundice, blood glucose, CA19-9, staging according to the seventh edition of the American Joint Committee on Cancer (AJCC) staging manual, 12 tumor size according to the CT scan (preoperative) and pathology report (postoperative), operative details, last visit records, and disease-specific survival. Descriptive data were presented as median ± standard deviation as appropriate. Univariate analysis of the factors affecting relapse was calculated using chi-squared test and Fisher's exact test. Disease-free survival (DFS) was calculated using Kaplan–Meyer analysis. Statistics were calculated with SPSS GradPack® version 17 (IBM Corp.).
Results
The present cohort of patients represent all consecutive pancreatic adenocarcinoma patients presenting to our service in the period from June 2008 to June 2013 whose cancer originated in or invaded the uncinate process. Data of 23 patients were extracted from the archived files, and 4 patients who were not offered resection for curative intent were excluded. Further analysis included the 19 patients who were treated for pancreatic adenocarcinoma with either conventional Whipple pancreaticoduodenectomy or total pancreatectomy. Baseline criteria are summarized in Table 1.
The clinicopathological features of the patients. Staging was according to the seventh edition of the AJCC staging manual, Stage I: tumor limited to the pancreas, Stage II: tumor extends beyond the pancreas without major vascular infiltration, and Stage III: tumor with major vascular infiltration.

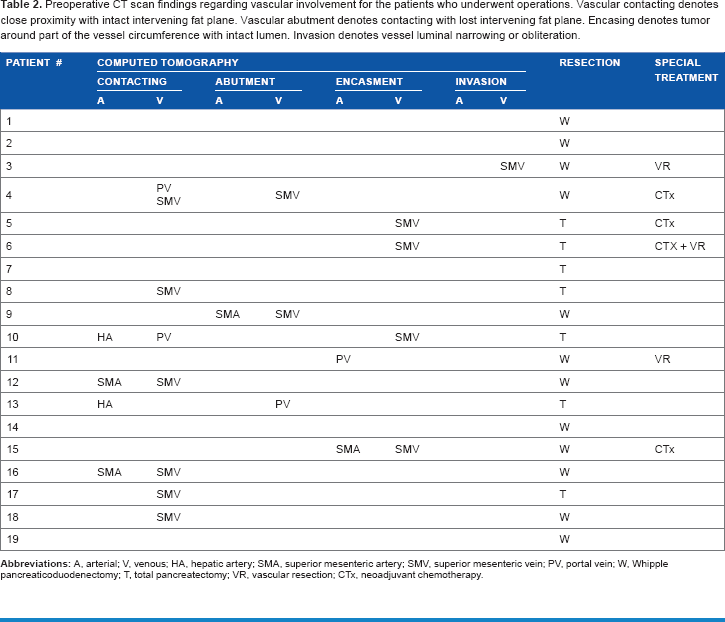
In all, 12 patients had Whipple resection and 7 patients were offered total pancreaticoduodenectomy because of tumor location. Postoperative chemotherapy was used in all cases and consisted of six months of 1 gm/m2 gemcitabine (IV) at days 1, 8, and 15. Four patients received preoperative chemotherapy for the absence of the fat plane between the tumor and the mesenteric vein, demonstrated on a preoperative CT scan (Table 2). In total, there were 9 R0 and 10 R1 resections. There were two cases of in-hospital mortality caused by massive pulmonary embolism two days after the surgery. Postoperative leakage rate was 21.1% (4/19), and wound sepsis rate was 21.1%. Postoperative leakage was defined as ≥50 mL of drainage for ≥3 days with ≥3 times serum level of amylase and/or bilirubin. Accordingly, two patients had persistent biliary leak and two other patients had pancreatic leak. All four patients were reoperated. Wound sepsis occurred in four patients.
Preoperative CT scan findings regarding vascular involvement for the patients who underwent operations. Vascular contacting denotes close proximity with intact intervening fat plane. Vascular abutment denotes contacting with lost intervening fat plane. Encasing denotes tumor around part of the vessel circumference with intact lumen. Invasion denotes vessel luminal narrowing or obliteration.
All patients were followed for the occurrence of relapse. Median DFS for the whole group was 19.2 months (95% CI = 11.2-27.3 months). On univariate analysis, the type of resection (Whipple vs. total pancreatectomy), infiltration of the retroperitoneal safety margin, and the presence of vascular resection did not affect the relapse rate (all P-values = NS; chi-square test). Patients who received total pancreaticoduodenectomy had shorter DFS than patients who underwent Whipple resection. The presence of vascular resection did not affect DFS in this cohort (Figs. 1 and 2). Similarly, 12 patients with free retroperitoneal margin and 7 patients with infiltrated margin had no significant difference in median DFS (19.22 vs. 17.87 months; P = NS; log-rank, Mantel-Cox tests). Only three patients had an infiltrated pancreatic transaction margin and one patient had a narrow transaction margin. Three other patients were offered vascular resection, and their data are summarized below.
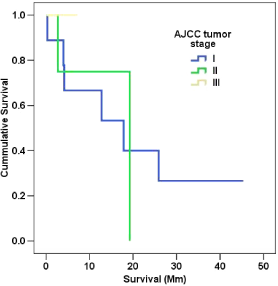
DFs according to tumor stage.

DFS according to retroperitoneal margin status.
Patient 1 was a male in his 40s presenting with marked jaundice, intolerable pain, and recent onset diabetes. A preoperative CT scan revealed a 5-cm mass in the head and uncinate process of the pancreas encasing the SMV. A post-neoadjuvant therapy CT scan showed a 2.8-cm mass related to SMV and a single pulmonary nodule. Total pancreatectomy, resection of the SMV, and synthetic graft repair were performed. Postoperative pathology reported a 4-cm mass invading the duodenum, satellites in the pancreatic body, free retroperitoneal margin, free vein wall, and free pancreatic transaction margin. The patient succumbed to massive pulmonary embolism.
Patient 2, a male in his 50s diabetic, presented with moderate pain and moderate jaundice. Preoperative CT scan showed a 2.5-cm mass in the head of the pancreas with lost fat plane with the portal vein. Whipple pancreaticoduodenectomy with resection of a portal vein segment and end-to-end anastomosis was done (Fig. 3). Postoperative pathology revealed a GII adenocarcinoma with lymphovascular emboli, 5/7 infiltrated lymph nodes, invaded portal vein, and perineural invasion but free retroperitoneal margin. The patient was disease free on follow-up at 26 months.

Operative photographs of Patient 2. (From left to right) (
Patient 3 was a male in his 60s presenting with mild pain without jaundice. A preoperative CT scan reported a 5.5-cm mass in the head and uncinate process of the pancreas infiltrating at least 1/4 of the circumference of a 3-cm segment of the SMV. Whipple pancreaticoduodenectomy with vascular resection and synthetic graft repair was done (Fig. 4). Postoperative pathology revealed a 4-cm GII adenocarcinoma with invaded 1/9 lymph nodes, invaded SMV, and infiltrated retroperitoneal margin. The pancreatic resection margin was free of tumor invasion. The patient was disease-free on follow-up at nine months.

Operative photograph of Patient 3. Left panel: operative bed of the mobilized pancreas showing the portal vein, the superior mesenteric vein infiltrated with the tumor, and the superior mesenteric vein stump. Right panel: completed synthetic graft anastomosis. Inset panel: operative specimen photograph showing the posterior aspect of the pancreas and cannulated superior mesenteric vein segment.
Discussion
Uncinate process carcinoma is a technically challenging condition from a surgical perspective. Diagnosis is often late because of late onset of jaundice. Uncinate process tumors are notorious, particularly for poor outcome, because of technical complications related to vascular surgery or the frequent inability to achieve a retroperitoneal-free pathological safety margin.13–15
Previous studies of treatment outcome after curative resection of uncinate process carcinoma recorded a mortality rate of 0-10%. 14 One series of 10 patients with uncinate tumors was published by Li and colleagues in 2002. 9 Seven of the operated cases had portal vein resection. These authors reported one case of early postoperative mortality and a median survival of 17 months. A larger study of 59 patients was published by Ye and colleagues, 16 of whom had vascular resection as a part of their surgery. 10 The median survival time of the whole cohort was 12.1 months. Both studies are comparable with the results of the present study. In a larger study comparing uncinate process cancer with usual pancreatic head cancer, uncinate carcinomas were found to have a median DFS time of 15.2 months and were equivalent to that of pancreatic head tumors. 16
There has been much discussion and debate among pancreatologists regarding the impact of safety margin status on disease outcome. Reports are heterogeneous regarding the technique of pathological sample handling, serial sectioning procedures, and the minimal margin deemed adequate. 17 Multiple publications have emphasized the prognostic impact of margin status.4,6,18–21 Other reports, however, have not found any effect of margin infiltration on patients’ overall survival rates.22–26 Elaborate pathological studies have helped to clarify the controversy. Recent reports suggested that the pancreatic transaction margin, in particular, is the critical factor affecting tumor relapse.25,26 Positively infiltrated pancreatic tissue at the medial transaction margin implies a massive and/or multicentric tumor, and has been associated with disease relapse and poor prognosis. It seems that retroperitoneal margin infiltration does not carry the same prognostic importance. 24 Although there is no direct evidence for this hypothesis, we speculate that contemporary adjuvant treatment may help clear the superior mesenteric vessels of the mild microscopic tumor burden that is often associated with uncinate process enucleation. It is intuitive to believe that the larger tumor burden associated with bulky or multicentric tumors would be less amenable to the chemotherapeutic effect.
In our cohort, patients who underwent Whipple resection had longer DFS than patients who had total pancreaticoduodenectomy. Although the latter group had larger tumor size, we do not have enough evidence to conclude whether their worse outcome was because of more advanced cancers or because of the operative technique itself.
Conclusion
Operative treatment with curative intent should be offered in all cases with uncinate process carcinoma whenever technically feasible. Our data suggest that tumor enucleation with or without vascular resection is of benefit to the patient. All efforts should be taken to avoid macroscopic tumor residue (R2 resection), including resection of the superior mesenteric and/or portal vein when these vessels appear to be affected at operation (Table 3).
summary of suggested recommendations for uncinate process carcinoma.

Author Contributions
Conceived and designed the research plan: SR and OH. Analyzed the data: OH and AA. Wrote the first draft of the manuscript: OH. Contributed to the writing of the manuscript: AS. Agree with manuscript results and conclusions: SR, OH, AA, KA and AS. Jointly developed the structure and arguments of the paper: SR, OH, KA and AA. Made critical revisions and approved final version: SR and OH. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
The authors are indebted to the staff of the Surgical Oncology Department, Pathology Department, and Radiology Department of the Mansoura University Cancer Center for their continued help and support.