
Abstract
Background:
Peritoneal dialysis (PD) continues to be demanding for patients affected by kidney failure. In kidney failure patients with residual kidney function, the employment of incremental PD, a less onerous dialytic prescription, could translate into a decrease burden on both health systems and patients.
Methods:
Between 1st January 2009 and 31st December 2021, 182 patients who started continuous ambulatory peritoneal dialysis (CAPD) at our institution were included in the study. The CAPD population was divided into three groups according to the initial number of daily CAPD exchanges prescribed: one or two (50 patients, CAPD-1/2 group), three (97 patients, CAPD-3 group) and four (35 patients, CAPD-4 group), respectively.
Results:
Multivariate analysis showed a difference in term of peritonitis free survival in CAPD-1/2 in comparison to CAPD-3 (hazard ratio (HR): 2.20, p = 0.014) and CAPD-4 (HR: 2.98, p < 0.01). A tendency towards a lower hospitalisation rate (CAPD-3 and CAPD-4 vs. CAPD-1/2, p = 0.11 and 0.13, respectively) and decreased mortality (CAPD-3 and CAPD-4 vs. CAPD-1/2, p = 0.13 and 0.22, respectively) in patients who started PD with less than three daily exchanges was detected. No discrepancy of the difference of the mean values between baseline and 24 months residual kidney function was observed among the three groups (p = 0.33).
Conclusions:
One- or two-exchange CAPD start was associated with a lower risk of peritonitis in comparison to three- or four-exchange start. Furthermore, an initial PD prescription with less than three exchanges may be associated with an advantage in term of hospitalisation rate and patient survival.
This is a visual representation of the abstract.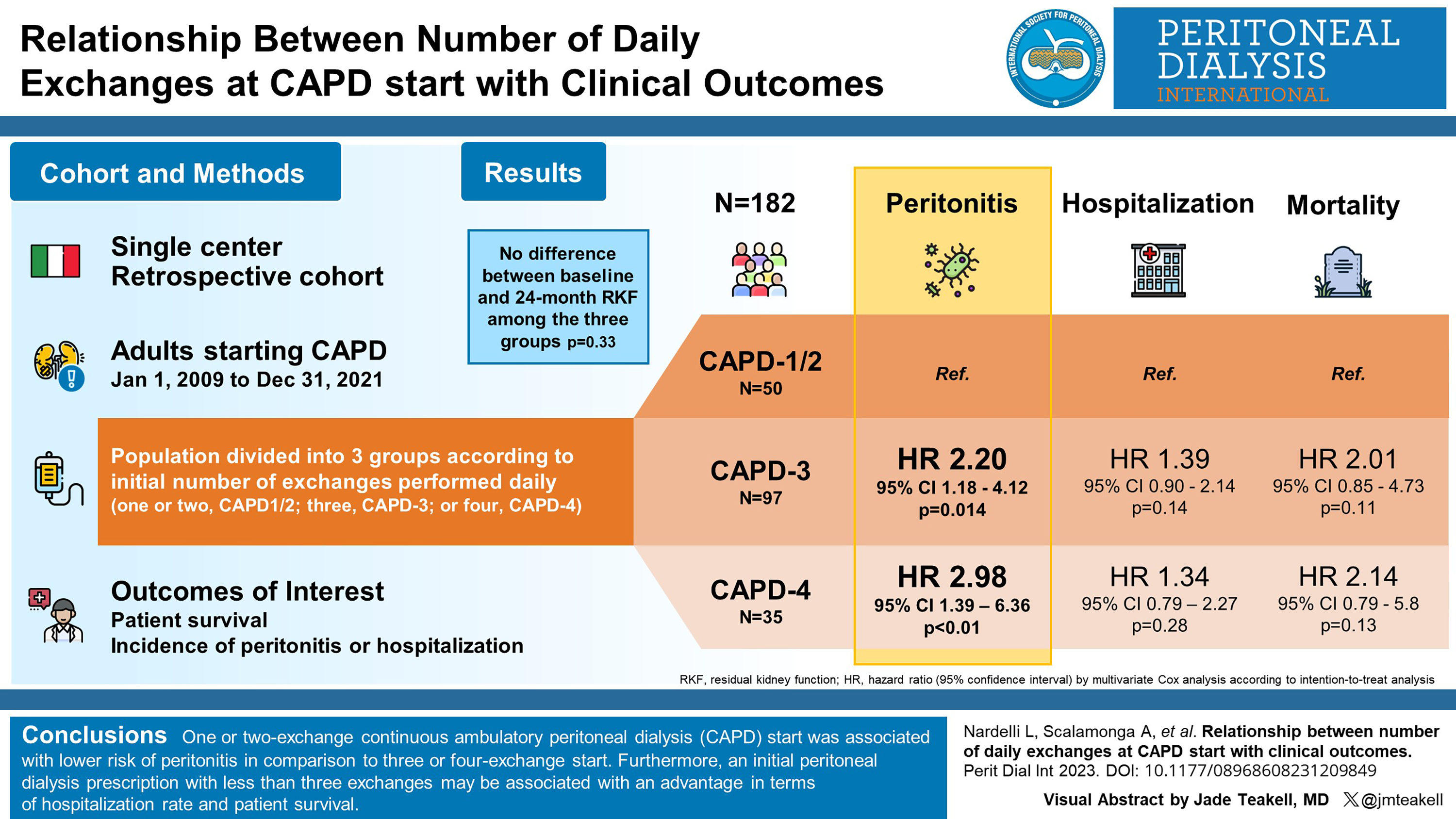
Introduction
The global dialysis population continues to grow every year and is projected to exceed five million by 2030. 1 When these numbers are considered in the light of the current scarcity of resources and climate changes as well as the global recession, the enormity of the economic and environmental impact of kidney replacement therapy becomes evident. 2 –5 In addition, dialysis continues to be extremely demanding for patients affected by kidney failure. 6 Thus, the employment of a less onerous dialytic prescription with no effect on patient outcomes would translate into a decrease burden on both health systems and patients. 7
It has been formulated that full-dose continuous ambulatory peritoneal dialysis (CAPD) is not required to achieve clearance targets in most new patients with substantial residual kidney function. 8 The modality consists of taking advantage of kidney contribution to fluid and solute removal to prescribe initially less burdensome peritoneal dialysis (PD) regime while still achieving individualised clearance targets.
This approach, referred to as incremental peritoneal dialysis (incPD), has been variably defined. 9 –11 Recently, incPD has been proposed as a strategy, rather than a specific regime by the International Society for Peritoneal Dialysis (ISPD). 12
IncPD may offer several potential advantages including preservation of RKF, lower peritonitis risk, glucose exposure, health-related cost, environmental waste, better PD adherence as well as improved quality of life. 10,13 –17 Conversely, some possible drawbacks are feared, such as reduced small solute clearance, increased risk of fluid overload, higher mortality and patient reluctance to increase PD prescription when required. 18
Thus, this study aims to evaluate the major clinical outcomes of an unselected PD population divided into three groups according to initial PD exchanges.
Methods
Study design and participants
This is a single-centre retrospective cohort study. Adults (>18 years) who started CAPD between 1st January 2009 and 31st December 2021 at IRCCS Ca’ Granda Foundation Maggiore Policlinico Hospital were included in the study. Patients who had a total follow-up less than 6 months or started PD with an automated cycler were excluded. All patients were followed up to the end of the study period or until the discontinuation of PD due to death, kidney transplantation, transfer to HD or to another PD centre.
The CAPD population was divided into three groups (CAPD-1/2, CAPD-3 and CAPD-4) according to the initial number of PD exchanges performed daily (one or two, three and four, respectively). The starting number of CAPD exchanges was chosen based on clinician variability, taking into account clinical parameters and patient’s willingness. The patients starting with one or two daily exchanges were gathered together for two reasons: (1) the number of subjects who initiated CAPD with one exchange was too small to fit statistical purpose; (2) the one- or two-exchange start meets the common Italian definition of incremental CAPD.
Age, sex, primary kidney disease, comorbidities, body mass index (BMI), creatinine and urea kidney clearance from a 24-h urine collection and residual urine output (mL/24 h) were recorded in an electronic database (Galenus®, Infogramma s.r.l., Milan, Italy). Modified Charlson comorbidity index for PD patients was calculated according to Cho et al. 19
Further measurements included urinary, peritoneal and total weekly Kt/V calculated from a 24-h urine/PD fluid collection as well as peritoneal permeability parameters obtained by a modified 3.86% peritoneal equilibration test (PET) carried out 1 month after the start of PD. 20 In addition, residual kidney function (RKF), urine output and dialysis small solute indicators were measured every 6 months and, when clinically indicated, a PET was performed. Peritonitis was diagnosed according to the ISPD 2022 guidelines, 21 and hospitalisation was defined as any event requiring admission to an in-patient unit.
CAPD dose prescription
After obtaining informed consent for catheter insertion, double-cuffed Tenckhoff catheter was placed by an interventional nephrologist according to semi-surgical or surgical procedure described thoroughly elsewhere. 22 –24
Incremental CAPD was defined as the start of PD with less than four exchanges per day, 7 days a week and a peritoneal weekly Kt/V < 1.7 per week, but a total weekly Kt/V ≥ 1.7 per week. 12 All patients included in CAPD-1/2 and CAPD-3 groups met these criteria.
Generally, initial CAPD regimens consisted of 2-L dialysate. Dextrose and calcium concentrations in PD fluid as the use of icodextrin or amino acids solutions were determined accordingly the patient’s individual clinical condition. Daily exchanges were gradually increased following one of these indications: (1) total weekly Kt/V < 1.7 with initial clinical manifestations of underdialysis and (2) fluid overload despite strict salt and water control, diuretic therapy, increasing dextrose concentration of PD fluid or prescribing icodextrin 7.5% solution.
Outcomes
The composite outcome of death and transfer to HD as well as the single events death and transfer to HD were considered. All causes of patient death and transfer to HD were reported. The overall incidence rates of peritonitis and hospitalisation were expressed as episodes/patient-years dividing the number of events by the time at risk according to the ISPD 2022 guidelines. 21 In order to evaluate the velocity of RKF loss among the three groups (CAPD-1/2, CAPD-3 and CAPD-4), the means of the difference between baseline and 24 months RKF in patients with 2-year follow-up were compared. Similarly, the means of the difference between baseline and 24 months D/P, G/G0, DNa and ultrafiltration volume (UF) were compared for the purpose of investigating the change of peritoneal membrane function over time.
Statistical analysis
Normally distributed variables are presented as mean ± standard deviation, while non-parametric data are presented as median with interquartile range (IQR). Categorical variables are expressed as frequency and percentage. The parametric continuous variables were compared by the Student t-test; otherwise, the Mann–Whitney U-test was used. Fisher’s exact test for 2 × 2 contingency tables and χ 2 analysis for larger table were used to compare the nominal data. All probabilities were two-tailed, and significance level was set at 0.05 to reject the null hypothesis. Analysis of variance was used to test the difference between two more means and, when needed, Tukey’s test was used to determine the discrepancy among the three groups. Unadjusted and adjusted time-dependent Cox proportional hazards regression analyses were performed to identify the association between incremental approach of PD and patient, HD transfer, hospitalisation and peritonitis survival. The Cox analysis was performed according to ‘an intention to treat analysis’, meaning that the event allocations have been established according to the starting CAPD exchange number, even if the dose had been increased at the time of the event occurrence. All statistical analyses were performed using either JMP version 16 (SAS Institute, Cary, North Carolina, USA) or PRISM9 (GraphPad, San Diego, California, USA) software packages.
Results
Baseline data
During the study period, the number of incident PD patients at our centre was 226, of whom 17 had a follow-up <6 months, and 27 either started the dialytic treatment with an automated cycler (automated peritoneal dialysis (APD)) or changed to APD during the treatment. As a consequence, the eligible patients were 182 (Figure 1). The demographic and clinical characteristics of the 182 participants are shown in Table 1. The patients showed a mean RKF of 6.1 ± 3.6 mL/min/1.73 m2 and a mean urine output of 1184 ± 680 mL/24 h . Overall, at the initiation of PD, the prescribed peritoneal Kt/V (1.28 ± 0.55) was slightly higher than the weekly urinary Kt/V (1.16 ± 0.73) with a total Kt/V equal to 2.44 ± 0.71.
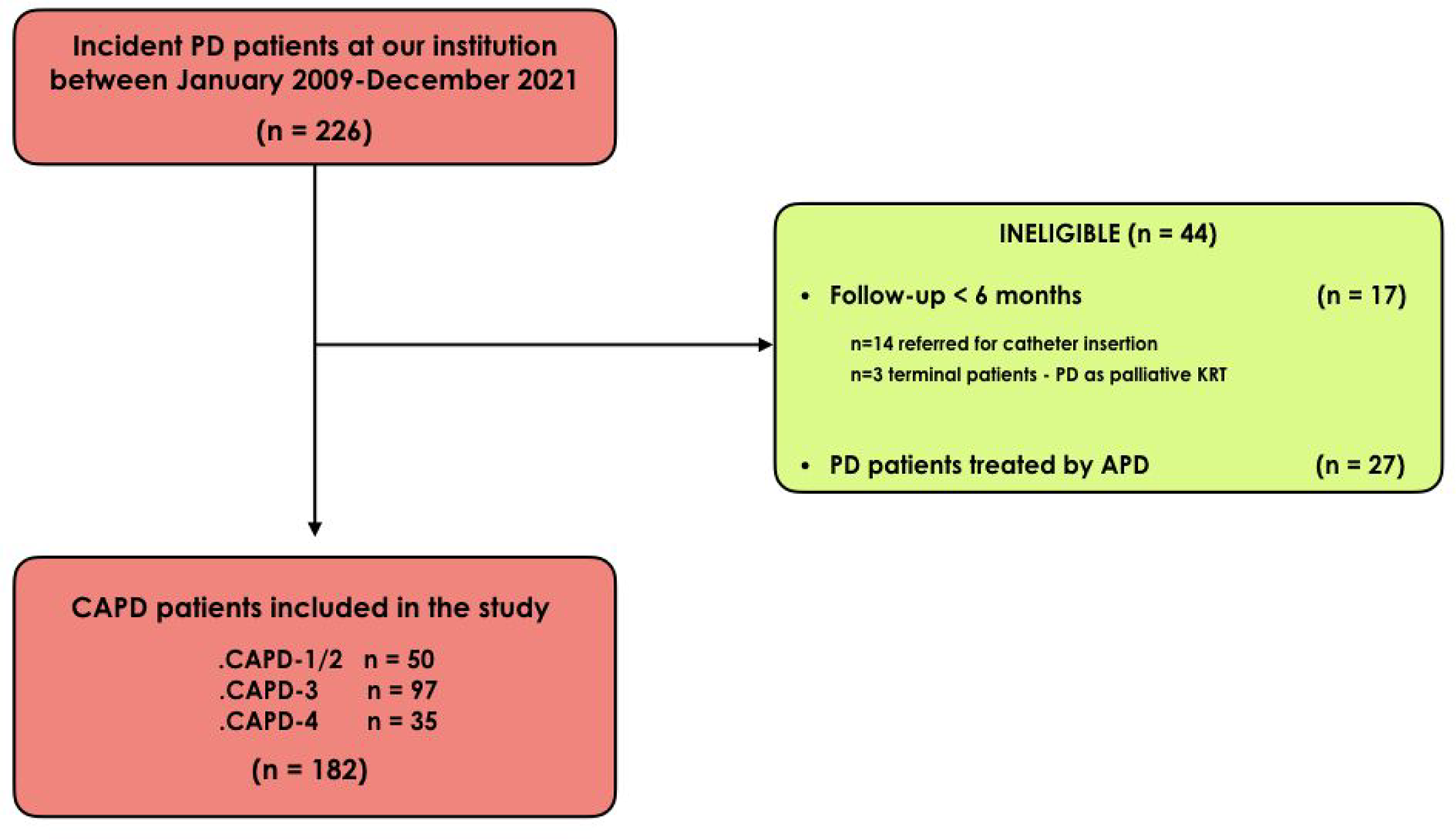
STROBE flow diagram representing the 182 eligible patients.
The three groups (CAPD-1/2, CAPD-3 and CAPD-4) had a similar age, comorbidities, gender and BMI, whereas there was a discrepancy of RKF and follow-up time. In particular, the patients who started CAPD with one or two exchanges showed a higher RKF (and hence a greater urinary Kt/V and a lower peritoneal Kt/V). No differences in term of baseline peritoneal function were observed (Table 1).
Baseline clinical characteristics of 182 patients treated by continuous ambulatory peritoneal dialysis.
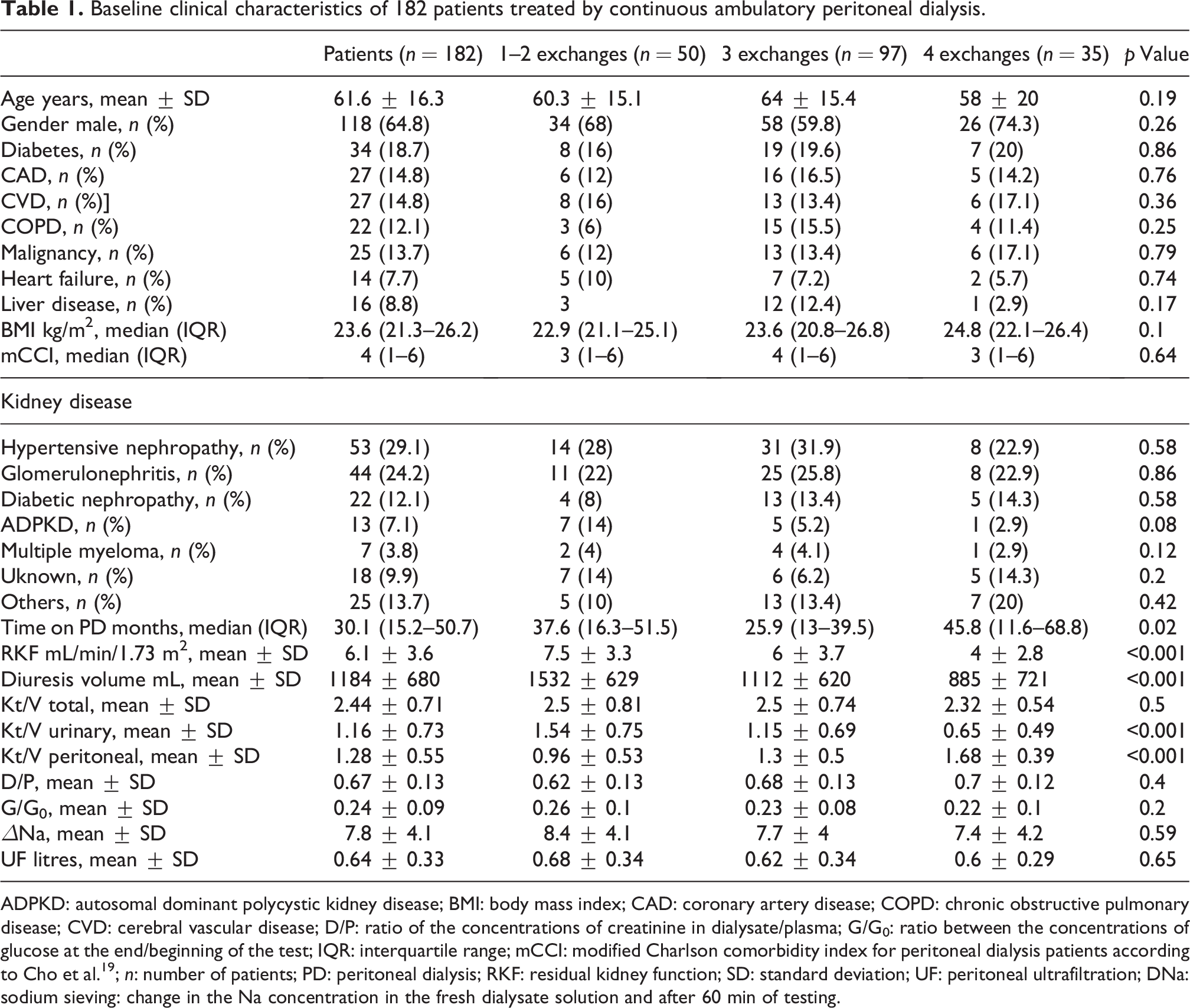
ADPKD: autosomal dominant polycystic kidney disease; BMI: body mass index; CAD: coronary artery disease; COPD: chronic obstructive pulmonary disease; CVD: cerebral vascular disease; D/P: ratio of the concentrations of creatinine in dialysate/plasma; G/G0: ratio between the concentrations of glucose at the end/beginning of the test; IQR: interquartile range; mCCI: modified Charlson comorbidity index for peritoneal dialysis patients according to Cho et al. 19 ; n: number of patients; PD: peritoneal dialysis; RKF: residual kidney function; SD: standard deviation; UF: peritoneal ultrafiltration; DNa: sodium sieving: change in the Na concentration in the fresh dialysate solution and after 60 min of testing.
Change of PD exchanges
During the study period, CAPD discontinuation occurred in 156 (85.7%) patients out of 182, while 26 subjects were still on PD at the end of the study. The number of patients who started CAPD by an incremental approach was 147 (CAPD-1/2 + CAPD-3 patients). In particular, 9 patients initiated PD with 1 daily exchange and 41 with 2 daily exchanges, while 97 started with three PD exchanges; among those, excluding patients still on PD (25) and lost at follow-up (5), 14 (11.9%) patients out of 117 were transferred from incremental to full dose before discontinuing PD. The median transition time from 1 to 2, from 2 to 3 and 3 to 4 exchanges were 5 (IQR: 2.1–13.4), 9 (IQR: 5.2–24.8) and 11.8 (IQR: 6.2–23.2) months, respectively.
Kidney function, PD dose and peritoneal membrane parameters
As expected, along with the reduction of RKF, the prescribed PD increased, while urinary clearance diminished maintaining the total Kt/V unaltered. The mean value of PD dose parameters over time is shown in the Online Supplemental Table S1.
No discrepancy of the difference of the mean values between baseline and 24 months RKF (p = 0.33) and urine output (p = 0.57) was observed among the three groups when comparing the patients with a minimum 2-year follow-up (Table S2). The rate of RKF and urinary volume loss was approximately 0.1 mL/month (1.2 mL/year) and 10–20 mL/month, respectively.
Similarly, no discrepancy of the difference of the mean of the peritoneal equilibration test values (D/P, G/G0, DNa and UF) between baseline and 24 months was registered when comparing the patients with a minimum 2-year follow-up among the three groups (Table S3). D/P value did not increase more than 0.1 during this period as well as G/G0, while DNa remained stable and UF did not drop more than 200 mL.
Patient survival and transfer to HD
During the study period, 49 patients (26.9%) died. The causes of death are listed in Figure 2(a). Univariate Cox analysis showed that age (HR: 1.07, 95% CI: 1.05–1.11, p < 0.001), diabetes (HR: 2.94, 95% CI: 1.57–5.48, p < 0.001), the burden of comorbidities (HR: 1.25, 95% CI: 1.16–1.35, p < 0.001) and 3 versus 1/2 PD starting exchanges (HR: 2.54, 95% CI: 1.1–5.8, p = 0.03) were significantly correlated with mortality (Figure 3(a)). The latter observation, however, was not confirmed by multivariate analysis (CAPD-3 vs. CAPD-1/2, HR: 2.01, 95% CI: 0.85–4.73, p = 0.11; Figure 4(a)).
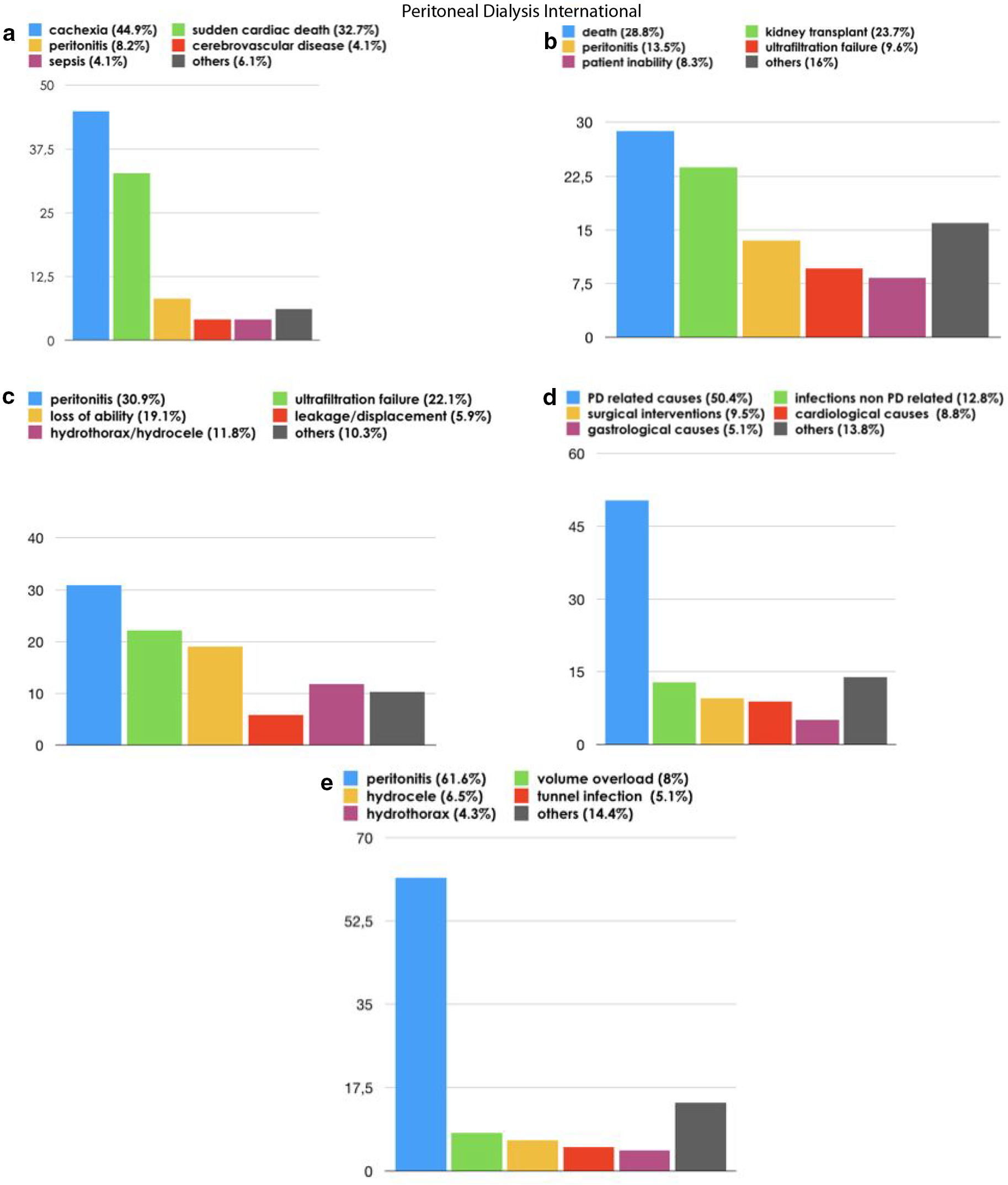
(a) Overall causes of deaths; (b) overall causes of PD discontinuation; (c) overall causes of HD transfer; (d) overall causes of hospitalisations; and (e) PD-related causes of hospitalisations in CAPD patients.
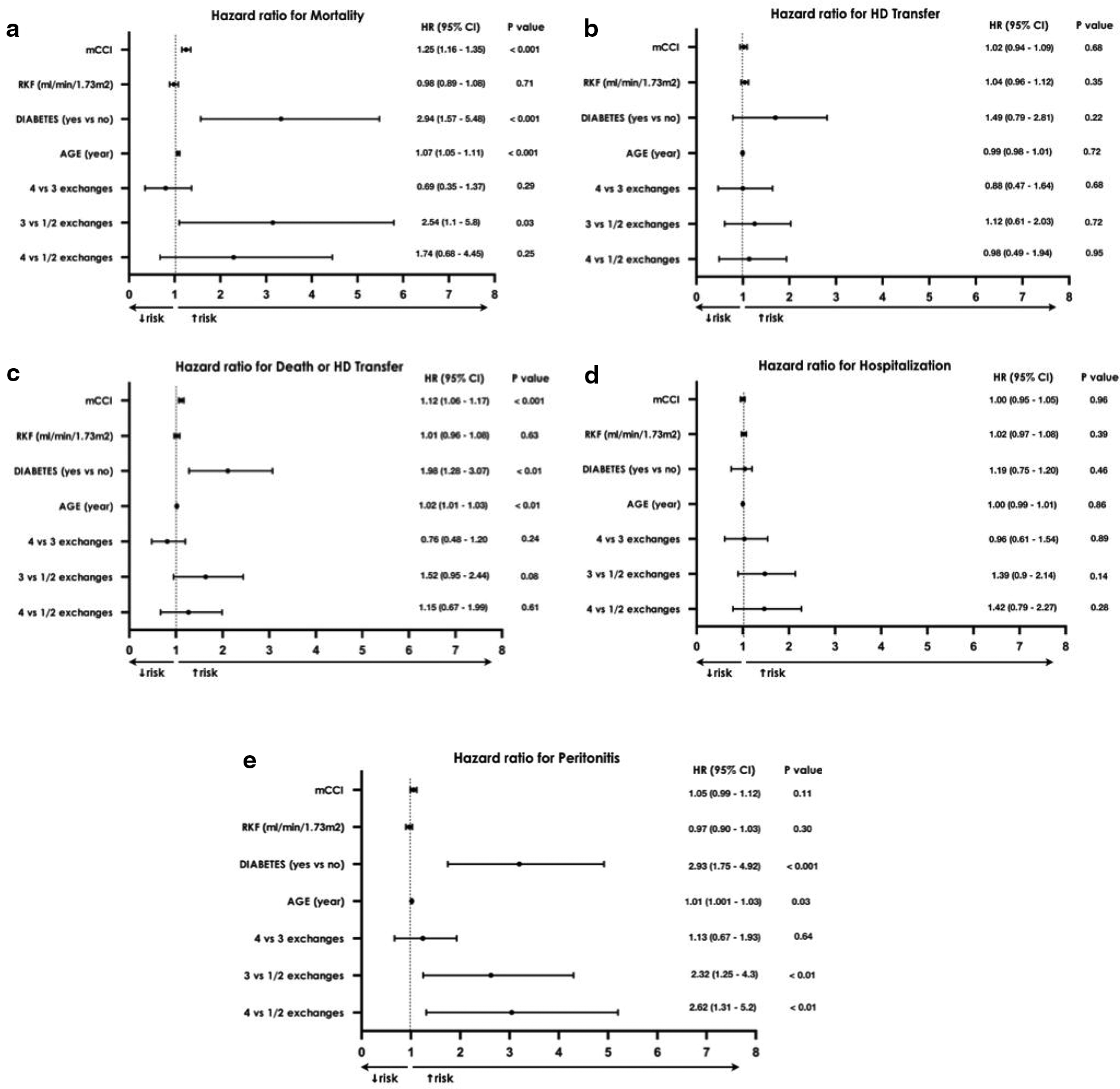
Forest plot showing univariate time-dependent Cox proportional hazards model analyses for (a) mortality, (b) HD transfer, (c) death or HD transfer, (d) hospitalisation and (e) peritonitis.
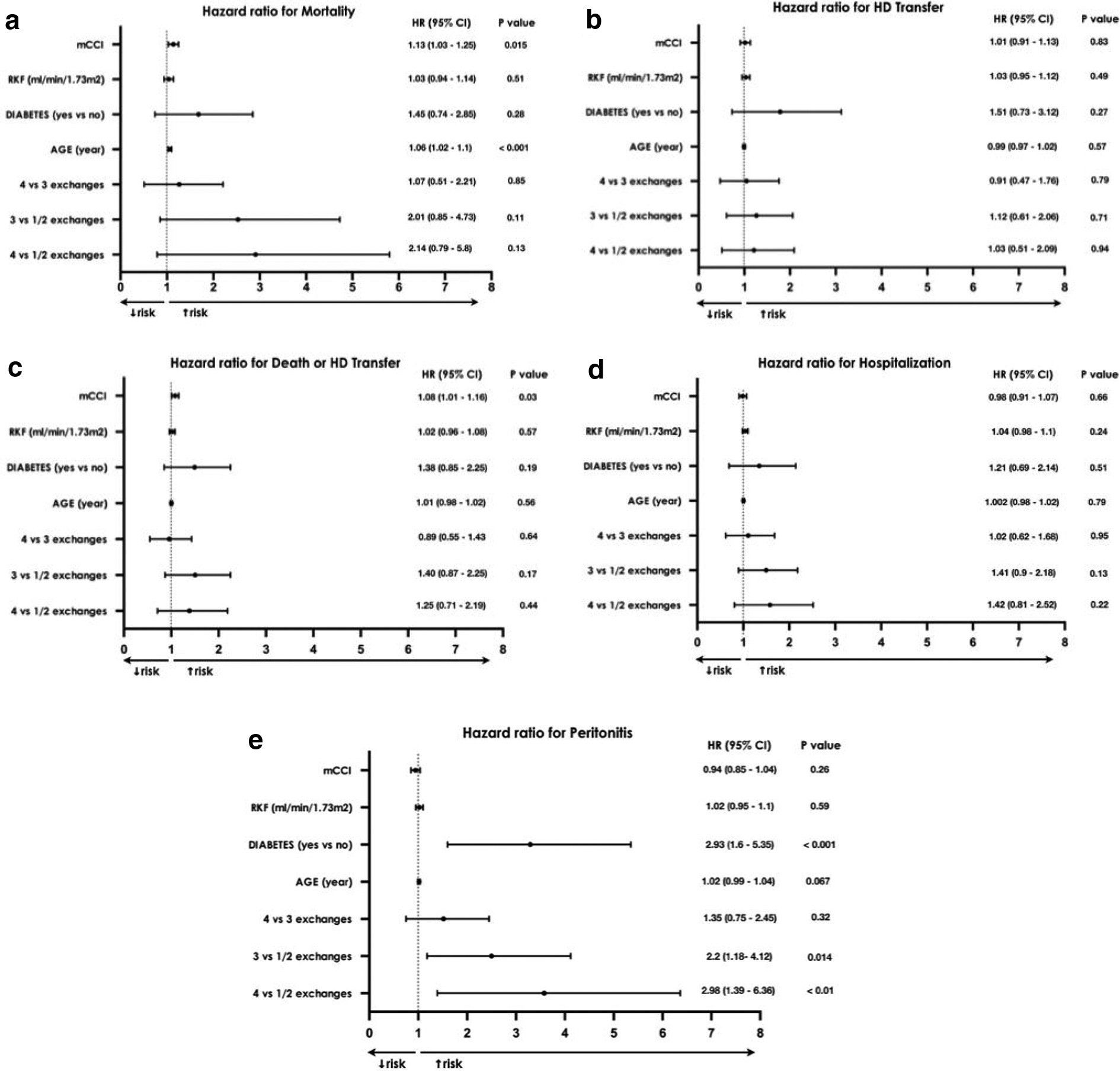
Forest plot showing multivariate time-dependent Cox proportional hazards model analyses for (a) mortality, (b) HD transfer, (c) death or HD transfer, (d) hospitalisation and (e) peritonitis.
Univariate Cox analysis did not identify any risk factor of HD transfer (Figure 3(b)) in accordance with the multivariate analysis (Figure 4(b)). During the study period, 156 patients (85.7%) discontinued the dialytic technique; among them 69 were transferred to HD. The PD drop-out and HD transfer causes are reported in Figure 2(b) and (c). Approximately 50% of PD termination causes were due to either death or kidney transplantation. The main causes of HD transfer causes were represented by peritonitis (21/68, 30.9%) and loss of peritoneal membrane ultrafiltration (15/68, 22.1%). Considering the failure events due to patient inability to perform the PD procedure independently, the comparison between CAPD-1/2 (2/50, 4%) and CAPD-4 (5/35, 14.3%) did not reach the statistical significance (p = 0.09). No difference was also observed in the percentage of HD transfers due to ultrafiltration failure (G2 8/50, 16% vs. G4 5/35, 14.2%; p = 0.83).
Considering the composite outcome of death or HD transfer, unadjusted Cox analysis identified age (HR: 1.02, 95% CI: 1.01–1.03, p < 0.01), diabetes (HR: 1.98, 95% CI: 1.28–3.07, p < 0.01) and comorbidities (HR: 1.12, 95% CI: 1.06–1.17, p < 0.001) as potential risk factors (Figure 3(c)). However, adjusted Cox analysis showed a significant correlation only with patient comorbidities (HR: 1.08, 95% CI: 1.01–1.16, p < 0.03; Figure 4(c)).
Hospitalisation and peritonitis
During a total follow-up of 524.3 patient-years, 274 admissions were recorded (0.52 episodes/patient-years) for a total of 3955 days of hospitalisation (7.5 days/patient-years) with a median single admission time of 12 days (IQR: 8–16). Hospitalisation incidence rates of CAPD-1/2, CAPD-3 and CAPD-4 were 0.41, 0.40 and 0.52 episodes/patient-years, respectively.
Even though the presence of a statistical trend, CAPD start with more than two exchanges did not reach the statistical significance as risk factor for hospitalisation in univariate Cox analysis (CAPD-3 vs. CAPD-1/2, HR: 1.39, 95% CI: 0.90–2.14, p = 0.14; CAPD-4 vs. CAPD-1/2, HR: 1.34, 95% CI: 0.79–2.27, p = 0.28; Figure 3(d)). Similarly, Cox multivariate analysis led to analogous results (CAPD-3 vs. CAPD-1/2, HR: 1.41, 95% CI: 0.90–2.18, p = 0.13; CAPD-4 vs. CAPD-1/2, HR: 1.42, 95% CI: 0.81–2.52, p = 0.22; Figure 4(d)).
Approximately 50% of the hospitalisation episodes were due to pathological events associated with PD (Figures 2(d) to (e)). Peritonitis (31%) represented the more frequent cause of hospitalisation followed by infectious episodes unrelated to the dialytic technique (12.8%).
No difference in the percentage of hospitalisation episodes due to peritonitis was observed between CAPD-1/2 and CAPD-3/CAPD-4 (CAPD-1/2 14/62, 22.6% vs. CAPD-3 50/145, 34.5%; p = 0.89; CAPD-1/2 14/62, 22.6% vs. CAPD-4 21/67, 31.3%; p = 0.26).
The overall number of peritonitis episodes was 126 with an incidence rate of 0.23 episodes/patient-years, while peritonitis incidence rates of CAPD-1/2, CAPD-3 and CAPD-4 were 0.14, 0.25 and 0.28 episodes/patient-years, respectively.
Unadjusted Cox analysis showed a higher probability of peritonitis in patients starting PD with more than two exchanges (CAPD-3 vs. CAPD-1/2, HR: 2.32, 95% CI: 1.25–4.3, p < 0.01; CAPD-4 vs. CAPD-1/2, HR: 2.62, 95% CI: 1.31–5.20, p < 0.01; Figure 3(e)). After adjusting for age, diabetes, RKF and comorbidity index, this observation was confirmed by multivariate analysis (CAPD-3 vs. CAPD-1/2, HR: 2.20, 95% CI: 1.18–4.12, p = 0.014; CAPD-4 vs. CAPD-1/2 HR: 2.98, 95% CI: 1.39–6.36, p < 0.01; Figure 4(e)).
The microbiological causes of peritonitis are reported in Table 2. Gram-positive and gram-negative bacteria accounted for 74.1% and 25.9% of peritonitis, respectively. The two most common gram-positive microorganisms were Staphylococcus species (20.7%) and Streptococcus species (19.0%), while the most common gram-negative was Escherichia coli (8.3%). The percentage of negative culture reached approximately 30%. In five cases, results of the culture were missing, hence the causative organism remained unknown. Considering the peritonitis due to either Staphylococcus and Streptococcus species, the comparison between CAPD-3 (31/75, 41.3%) and CAPD-1/2 (6/22, 27.2%) did not reach the statistical significance (p = 0.23) as well as among CAPD-4 (11/29, 37.9%) and CAPD-1/2 (p = 0.42).
Microbiological causes of the peritonitis episodes.
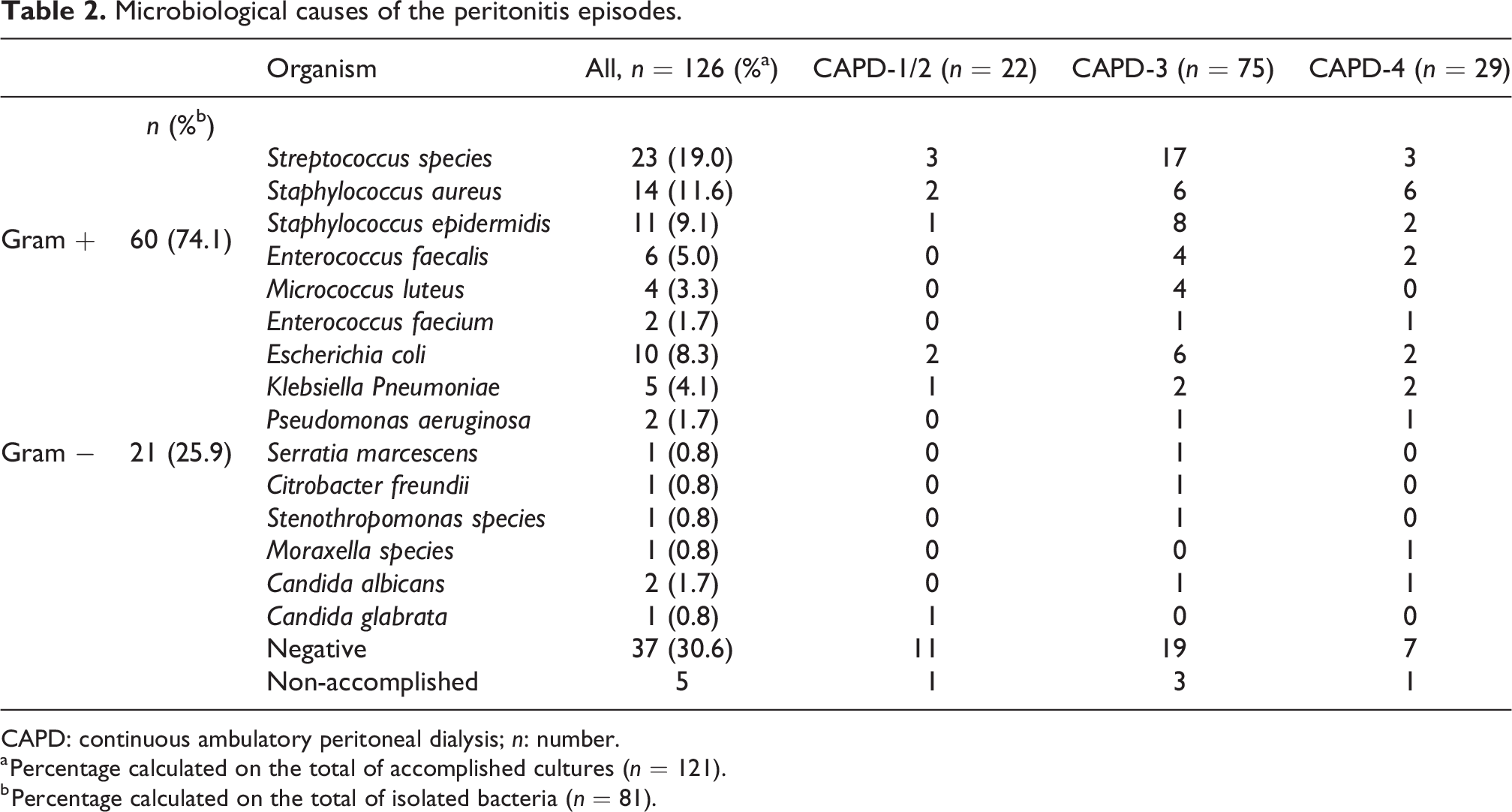
CAPD: continuous ambulatory peritoneal dialysis; n: number.
a Percentage calculated on the total of accomplished cultures (n = 121).
b Percentage calculated on the total of isolated bacteria (n = 81).
Discussion
This study evaluated several clinical outcomes dividing the PD population in three different groups according to the number of starting PD exchanges (one or two, three and four).
In our experience, less than 12% of patients who started PD with an incremental approach were transferred to a four-exchange prescription before discontinuing PD. In fact, nearly 50% of incPD patients discontinued PD due to either death or kidney transplant.
It has been claimed that starting PD with a lower rather than full dose may be associated with clinical, metabolic, environmental and economic advantages. 7 It could be theorised that accessing the peritoneum fewer times per day might decrease the likelihood of lumen catheter’s contamination and the subsequent migration of the microorganisms into the peritoneal cavity during the exchange manoeuvre. Furthermore, it has been reported that longer duration of the dry status is associated with a lower peritonitis incidence. 25
Although it was not statistically significant, a tendency towards decreased susceptibility to peritonitis was reported in a randomised controlled trial (RCT) of 139 CAPD patients followed over 2 years that compared three exchanges per day patients with four exchanges. 16 Similarly, albeit the absolute incidence was quite different (1/135 vs. 1/52 patient-months), the cumulative probability of being peritonitis-free showed no significant difference between incPD (2 exchanges per day) and standard PD (≥ 3 exchanges per day) in the study by Sandrini et al. 13 Similar results were described by Lee et al. 14 Conversely, two Asian papers reported a lower peritonitis incidence in the incPD arm. 15,26
The results of our study might partially resolve these conflicting results. Confronting one or two versus three versus four exchanges per day, we obtained that the statistical significance was reached only when one-/two-exchange group was compared with three- and four-exchange arms. Thus, we observed that the initial exchanges threshold in order to decrease the peritonitis rate might be two. Furthermore, the Kaplan–Meier curve showed that the discrepancy in term of peritonitis-free survival among the three groups occurred during the first 12 months (Online Supplemental Figure S1), while the percentage drop remained quite stable for the following period. This observation strengthens the hypothesis that the first year of PD represents the most vulnerable period due to the lack of patient experience in performing CAPD manoeuvres. To further corroborate this hypothesis, we compared the percentage of peritonitis caused by Staphylococcus and Streptococcus species that are mainly involved in either touch or nasal contamination. The results showed a tendency towards a higher probability of these infectious episodes in CAPD-3 (41.3%) and CAPD-4 (37.9%) groups in comparison to CAPD-1/2 (27.2%). The statistical significance could have not been reached due to the relatively small sample size. Thus, starting PD by a lower number of daily exchanges might decrease the peritonitis rates minimising the probability of infection when the risk is the highest, but additional studies are needed to further elucidate this hypothesis.
Locally, the exposure to a high glucose concentration in PD solution has detrimental effects on the structure and function of the peritoneal membrane resulting ultimately in neoangiogenesis, mesothelial cell death and progressive fibrosis. 27 –32 Thus, by minimising glucose exposure, incPD may prolong the overall longevity of the peritoneal membrane and reduce late-onset HD transfer due to membrane failure.
However, we did not observe lower HD transfer episodes due to ultrafiltration failure when comparing CAPD-1/2 with CAPD-4. As reported by Yan and Lee, 14,16 we did not identify a technique survival advantage in incPD groups in comparison to full dose.
An incremental approach may also lessen the care burden and allow patients together with their families to gradually adjust to the changes in lifestyle and responsibility that result from dialysis treatment. Although it was not statistically significant, a tendency towards decreased susceptibility to PD discontinuation because of patient inability to perform autonomously PD manoeuvre was found in patients starting with one- or two-exchange CAPD.
Frequency and duration of dialysis and intradialytic hypotension have been associated with loss of RKF in patients on HD, 33 with observational study outcomes revealing better RKF preservation through incremental HD. 34,35 Consequently, it has been hypothesised that incPD might help preserve RKF in comparison with full-dose PD. 13,14
An Italian study compared two groups with comparable RKF that started either with 1/2 or more than 2 daily PD exchanges (29 and 76 patients, respectively) observing at the end of the follow-up, a higher RKF in first group. 13 Similarly, an Asian paper reported a reduced risk of anuria in a group of patients initiating CAPD by a PD regimen of one to two exchanges in comparison with three to four exchanges per day. 14 Albeit underpowered, the only RCT on incremental versus full-dose PD considering as primary outcomes the decline of glomerular filtration rate and anuria-free survival failed to show a significant discrepancy between the two groups after a follow-up period of 24 months. 16
We observed a slow loss of kidney function (approximately 1.2 mL/year) that allowed to maintain most of the patients in incPD. Since the baseline RKF was different among the three groups, the means of the difference between baseline and 24 months RKF in patients with at least 2-year follow-up were compared. In this evaluation, we did not identify a slower RKF decrease in any incPD groups (CAPD-1/2 or CAPD-3).
In accordance with the previous studies, 13 –16,26 an inferiority in term of mortality in the incPD groups was not observed. In the multivariate analysis after adjusting for several factors, one- or two-exchanges PD start showed a trend towards decreased mortality although it was not statistically significant.
The main limitation of the study is probably related to its sample size that was not adequately powered to evaluate part of the outcomes examined. In addition, its generalisability to other countries with different PD practices, population and ethnicity backgrounds is limited due to its single-centre design and exclusive inclusion of CAPD patients. Further limitations are represented by its retrospective nature and the clinician variability regarding the starting CAPD prescription; for these reasons, the possibility of indication bias with residual confounding could not be completely excluded.
However, the comprehensive data collection was performed trough the support of an electronic database. Furthermore, the paper includes long-term follow-up of a relatively large and unselected CAPD cohort. In addition, this is the first study that compared three CAPD groups according to the number of starting PD exchanges.
In conclusion, our study might support the evidence that incremental approach is not inferior to full-dose PD while providing several advantages. 7 Furthermore, a one- or two-exchange CAPD start could be associated with a lower risk of peritonitis, particularly during the first months of the dialytic treatment. However, a well-powered and long-term RCT is required to confirm these data and to explore potential incPD advantages in term of hospitalisation and HD transfer rate as well as patient survival in comparison to full-dose PD.
Supplemental material
Supplemental Material, sj-docx-1-ptd-10.1177_08968608231209849 - Relationship between number of daily exchanges at CAPD start with clinical outcomes
Supplemental Material, sj-docx-1-ptd-10.1177_08968608231209849 for Relationship between number of daily exchanges at CAPD start with clinical outcomes by Luca Nardelli, Antonio Scalamogna, Elisa Cicero, Federica Tripodi, Simone Vettoretti, Carlo Alfieri and Giuseppe Castellano in Peritoneal Dialysis International
Footnotes
Acknowledgements
None.
Authorship contributions
Research idea and study design: LN and AS; data acquisition: LN, EC and FT; data analysis/interpretation: LN and AS; statistical analysis: LN; supervision or mentorship: CA, SV and GC. Each author contributed important intellectual content during manuscript drafting or revision and accepts accountability for the overall work by ensuring that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not required (retrospective cohort study undertaken through a case note review).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent to participate
Not required.
Informed consent to publish
No doubt that anonymity can be maintained.
Trial registration
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.