
Abstract
Thyrotoxic periodic paralysis (TPP) is a potentially lethal complication of hyperthyroidism characterized by recurrent muscle weakness and hypokalemia. It has been commonly reported in non-Asian populations. Four cases were reported in Saudis so far, and one had a life-threatening arrhythmia. We describe an additional case of a 28-year-old apparently healthy Saudi male patient, who presented with acute paraparesis associated with hypokalemia (K: 2.0 mmol/L), complicated by ventricular tachycardia and cardiac arrest. He was successfully resuscitated and his hypokalemia was corrected. A diagnosis of Graves’ disease associated with TPP was made. He was initially treated with carbimazole and β-blockers and then given a definitive therapy with radioactive iodine, which showed a good response. This case highlights the importance of early recognition and prompt treatment of TPP as a differential diagnosis for muscle weakness. A brief review of TPP and associated arrhythmia is included.
Keywords
Case Report
A 28-year-old Saudi male patient was presented in the emergency room of King Salman Hospital in Riyadh, Saudi Arabia, with acute bilateral proximal weakness of lower limbs followed immediately by a presyncopal attack. The patient's vitals on presentation were Heart Rate (HR) = 107/minute, Blood Pressure (BP) = 118/74 mmHg, Respiratory Rate (RR) = 19/minute, and body temperature = 37.5 °C. The patient's Body Mass Index (BMI) was 28.7 kg/m2, and he had 97% oxygen saturation on room air. The ECG revealed a wide complex tachycardia (Fig. 1), and his serum potassium level was 2.0 mmol/L. The patient was treated according to an advanced cardiac life support protocol for ventricular tachycardia (VT) with cardioversion followed by amiodarone infusion as well as correction of hypokalemia. His lower limb weakness and VT were resolved after correction of hypokalemia. He was then transferred to the cardiac unit of King Fahad Medical City in Riyadh for further investigations and management.

ECG at the time of presyncopal attack (29 hours after admission).
The patient had a two-month history of intermittent palpitations and diarrhea and lost
Investigations showed 3.6 mmol/L of serum potassium (after replacement), 39.7 pmol/L of serum-free thyroxine (T4), ≤0.005 mIU/L of serum TSH, and positive TSH receptor antibodies (Table 1). ECG (Fig. 2) showed normal sinus rhythm and narrow QRS complex. Random blood sugar was 112 mg/ dL and HbA1c was 5.6%. A 24-hour Holter ECG monitoring during his stay revealed no arrhythmias. Left ventricular size and function were normal on transthoracic echocardiography. Thyroid ultrasound confirmed the finding of diffuse thyroid enlargement with heterogeneous echoes. Thyroid scintigraphy using TC-99m showed diffuse enhancement of the enlarged thyroid gland bilaterally (Fig. 3). The diagnosis of thyrotoxic periodic paralysis (TPP) due to Graves’ disease was made, and the patient was started on carbimazole and continued on bisoprolol as provided by the referring hospital. He showed significant improvement with no further episodes of paralysis or arrhythmia. He was discharged home in a stable condition on carbimazole and bisoprolol only. Four months later, he elected to receive radioactive iodine (RAI) as a definitive therapy. A dose of 13.5 mCi of RAI was given as an outpatient treatment with good response. Currently, he is in a post-RAI ablation hypothyroid state and on levothyroxine replacement with regular follow-up. No further episodes of TPP were noted, and the potassium levels remained normal without supplements. The patient was then seen by a dietitian during the follow-ups.
Laboratory investigations.


ECG upon arrival at King Fahad Medical City (four days after cardioversion).
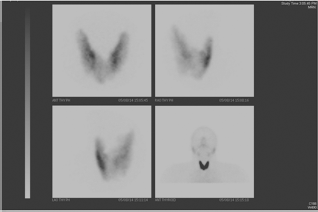
Thyroid scintigraphy.
Discussion
TPP is an uncommon but potentially lethal manifestation of thyrotoxicosis. 1 It is the most common cause of acquired hypokalemic periodic paralysis. 2 It is well known that East Asian populations are affected more frequently than other ethnicities, with an incidence of 2% as compared to 0.1–0.2% in Western populations. Although hyperthyroidism is more common in female patients, TPP affects male patients more frequently with an incidence of 8.7–13% and a male:female ratio of 20:1. Currently, TPP has been increasingly reported in other populations also. A review of 67 case reports published from 1996 to 2005 (24 Asians and 43 non-Asians) suggested that TPP is no longer restricted to non-Asian populations.3,4
Few cases had been reported among Arab population. To the best of our knowledge, only four cases have been reported in the Saudi population, with one case complicated by a life-threatening arrhythmia. 5 This is the fifth case of TPP and the second case that has been complicated by life-threatening arrhythmia among Saudis.
Although the pathogenesis of TPP remains unclear, it is well established that high circulating levels of thyroid hormones in hyperthyroidism increases the Na+/K+/ATPase activity and the subsequent influx of potassium into the intracellular compartment, thereby leading to hypokalemia. Hyperthyroidism is also associated with increased adrenergic response, which in turn increases the Na+/K+/ATPase activity. This might explain the good response to nonselective β-blockers during acute attacks of TPP. Androgens were reported to increase the activity and expression of Na+/K+/ATPase, which might explain the predilection of this condition for males. 6 In addition, insulin has been found to activate the Na+/K+/ATPase pump causing an influx of potassium into cells. Therefore, anything that promotes hyperinsulinemia, such as high-carbohydrate meals, can trigger or exacerbate TPP. 7 A recent study indicates that the loss of function of the skeletal muscle-specific potassium channel Kir2.6 may contribute to this disorder. 8
The hallmark clinical feature of TPP is recurrent, acute, and reversible attacks of symmetrical proximal muscle weakness that affects mostly the lower extremities than upper extremities due to hypokalemia in the setting of thyrotoxicosis. Prodromal symptoms of muscle aches, cramps, and stiffness might occur. Sensations and consciousness are not affected. Deep tendon reflexes are decreased or absent, but might be brisk. Ocular, bulbar, and respiratory muscles are usually, but not always, spared.5,9,10 The age of onset is usually between 20 and 40 years in ∼80% of patients. The attacks tend to occur in the early morning during summer and fall, which can be attributed to the increased outdoor activity and ingestion of sugar-containing cold beverages, 2 and usually last for 3–36 hours. 10 TPP is triggered by various factors, most commonly high-carbohydrate meals and strenuous exercise. Other events that can induce attacks include trauma, stress, infections, alcohol, and medications (eg, insulin, acetazolamide, and corticosteroids). 2
Patients with TPP have clinical findings of hyperthyroidism. However, these findings are usually subtle to undetectable that makes TPP often overlooked as a cause of periodic paralysis. Around 17% of TPP patients manifest overt hyperthyroidism, and one-third of them have known personal or family history of hyperthyroidism. 2 Clues to diagnosis include warm and moist skin, fever, tachycardia with a wide pulse pressure, and goiter. Tachycardia has been reported to be the most sensitive indicator of TPP than the other classic signs of hyperthyroidism. 10 Graves’ disease is the most common cause of hyperthyroidism that is associated with TPP. However, it has been reported to be associated with thyrotoxicosis of any cause, such as toxic adenoma, toxic multinodular goiter, subacute thyroiditis, T3-containing weight-reducing agents, 2 painless thyroiditis, TSH-secreting pituitary adenoma, amiodarone-induced thyrotoxicosis, inadvertent iodine excess, 11 and over-replaced hypothyroidism. 12 Thorough clinical assessment is crucial to differentiate periodic paralysis from other causes of acute quadriparesis, such as myasthenic crisis, acute myelopathy, and Guillain–Barré syndrome.6,7 Hypokalemia is the hallmark of periodic paralysis. The possibility of thyrotoxicosis must always be evaluated in the setting of periodic paralysis to distinguish TPP from familial hypokalemic periodic paralysis (FHPP). Both disorders are similar in their clinical features, but TPP is rarely associated with a positive family history and has a later onset of presentation than FHPP. 1 However, some reports have shown that TPP might be the initial presentation of thyrotoxicosis. 8 On average, the patient will experience 2.8 episodes before the diagnosis is made. 4 Workups are directed in identifying the underlying etiology of thyrotoxicosis as the definitive treatment is to achieve euthyroid state, which is a cure for TPP. Thyrotoxicosis patients usually have hyperdefecation and increased bowel frequency, sometimes diarrhea and rarely steatorrhea.
Laboratory investigations during paralytic episodes usually reveal hypokalemia (≤3.0 mmol/L), low urinary potassium excretion, elevated free T4 (often mild), and suppressed TSH. Hypophosphatemia and hypomagnesemia might be observed, which are also due to the intracellular shift. The severity of the attack and its complications (including arrhythmias) correlates with the degree of hypokalemia, but not with the clinical or biochemical severity of thyrotoxicosis. 2 An ECG may show characteristic features of hypokalemia, which include increased amplitude of P waves, widening of QRS complexes, prolonged PR and QT intervals, and appearance of U waves. 6 Unlike hypokalemia from other causes, sinus tachycardia predominates in TPP patients. Arrhythmias may be detected as well. 9
Cardiac arrhythmias associated with thyrotoxicosis are usually supraventricular. However, ventricular arrhythmias had been reported to be associated with thyrotoxicosis, which tend to occur in patients with intrinsic cardiac disease. 13 In cases of TPP, a combination of hyperthyroidism and hypokalemia may potentially result in a wide variety of cardiac arrhythmias in patients with or without intrinsic cardiac disease. 5 Various AV and right bundle branch blocks, VT, ventricular fibrillation, and cardiac arrest have been reported. 4 Hypokalemia is the classical and most important precipitating factor and is usually associated with a unique form of VT, known as torsades de pointes (twisted point) or polymorphic VT. Other triggers include heart failure, acute myocardial infarction, drug toxicity, and alcohol consumption. 14
Hemodynamically unstable VT is a life-threatening condition that may persist and degenerate into ventricular fibrillation, which will lead to sudden death in the absence of prompt treatment. Immediate defibrillation is the treatment of choice despite the underlying etiology. Further therapy is required to treat the underlying disorders and prevent recurrences. 14 While attempting to elucidate the underlying cause of arrhythmia for the targeted treatment, current guidelines for the management of hemodynamically stable VT advocate revascularization and beta blockade in addition to initiating treatment with amiodarone or procainamide. 15
After stabilization of the general condition, the management of TPP consists of treating the acute paralytic attacks and treating the underlying cause of thyrotoxicosis. Although acute attacks of TPP might recover spontaneously, potassium supplementation, whether oral or IV depending on the patient's status, is recommended to hasten muscle recovery and prevent cardiopulmonary complications. However, potassium is released from muscles into the extracellular space upon recovery, leading to rebound hyperkalemia, which has been reported to occur in ∼40–70% of cases and might lead to fatal arrhythmias. Therefore, potassium supplementation should be given cautiously at a low rate (≤10 mmol/hour or even a total dose of ≤50 mmoL), with frequent monitoring of serum potassium and continuous cardiac monitoring, unless the patient has complications of hypokalemia, such as arrhythmia.10,16,17 Potassium supplementation should be further slowed or stopped with evidence of raising plasma K or resolution of ECG changes, which might be an early sign of subsiding TPP due to the high sensitivity of cardiac muscle to the plasma K concentration. 18 Potassium supplementation is not useful for prevention against further paralytic attacks; therefore, it should not be given between attacks. 3 Nonselective β-blockers, such as propranolol, can be given as an alternative option to treat acute attacks. 10 Propranolol acts by blunting the hyperadrenergic stimulation of the Na-K-ATPase pump that has been implicated in the pathogenesis of TPP. 19 It has been reported that some cases of TPP were reversed rapidly with a high dose of oral propranolol (3–4 mg/kg) alone and without developing rebound hyperkalemia. 12 However, more modest doses of oral β-blockers, such as 20–40 mg of propranolol, three to four times a day, are considered to be effective. Further (controlled) studies are needed to document the effectiveness of β-blockers alone or in combination with potassium as therapeutic options for acute attacks of TPP. 19
The definitive treatment of TPP is to achieve euthyroidism that completely abolishes the attacks of TPP. Management of hyperthyroidism should be individualized according to the underlying cause. 10 Initial treatment with β-blockers and antithyroid medications shows improvement, but hyperthyroidism and paralytic episodes may recur if antithyroid medications are discontinued, and the underlying cause of thyrotoxicosis persists, especially in patients with Graves’ disease. 11 Both RAI therapy and thyroidectomy are effective options for hyperthyroidism and should be discussed with the patient. 12 In the absence of contraindications, RAI is the definitive treatment for patients with Graves’ disease, toxic MNG, or toxic adenomas.6,10 However, it takes a couple of weeks to achieve euthyroidism. Thus, the use of nonselective β-blockers and avoidance of any precipitating factors are important during early treatment with antithyroid drugs or after RAI therapy to prevent the recurrence of attacks that might occur while waiting for a euthyroid state to be achieved. 3 Carbonic anhydrase inhibitors such as acetazolamide, which is used to decrease the frequency of paralytic attacks in FHPP, should never be used in patients with TPP as it may actually precipitate or worsen the attacks. 11 Caution should be exercised upon the use of dextrose infusion and/or β-adrenergic agent in patients with cardiac arrhythmias associated with hypokalemia.20,21
Our patient presented with an acute attack of TPP that has been complicated by a near-fatal ventricular arrhythmia as an initial presentation of Graves’ disease. He responded very well to RAI as a definitive therapy and did not have further attacks. However, he is in a post-RAI hypothyroid state for which he is on levothyroxine replacement therapy.
In conclusion, we report the second case of TPP presenting as Graves’ disease with nonfatal ventricular arrhythmia, which has been increasingly reported in the non-Asian population, and can be associated with any cause of hyperthyroidism in an Arab population. It can present with life-threatening arrhythmias due to severe hypokalemia, which emphasizes the importance of early recognition and prompt treatment. Thus, TPP should be included in the differential diagnosis of acute muscle weakness associated with hypokalemia. However, a high clinical index of suspicion is needed as the clinical features of hyperthyroidism are subtle. The goals of management should be to cautiously correct hypokalemia to prevent cardiopulmonary complications and to achieve euthyroidism.
Author Contributions
Provided clinical care: MMA, NAJ. Analyzed the data: OH, MMA, NAJ. Wrote the first draft of the manuscript: OH. Contributed to the writing of the manuscript: MMA. Agree with manuscript results and conclusions: NAJ. Jointly developed the structure and arguments for the paper: OH, MMA. Made critical revisions and approved final version: MMA, NAJ. All authors reviewed and approved of the final manuscript.