
Abstract
Introduction
Vernix caseosa peritonitis (VCP) is a very unusual complication caused by inflammatory response to amniotic fluid spilled into the maternal peritoneal cavity. Twenty-seven cases have been reported, and all occurred after cesarean section.
Case presentation
We present a case of VCP following vaginal delivery; this may be the first case reported after vaginal delivery. Mrs. A, 28 years old, gravida 3, para 2, with one previous cesarean section, was admitted at 41 weeks gestation in active labor. Vacuum extraction was performed to deliver a healthy male baby, 4.410 kg, Apgar scores 7, 8. She developed fever, acute abdominal pain, and distension about 3 hours after delivery. A diagnosis of acute abdomen was made. Laparotomy was performed and it revealed neither uterine scar rupture nor other surgical emergencies, but 500 mL of turbid fluid and some cheesy material on the serosal surface of all viscera. Biopsies were taken. She had a course of antibiotics and her recovery was complete. Histology of the peritoneal fluid and tissue biopsy resulted in a diagnosis of VCP.
Conclusion
Clinical diagnosis of peritonitis due to vernix caseosa should be considered in patients presenting postpartum with an acute abdomen after vaginal delivery.
Introduction
Vernix caseosa peritonitis (VCP) is a very unusual complication caused by inflammatory response to amniotic fluid spilled into the maternal peritoneal cavity; only 27 cases of this entity have been reported in literature. 13 All the cases reported occurred after cesarean section.1–18 The previous publications in this field were identified by PubMed Search using the search words “vernix”, “caseosa”, “peritonitis”, “diagnosis”, and “management.” Only three cases have been reported, which had their onset of symptoms from the antenatal period.7,11 The other cases were diagnosed in the postpartum period after uneventful cesarean section. A recent case of VCP that occurred 5 weeks after cesarean section, the longest period for such a presentation so far, has been reported. 15
A vernix caseosa spill into the peritoneal cavity is thought to incite an inflammatory reaction, causing symptoms resembling an acute abdomen. Even though spillage of amniotic fluid into peritoneal cavity at cesarean section is almost inevitable and is usually insignificant in terms of symptomatology, it may rarely progress to peritonitis. 13 The exact mechanism leading to the development of such a complication is unknown. 8
We present a case of peritonitis due to vernix caseosa diagnosed soon after vaginal delivery in a patient with previous cesarean section. As far as we are aware, this is the first case of VCP reported following vaginal delivery.
Case Presentation
Mrs. A, 28 years old, G3, para 2, was admitted at 41 weeks gestation in active labor with a history of onset of regular contractions about 1 hour before admission. There was no history of ruptured membranes and she had no previous medical problems.
She had a lower segment cesarean section at term in 2005 for non-reassuring fetal status followed by normal vaginal delivery of a 3.5 kg baby in 2010.
She had uneventful antenatal care at the primary care center. Antenatal ultrasound examination at 14 weeks revealed normal findings for the pregnancy, and the ovaries were normal.
At admission to the labor room, her general condition was satisfactory, and her vital signs were as follows: temperature of 37.2 °C, heart rate of 110 beats per minute, blood pressure of 115/70, a respiratory rate of 18–20 breaths per minute, and oxygen saturation of 100% on room air. The cervical ostium was 8 cm dilated, the presentation was vertex at 2 cm above the ischial spine. Artificial rupture of membranes was performed and the amniotic fluid was clear. In view of repeated fetal heart decelerations, vacuum extraction was performed and a male baby, 4.410 kg, was delivered with an Apgar score of 7 in 1 minute and Apgar score of 8 in 5 minutes.
The results of investigations at admission were hemoglobin: 12.9 gm/dL; platelets: 158 × 109/L; white blood cell count (WBC): 10.6 × 109/L; polymorphs: 75%; and lymphocytes: 16%.
Three hours after delivery, she developed a fever of 37.9
Systemic examination showed a soft, mildly distended abdomen with generalized diffuse tenderness. There was no rigidity, guarding, or abnormal mass on abdominal examination.
The results of further investigations were as follows: WBC, 17.4 with polymorphonuclear leucocytes of 93%; lymphocytes, 3%; hemoglobin, 11.6 gm/dL; and platelets, 149.
Ultrasound examination of the abdomen revealed the following findings: significant amount of free fluid in the hepatorenal and lienorenal angles and also in the pelvis, normal ovaries and a normal puerperal uterus, and a small hemangioma in the liver.
There was cross-consultation with the general surgeon who advised that computed tomography (CT) of the abdomen with contrast be performed, and preparation for this procedure was initiated. However, because the abdominal pain increased in severity over the next 2 hours, a decision was taken not to undertake this investigation, but rather to proceed with more definitive treatment.
A decision was taken for laparotomy, with the probable differential diagnoses of ruptured uterine scar or other surgical emergencies under consideration. Laparotomy was performed with collaboration of the surgeon. The operative findings included about 500 mL of turbid fluid in the peritoneal cavity, with patches of cheesy material on the serosal surface of all viscera; the uterus was intact, with an intact uterovesical fold of the peritoneum and the anterior and posterior walls of the uterus. In addition, the ovaries and fallopian tubes were normal. The appendix, liver, spleen, and intestines were all normal.
A biopsy was taken from adjacent mesenteric lymph nodes, which were found to be slightly enlarged. The uterovesical fold was opened to examine the uterus. The lower segment was found intact. Some patches of the cheesy material, some peritoneal fluid, and omental biopsy were taken and sent for histopathology. Peritoneal lavage was performed using about 1 L of physiological normal saline.
Postoperatively, she was treated with intravenous ceftriaxone and metronidazole. Recovery was uneventful, and she was discharged on the 5th postoperative day.
Histopathological examination of peritoneal fluid and the cheesy material showed many keratin flakes and a rare squame mixed with severe mixed inflammatory infiltrate of neutrophils and lymphonuclear cells, as well as a very rare giant cell, but there were no granulomas, caseation, or necrosis evident. The omental biopsy showed many areas of keratin flakes and nonspecific mixed inflammation; there were neither granulomas nor caseation observed. The mesenteric lymph node biopsy showed nonspecific reactive changes. Based on the findings of the peritoneal contents and the omentum, a diagnosis of VCP was made. Some of the histopatholigical findings are depicted in Figures 1 and 2.
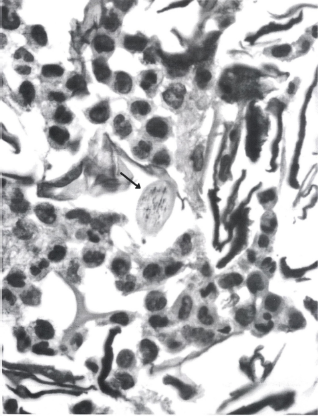
Microphotograph showing lanugo hair (arrow) amidst acute inflammatory cells, keratin flakes, and anucleate squames.
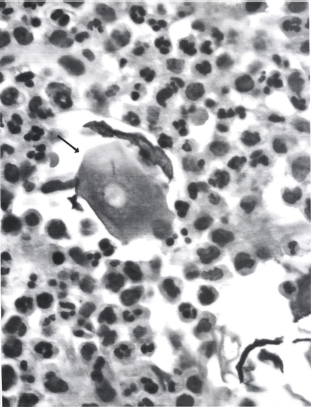
Anucleate squamous epithelial cell (arrow) surrounded by keratin flakes and acute inflammatory reaction.
Discussion
Vernix caseosa, the cheese-like white cutaneous material covering the skin of the newborn, consists of a mixture of sebaceous glandular secretions, lanugo hairs, and desquamated squamous cells. These squamous cells are described as being derived from fetal periderm. Numerous squamous cells are present in the amniotic fluid.4,5 The onset of peritonitis due to vernix caseosa occurring after uncomplicated cesarean sections has been attributed to incomplete peritoneal lavage of spilled amniotic fluid, 7 although this spillage is usually insignificant and only rarely does it progress to peritonitis. 13 Davis et al 7 and Schwartz et al 11 have reported that peritonitis due to vernix caseosa could be initiated by antenatal or intrapartum leakage of amniotic fluid, the suggested mechanisms being utero tubal reflux,7,15 and unrecognized uterine perforation. 11 In our case, uterine perforation was clearly ruled out, but intrapartum utero tubal reflux spill could not be excluded, and we therefore support this hypothesis as the probable initiating factor in the pathology of this patient.
Although the exact cause of the subsequent development of peritonitis is not known, different theories have been suggested. Both meconium and keratinised squamous cells have the capacity to induce a brisk inflammatory response, collectively or individually, most probably by mechanical irritation 6 —the former in the setting of neonatal meconium peritonitis secondary to intestinal perforation, and the latter in the context of ruptured keratinous cysts, dermoid cysts, and keratinizing neoplasms. Interestingly, meconium is composed largely of swallowed amniotic fluid (which contains anucleate squamous cells and lanugo hair derived from vernix caseosa). 9 Furthermore, it is recognized that direct spillage of meconium into the peritoneal cavity can incite a granulomatous peritonitis. The concentration of vernix caseosa in the amniotic fluid may have pathogenetic significance.
A hypersensitivity reaction may occur from sen-sitization occurring from previous pregnancy and delivery (as in multipara), or from an antenatal primary event. 3 In keeping with hypersensitivity reactions, there are too few cases reported to see whether multipara have more exaggerated responses, and this is a potential focus of future research.
The principal symptoms of VCP are generalized severe abdominal pain, pyrexia, peritonism, and elevated WBC, with inconclusive or normal imaging. It can present within a few days to weeks after an inciting event. Other causes of peritonism should be excluded including intraperitoneal sepsis, endometritis, bowel injury, appendicitis, cholecystitis, perforated viscus, and ruptured uterus. The case presented had the hallmarks of the scenario stated above.
Observation of the white and yellow cheese-like plaques within the peritoneal cavity and on the serosal surfaces of the visceral organs like the omentum and appendix during laparoscopy/laparotomy should raise suspicion of VCP. Absence of inflamed organs with the presence of these patches on the serosal surfaces is the sine qua non of VCP. 8 Appropriate serosal biopsies are needed to confirm the diagnosis in the absence of other identifiable pathologies. The findings in the case we have presented are similar to those stated above, and the management protocols followed are based on the principles stated above.
Histological examination of the cheesy white exudates shows they are of fibrinous nature, containing epithelial squamous cells, lanugo hair, and probably sebum. The characteristic desquamated squamous cells appear singly or in clumps, and are polygonal or ovoid in shape. The nuclei are absent; however, nuclear ghosts are frequently present. Increased acid phosphatase enzyme activity is reported to be characteristic.4,5
Cases of peritonitis due to vernix caseosa occurring shortly after delivery have neutrophils as the predominant primary reactant, which was the feature in our case, as it occurred soon after delivery. After several days, both an acute and foreign body inflammatory reaction will usually be evident. Cases occurring at a longer interval after delivery demonstrate predominantly granulomatous foreign body reactions.7,9
Tawfik et al 6 suggested evaluation by preoperative CT and fine-needle aspiration cytology in suspected cases. A recent study showed that radiological imaging may identify lesions in the abdominal wall or peritoneal cavity, and diagnosis can be made by image-guided biopsy. 1 However, this may not be always practical and many patients undergo surgical exploration.
In our case, the acute presentation in a patient with previous cesarean section soon after an instrumental vaginal delivery made us suspect a ruptured uterine scar, with subsequent hemoperitoneum, which led us to embark upon a surgical exploration; CT scan was therefore considered unnecessary. A diagnostic and exploratory laparoscopy 14 with intraoperative pathological examination of the cheesy exudates could have prevented the exploratory laparotomy with a midline incision, although such a procedure would not have offered full treatment for a suspected ruptured uterus. The fact that the patient presented in labor with fever, tachycardia, and histopathological findings of neutrophilic infiltration point to an intrapartum-inciting event (most probably uterotubal reflux specifically), as the previous scar was found to be intact during the laparotomy.
Although in our case there was no need for removal of any viscera, many cases reported in the literature had significant additional procedures at laparotomy including cholecystectomy, 5 appendectomy,1,3,8,11 partial colectomy, 9 total hysterectomy, 12 bilateral salpingectomy,8,12 and so on, with subsequent finding of normal histology in the excised organs.
Various options of conservative treatment have been contemplated, as reported by many authors.7,9,10,12 Some authors have advocated postoperative antibiotic therapy.4–6,8,11,15 Adjuvant steroid therapy was used in two cases with resistant symptoms when infection has been excluded. 8 These authors 8 have postulated that steroids significantly enhanced the clinical course by suppression of the inflammatory response, thus facilitating recovery achieved in their cases. All the treatments discussed above remain empirical and controversial since none of them are really evidence-based. We believe that there is need for a more comprehensive study of VCP to establish a more universally accepted treatment regimen.
Stuart et al 3 reported significant morbidities following the initial diagnosis of VCP, including bowel obstruction, that required further operative procedures. So, although VCP may be self-limiting and may resolve with conservative management alone, the authors suggest monitoring the postoperative course in those diagnosed with VCP since delayed morbidities may arise.
Clinical diagnosis of peritonitis due to vernix caseosa should be considered in patients presenting postpartum with an acute abdomen.
Conclusion
VCP is an infrequent cause of puerperal peritonitis caused by spillage of amniotic fluid into the peritoneal cavity. It was previously reported only after cesarean section, but it can also occur even after vaginal delivery (as illustrated by the case presented), since the inciting event can occur during the antenatal or intra-partum period. The diagnosis of VCP should be kept in mind in any patient presenting with postpartum acute abdomen. Characteristic intraoperative findings and intraoperative diagnosis with involvement of a pathologist can help in decision-making with respect to the type of management employed, which may lead to a more conservative approach, and thus prevent unnecessary invasive procedures.
Author Contributions
SAS, FIAD, IAS and MFD were directly involved in the management of the case. SN provided the pathological analysis. SAS and FIAD prepared the initial draft of the manuscript, and also performed some of the literature searches. MFD made additional amendments/additions to the manuscript and provided a further literature search. All the authors have read, suggested modifications for, and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.