
Abstract
Abdominal hernias are a common cause of bowel obstruction. The major types of abdominal hernias are external or abdominal wall hernias, which occur at areas of congenital or acquired weakness in the abdominal wall. An alternative entity is internal hernias, which are characterized by a protrusion of viscera through the peritoneum or mesentery. We herein present the case of a female peritoneal dialysis patient with bowel obstruction due to an internal hernia. Although an initial work-up did not lead to a correct diagnosis, an exploratory laparotomy revealed that she had intestinal herniation due to a defect in the broad ligament of the uterus, which was promptly corrected by surgery. The concerns about the perioperative dialytic management as well as the diagnostic problems regarding the disease that arose in our experience with the present patient are also discussed.
Introduction
Abdominal hernias are a common cause of bowel obstruction. The major types of abdominal hernias are external or abdominal wall hernias, which occur at areas of congenital or acquired weakness in the abdominal wall. 1 Thus, the occasional link between such pathologies and peritoneal dialysis (PD), which is associated with increased intra-abdominal pressure, 2 may not be surprising. 3 A different entity is internal hernias, which are characterized by a protrusion of the viscera through the peritoneum or mesentery 4 and have been shown to account for approximately 0.5–5.8% of all cases of intestinal obstruction. 4 , 5 In this report, we describe our experience with a PD patient who was diagnosed with a bowel obstruction due to intestinal herniation, which occurred as a result of a defect of the broad ligament of the uterus. The patient has given consent for publication of details and images in this report.
Case Report
A 65-year-old woman who was treated with continuous ambulatory PD (CAPD) was admitted with lower abdominal pain of 1-day duration, which was followed by intermittent nausea and vomiting. She had chronic renal failure due to chronic glomerulonephritis, and had been treated for 22 months with CAPD (four daily exchanges; 2 L of Midperiq® 135
A Tenckhoff catheter was implanted through a classic transverse surgical incision, with a favorable postoperative course. Peritonitis was not noticed after the initiation of CAPD. The patient's blood parameters were acceptable, and her general condition was satisfactory. Her other medical history included hypertension, and she had undergone total hysterectomy because of a uterine myoma 15 years previously.
A physical examination conducted on admission revealed that she was alert and oriented, and had a body temperature of 36.6 °C. A clinical examination disclosed diffuse tenderness without peritoneal signs, while the abdomen was slightly distended and tympanic with diminished bowel sounds. The peritoneal fluid was clear, with a white blood cell (WBC) count of less than 50/mm3. The skin surrounding the peritoneal catheter, as well as the catheter's exit site, was unremarkable without any signs of inflammation. A laboratory evaluation revealed the following findings: WBC, 6300/mm3; hemoglobin, 8.0 g/dL; hematocrit, 22.7%; platelet count, 28.5 × 10 4 /mm3; blood urea nitrogen, 43 mg/dL; serum creatinine, 6.5 mg/dL; sodium, 137 mmol/L; potassium, 4.3 mmol/L; chloride, 104 mmol/L; and C-reactive protein, 0.44 mg/dL. Upright radiography showed some loops of dilated bowel with air-fluid levels (Fig. 1). Initially, a small bowel obstruction due to post-hysterectomy-related adhesion was suspected and she was managed conservatively. However, computed tomography (CT) of the abdomen, which was performed 2 days after admission, demonstrated discontinuity of the small bowel with a distended closed loop in the pelvic cavity (Fig. 2), suggesting that strangulation was the likely cause of the development of the bowel obstruction. She was therefore subjected to an exploratory laparotomy, which revealed incarcerated, small bowel herniation into the pouch of Douglas through a defect of the residual broad ligament of the uterus (Fig. 3A). Ten centimeters of the incarcerated bowel was slightly edematous (Fig. 3B); however, it was not ischemic and the entrapped bowel was freed using a bowel forceps, while the defect of the broad ligament was closed (Fig. 3C). No adhesion was observed between the adnexum and the small bowel. The PD catheter was also removed because the patient refused to continue with the PD. She started to receive hemodialysis (HD) three times per week via a right internal jugular vein catheter on the day after the operation. Finally, a wrist-arterio-venous fistula was created to provide permanent vascular access, and the periodic HD program was continued.

Abdominal X-ray showing mildly dilated loops of the bowel without fecal impaction.
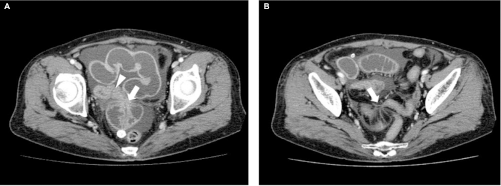
(
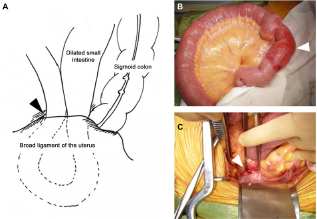
Findings of exploratory laparotomy. The schematic representation (
Discussion
Acute bowel obstruction is a common abdominal emergency. The majority of cases occur secondary to adhesion from prior surgery. 6 The remaining cases may be due to neoplasms, abdominal wall hernias, and, in decreasing frequency, Crohn's disease, volvulus, intussusception, bezoars, gallstones, trauma, and iatrogenic problems. 7 9 Bowel obstruction is rarely attributed to internal hernias.4,5,7–9 Broad ligament hernias are extremely rare and account for only a few percent of internal hernia cases. 4 In this regard, the paucity of literature describing the complications of internal hernias in patients who receive PD may not be surprising. To the best of our knowledge, this is the first report of a long-term PD patient with internal herniation that occurred because of a defect of the broad ligament of the uterus.
The broad ligaments of the uterus consist of layers of peritoneum that cover the intestinal and vesical surfaces, which are carried laterally in a tripod fashion to the side walls of the pelvis. 10 Based on the nature of the defects, the hernias can be classified into two categories: the fenestra type, with defects in both peritoneal layers, and the pouch type, with defects in only one of the two layers.4,11 As seen in the current patient, the viscera may be allowed to pass through the defect with potential hernial strangulation in subjects with fenestra-type hernias; otherwise, such structures may be permitted to enter and become entrapped in the parametrium in patients with pouch-type hernias. 4 The most common herniating viscus is the small intestine; less common structures include the sigmoid colon, ovaries, cecum, omentum, appendix, and the ureter. 10 The youngest patient ever described was 16 years of age, 12 while more than 85% of the cases have occurred in parous women. 10 A defect of the broad ligament is often present in a unilateral portion, and several etiological factors for such defects have been suggested, including trauma during pregnancy or delivery, surgical injury, pelvic inflammatory disease, and congenital anomalies.4,10–14 In the current case, the etiology of the disease could be multifactorial since our patient had a history of pregnancy, delivery, and abdominal surgery. Although it is difficult to determine the precise contributions of each factor, we believe that the patient's previous hysterectomy likely played a major role in the formation of the defect in the residual broad ligament. The tractive and/or stretching nature of PD, which is characterized by increased intra-abdominal pressure due to retention of dialysate, may have played an additional role in exacerbating the ligament fenestration, thereby predisposing our patient to the disease.
Hernias of the broad ligament have often been discovered at laparotomy for other reasons, and unless the defect is suspected after previous uteropexy the precise preoperative diagnosis of the disease is quite uncommon.10,15 This was also the case in the current patient. Indeed, a combination of the patient's medical history, which included a hysterectomy and an abdominal X-ray that showed the dilated loops of the bowel, encouraged us to initially attribute the illness to postoperative adhesion. Plain film radiography does not help with the specific diagnosis because of its low sensitivity and specificity. 16 Barium enema or other radiologic modalities, including CT, may occasionally lead to a correct diagnosis.10,17,18 The workup with the imaging analyses was not sufficient to allow a preoperative diagnosis of broad ligament herniation; however, the persistent ileus with the closed-loop obstruction, a CT finding that is suggestive of bowel strangulation, 9 led us to perform prompt surgical treatment, which likely played a pivotal role in avoiding bowel ischemia, necrosis, and perforation, which would have required intestinal resection and resulted in various degrees of complication.10,19,20 Abdominal wall hernias, localized PD catheter-related adhesions, and sclerosing encapsulating peritonitis, all of which may require prompt surgical intervention, are regarded as disease-specific causes of small bowel obstruction in patients with PD. 21 26 We believe that broad ligament herniation should always be regarded as the potential cause for the disease as well, especially in female patients who receive PD. This would lead to a high index of suspicion, prompt recognition, and immediate intervention, which are essential for reducing or preventing major morbidities of the disease. 27 Considering the fact that our patient did not require bowel resection, it might have been possible for her to resume PD at an intermittent schedule using low-volume dialysates despite the concerns about the leakage of dialysate and dehiscence because of poor wound healing mediated by abdominal distension.2,28–32 Finally, there are no clear recommendations regarding either the interruption or withdrawal of PD after abdominal surgery,20,31,32 and we gave priority to the patient's decision. The optimal therapeutic strategy for internal herniation in patients who receive PD may only be determined with the accumulation of experience from a larger number of cases similar to ours.
Author Contributions
Drafted the manuscript: NOT, TA. Contributed to the acquisition of the clinical data: AS, OS, SM, EK. Provided a detailed review of the contents and structure of the manuscript resulting in significant changes to the original document: AS, SM, DN. All authors have read and approved the final manuscript.