
Abstract
Mycosis fungoides (MF), also known as Alibert-Bazin syndrome or granuloma fungoides, is the most common form of cutaneous T-cell lymphoma. Cutaneous lymphomas are an uncommon, heterogeneous group of non-Hodgkin lymphomas (NHLs) of T- and B-cell origin where the skin is the primary organ of involvement. This is a case of a 60-year-old Nigerian woman, who was diagnosed and managed as a case of chronic dermatitis but further investigations confirmed a diagnosis of MF; she was thereafter managed with topical glucocorticoids/chemotherapy and improved on these treatments. We make a plea for better awareness of the disease among physicians and pathologists in Africa.
Background
The first clinical description of mycosis fungoides (MF) was made in 1806 by Baron Jean-Louis Alibert, a French physician, who identified a 56-year-old man with skin tumors resembling mushrooms after having a desquamating rash over several months. 1
In 1975, Lutzner, Edelson, and associates introduced the term cutaneous T-cell lymphoma (CTCL) to describe the spectrum of skin-based lymphomas of T-cell origin, including classic MF and Sézary syndrome (SS). 2
MF is twice as common in males as in females. The median age at diagnosis is 55 years. 3 Blacks are almost twice as likely to develop MF compared to whites and Asians. The etiology of MF remains unknown, but genetic, environmental, and infectious agents, eg, human T-cell leukemia virus 1 (HTLV-1) infection, have been implicated as possible factors triggering lymphocyte activation or transformation.4,5
A hypothesis of “persistent antigen stimulation” as an initial event has been proposed after MF was observed to be a disease of mature CD4+ memory cells, but the antigen is not known. MF may also be viewed as a disease of immune deregulation. Tumor progression is associated with decreased antigen-specific T cell responses and impaired cell-mediated cytotoxicity. 6
MF is difficult to diagnose in its early stages because the symptoms and skin biopsy findings are similar to those of other skin conditions. 7
Case Report
A 60-year-old female farmer presented at the hematology clinic on account of generalized body itching for 3 years and mild hypoanesthesia of the skin for 5 years. There were mixed hypopigmented and hyperpigmented maculopapular scaly patches in her back and both upper limbs.
There was no history of arthralgia, radiation, or chemical exposure, no swellings in any part of her body, and no bleeding into her skin or from any orifice. Patient neither took any form of alcohol nor tobacco products. Patient had presented at the dermatology clinic earlier where she was investigated for various conditions including leprosy. She was, however, being treated for chronic dermatitis prior to presentation at the hematology clinic. Investigations carried out at the hematology clinic included full blood count, peripheral blood film, chest X-ray, abdomino-pelvic ultrasound scan, and renal and liver function tests, and all were normal. Viral screens for HIV I & II, Hepatitis B surface Ag, and Hepatitis C virus antibodies were also negative. Multiple skin biopsy samples taken from her back were sent for histology at St. John's Institute of Dermatology, St. Thomas' Hospital, London, which revealed appearances diagnostic of cutaneous T-cell lymphoma (MF). She was diagnosed in the early stages, stage 1B (T2 N0 M0 B0) according to the modified tumor-node-metastasis-blood (TNMB) classification.
Patient was placed on topical glucocorticoids and commenced on eight courses of IV cyclophosphamide 750 mg/m2, IV epirubicin 25 mg/m2, and prednisolone tablets 40 mg/m2 daily for 5 days. Each course was given in 21-day intervals.
She completed all courses of chemotherapy and did well, evidenced by disappearance of her symptoms except the dyspigmentation on the skin which is still resolving.
Discussion
MF is the most common cutaneous lymphoma. 1 It is a relatively rare, extra nodal, non-Hodgkin's lymphoma with a stable incidence of approximately 0.36 per 100,000 personyears. 8 It most often presents in those aged 45 to 60 years but has been diagnosed in children and adolescents. 9 It is 50% more common in black than in white patients and twice as frequent in men as in women.
MF is classically divided according to its clinical presentation as patches, plaques, or tumors. 10 Our patient had mixed hypopigmented and hyperpigmented maculopapular scaly patches in her back and both upper limbs. The patch or plaque lesions of MF have a predilection for non–sun-exposed areas (eg, the buttocks, medial thighs, back, and breasts), although any area of the skin may be affected. 11 It is most often mis-diagnosed as chronic contact dermatitis, atopic dermatitis, or psoriasis especially in the early stages. 11 Patches and plaques may show hypopigmentation or hyperpigmentation, atrophy, and petechiae.11,12
The median ages of presentation of MF of 55 years reported by Weinstock and Reynes 3 and 45–60 years reported by Morales-Suárez-Varela 9 are similar to the patient's age of 60 years who has had a 5-year history of generalized body itching, dyspigmentation of the skin, and scaly patches before presentation.
Two main hypotheses have been recognized in the pathogenesis of MF. The antigenic-stimulation hypothesis suggests that MF is caused by antigen persistence. Continuous stimulation of T cells leads to initial chronic inflammation, which in turn leads to the development of a malignant T-cell clone.
13
A potential source is occupational exposure to certain substances in glass formers, pottery and ceramics workers,
9
with an increased risk in the paper processing industry.9,14 Bacterial superantigens, such as
The diagnosis is difficult especially in the early stages but it is made through a combination of the clinical picture and examination, and is confirmed by a skin biopsy and staged appropriately based on the results.
She was diagnosed in the early stages, stage 1B (T2 N0 M0 B0) according to the modified TNMB classification, originally adopted by the Mycosis Fungoides Cooperative Study Group (Table 1).10,22,23
Modified International Society for Cutaneous Lymphomas/European Organization for Research and Treatment of Cancer revisions to the TNMB classification of MF/Sézary syndrome.

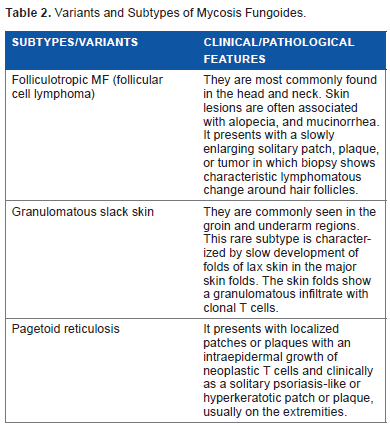
The histological parameters suggesting the diagnosis in early stages of MF include epidermotropism (lymphocytes disposed as solitary units within the basal layer of the epidermis in foci), dermal fibrosis and atypia of dermal lymphocytes, Pautrier's microabscesses, basal alignment of neoplastic lymphocytes, hyperconvoluted dermal and epidermal lymphocytes, and grandiosity sign (size of lymphocytes becoming larger as they migrate toward granular layer of epidermis).24–27 The patient's histology report revealed prominent exocytosis of the lymphocytes with cytological atypia. The cells are irregular and convolute infiltrating mainly the basal cell layer of the epidermis. At the superficial to mid-dermis, there were mild to moderately prominent perivascular and interstitial cell infiltrates consisting of round lymphocytes, histiocytes, and atypical lymphoid cells. These findings are similar to standard histologic criteria. There are various variants/subtypes of MF that follow similar clinical and pathological features and some distinctive characteristics. These are given in Table 2.
Variants and Subtypes of Mycosis Fungoides.
Variability in the clinical presentation and progression of MF makes multiple therapeutic options available, although its management is complex and there are no simple treatment algorithms;28,29 skin-directed therapies that include topical corticosteroids, nitrogen mustard, carmustine, local or total body radiation therapy, topical bexarotene, and phototherapy have been shown to give good response in early stage MF. 30 However, systemic chemotherapy or targeted therapy with a monoclonal antibody, oral retinoids, recombinant interferon alpha, and fusion toxins are used in more advanced stages.31,32
Current areas of interest in clinical trials for MF confined to the skin include combined modality therapies containing both topical and systemic agents.33,34 The patient was managed with a combined therapy of topical glucocorticoids, systemic chemotherapy (adriamycin and cyclophosphamide), and oral prednisolone of eight courses every 21 days, which the patient responded to favorably. Systemic chemotherapy used in advanced stages of MF was instituted because of poor response to topical glucocorticoids alone and unavailability of phototherapy in our centre.
The patient completed eight courses of systemic chemotherapy 6 months ago and is on topical glucocorticoids. She is presently symptom free and is being seen on a 3 monthly basis in the hematology clinic.
MF is incurable, but many patients experience prolonged periods of disease control. Quality of life is a major objective, in addition to cure, and maximizing periods of remission or stable disease and minimizing treatments and toxicities are two central concerns in clinical care. Treatment, therefore, is considered palliative for most patients, though major symptomatic improvement is regularly achieved.
Author Contributions
Conceived the concept: AA Akinbami. Wrote the first draft of the manuscript: BIO. Contributed to the writing of the manuscript: SOJ-O. Agree with manuscript results and conclusion: AA Adediran, EIU, AOD. Jointly developed the structure and arguments for the paper: O Osinaike, AKI. Made critical revisions and approved final version: MO, AD, O Okunoye. All authors reviewed and approved of the final manuscript.