
Abstract
A 66-year-old woman receiving continuous ambulatory peritoneal dialysis developed acute respiratory distress 12 hours after a fall. Blood gas analysis revealed hypoxia (PaO2 67.7 torr) and metabolic acidosis with an increased anion gap, consistent with lactic acidosis (lactate, 86.5 mg/dL; normal range, 4.0–16.0). Magnetic resonance imaging showed a lumbar vertebral body fracture. On the fourth hospital day, the patient died of multiorgan failure and disseminated intravascular coagulation. Postmortem studies revealed fat emboli in the systemic circulation, ie, fat embolism syndrome. Diagnosing fat embolism syndrome can be difficult in patients on dialysis or in those with collagen vascular or pulmonary diseases.
Introduction
Fat embolism syndrome (FES) is defined as the presence of fat emboli not only in pulmonary system but in the systemic circulation as well, with systemic ischemic or inflammatory signs such as neurological, renal, and cutaneous manifestations. 1 This condition may result in a fatal outcome. Pulmonary fat emboli occur in more than 90% of patients with long-bone fractures, 2 but the frequency of FES is reported to be between 0.9% and 11% following multiple bone fractures or lower long bone or pelvic fractures.2–4 Other conditions such as orthopedic surgery 5 and liposuction for obesity 6 have been reported as causes of FES. However, FES is very rare with vertebral body fractures7–9 despite their relatively high prevalence in the general population. 10
This is the first English-language case report describing FES following traumatic vertebral body fracture in a patient receiving continuous ambulatory peritoneal dialysis (CAPD) for anuric renal failure secondary to scleroderma renal crisis (SRC). We discuss the diagnostic criteria and therapeutic options for FES with a literature review.
Case Report
A 66-year-old woman was transferred to the Aichi Medical University Hospital emergency room because of severe back and abdominal pain after she slipped and fell 12 hours earlier. Prior to this, she had been treated with antihypertensive medication for 11 years. Ten years prior to admission, she was diagnosed with systemic scleroderma and was started on prednisolone (PSL) at 15 mg/day. Seven months prior to admission, CAPD was started for anuric renal failure secondary to SRC due to difficulties in creating a vascular access site as a result of systemic scleroderma. She was maintained on CAPD without any problems. Two months prior to admission, her blood pressure stabilized at 100–120/60–80 mmHg. Although PSL was continued at 9 mg/day, the following medications were discontinued: an angiotensin-converting enzyme inhibitor, an angiotensin receptor blocker, and a calcium channel blocker. One week before admission, blood gas analysis drawn while breathing room air showed pH 7.43, PaO2 96 torr, PaO2 39.4 torr, and serum bicarbonate 25.3 mmol/L, a normal study.
Twelve hours prior to admission, the patient slipped and fell in a passageway in her home and immediately experienced severe left-sided back pain and abdominal pain. She was transferred to our hospital's emergency room. She had normal mental status and a clear state of consciousness. Her height was 162 cm and her weight was 48.4 kg. Her body temperature was 36.0 °C, pulse was 129 beats/min and regular, respiratory rate was 24 breaths/min, and blood pressure was 154/98 mmHg. A physical examination revealed fine crackles audible in both lower lung fields, severe scleroderma on the upper and lower extremities, and an aggravated blue color and ulcerations on the fingers and feet. Blood oxygen saturation was 92%. Blood gas analysis of a sample drawn while the patient was breathing room air revealed pH 7.32, PaO2 67.7 torr, PaCO2 17.3 torr, and serum bicarbonate 8.9 mmol/L. The patient had severe metabolic acidosis with an elevated lactate level of 86.5 mg/dL (normal range: 4.0–16.0). The alveolar-arterial oxygen tension difference (A-aDO2) was 60 (normal range: below 20). Serum sodium was 131 mmol/L, potassium was 4.1 mmol/L, and chloride was 103 mmol/L. The patient's white blood cell count was 13,500/µL, red blood cell count was 259 × 104/µL, hemoglobin was 8.8 g/dL, hematocrit was 26.2%, platelet count was 20.7 × 104/µL, albumin was 2.9 g/dL, blood urea nitrogen was 64.9 mg/dL, and creatinine was 5.12 mg/dL. Aspartate aminotransferase (AST) was 78 IU/L, alanine aminotransferase (ALT) was 56 IU/L, and lactate dehydrogenase (LDH) was 521 IU/L. Her C-reactive protein level was 4.91 mg/dL and anti-nuclear antibody titer was elevated at 1:320 in a speckled pattern. The anti-Scl-70 antibody level was 3600 U/mL (normal range: below 10 U/mL). Blood tests were negative for anti-centromere, anti-RNP, anti-SS-A and SS-B, and myeloperoxidase-anti-neutrophil cytoplasmic antibodies, hepatitis B antigen, hepatitis C virus antibody, and cryoglobulins.
X-rays of the chest, abdomen, and pelvis revealed a large homogenous shadow in the right upper and middle lung fields and a reticular shadow in the left middle lung field (Fig. 1A) and no evidence of pelvic fractures. Computed tomography (CT) of the chest revealed massive infiltration of the right middle lung field (Fig. 1B).

Sagittal T1 weighted and fat-suppressed T2 weighted magnetic resonance imaging (MRI) of the lumbar spine showed a vertebral body fracture at the level of L1 (Fig. 1C).
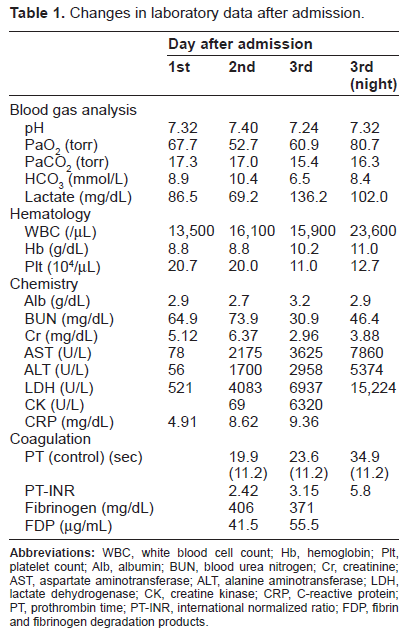
After admission, we investigated the cause of hypoxia and severe lactic acidosis with oxygen therapy and administration of bicarbonate. On the second hospital day, AST was 2175 IU/L, ALT was 1700 IU/L, and LDH was 4083 IU/L (Table 1). Her level of consciousness rapidly decreased to drowsy. Brain CT demonstrated neither bleeding nor infarction. She was transferred to the intensive care unit on the third hospital day. The mode of dialysis was changed from CAPD to hemodialysis in the ICU. She received 20 units of fresh frozen plasma and 400 mL of red blood cells. Serum levels of creatine kinase rapidly increased to 6320 U/L, along with increases in AST, ALT, and LDH levels. Prolongation of prothrombin time and the international normalized ratio, significantly elevated levels of fibrin and fibrinogen degradation products (FDPs), and a rapidly decreasing platelet count suggested disseminated intravascular coagulation (DIC), based on the International Society on Thrombosis and Haemostasis (ISTH) criteria. Initially, we made a diagnosis of pneumonia after the vertebral body fracture was identified. The patient's blood pressure dropped to 80 mmHg. On the morning of the fourth hospital day, she died from multiorgan failure and disseminated intravascular coagulation.
Changes in laboratory data after admission.
Postmortem Pathological Studies
Pathological studies demonstrated fat emboli, including bone marrow cells in the pulmonary artery (Fig. 1D), gastrointestinal artery (Fig. 1E and F), and adrenal glands (data not shown). In both lungs, partial bronchopneumonia and diffuse pulmonary fibrosis were observed. Necrosis was observed in the small intestines, descending colon, and liver (data not shown). Fibrointimal sclerosis with adventitial fibrosis in the large- and middle-sized arteries of the kidney and ischemic glomerular collapse with double contouring of the basement membrane (tram-tracking) were compatible with chronic damage or organization resulting from previous SRCs. Incidental papillary adenocarcinoma without metastasis was observed in the left thyroid gland.
Discussion
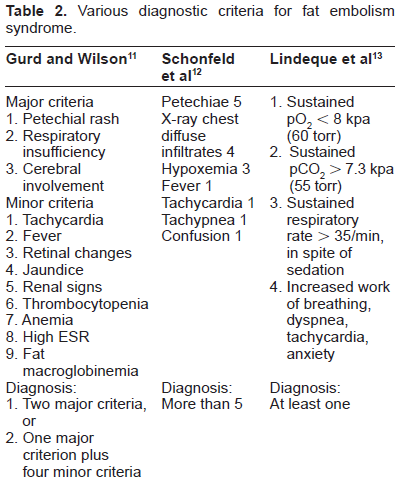
FES is commonly associated with traumatic fracture of the femur, pelvis, and tibia. It is very difficult to diagnose FES in clinical practice. The diagnostic criteria proposed by Gurd and Wilson 11 are typically used, which includes two major criteria or one major criterion with 4 minor criteria compatible with FES (Table 2). Schenfeld et al proposed a quantitative scoring system for diagnosing FES; a score greater than 5 is required to diagnose FES (Table 1). 12 Based on the involvement of the respiratory system alone, Lideque et al added another criterion (Table 1). 13 There is currently no consensus on how to diagnose FES. 14 In the present patient, hypoxia with PaO2 less than 60 torr, the first major item in Gurd and Wilson's criteria, was not met, since her PaO2 was 67.7 torr. However, severe lactic acidosis suggests tissue anoxia, and a sudden large, 60-torr increase in A-aDO2 (normal range: less than 10 torr) also suggests pulmonary emboli or infarction compared to the patient's normal blood gas analysis values of pH 7.43, PaO2 96 torr, PaO2 39.4 torr, HCO3 25.3 mmol/L one week before admission. Regarding the decreased level of consciousness, the present patient had normal consciousness upon arrival in the emergency room, but her level ofconsciousness rapidly decreased the next day. Unfortunately, brain CT could not detect cerebral infarction or bleeding. Normal CT findings led to a decision to not recommend a further MRI study, which is useful tool for diagnosis of FES. Regarding petechiae, the present patient with scleroderma already had thickened skin, telangiectasias, and livedo-like skin lesions. It was very difficult to distinguish whether the rapid progressive blue color on the fingers was due to fat emboli or an aggravation of scleroderma. The present patient fulfilled only one minor criterion, tachycardia, but other criteria such as urinary condition could not be evaluated because she was receiving continuous peritoneal dialysis for anuric renal failure due to SRC. In patients on dialysis and systemic sclerosis, Gurd and Wilson's criteria are unsatisfactory.
Various diagnostic criteria for fat embolism syndrome.
The development of FES from pulmonary fat emboli is thought to include two mechanisms: the first is the presence of right-to-left shunting due to an atrial septal defect or patent foramen ovale 15 and the second is that fat tissue, including bone marrow cells, which can pass through pulmonary capillary networks into systemic circulation, which may be associated with fatty acid generation by pneumocytes. 16 In the present case, autopsy did not identify a patent foramen ovale or a right-to-left shunt.
Vertebral body fractures are rare causes of FES, although the prevalence of vertebral body fractures is approximately 20% in postmenopausal women over the age of 50 years in Europe. 10 There are no detailed data on the prevalence of mild FES in patients with acute vertebral body fractures. One possibility is that a mild degree of fat embolism is associated with vertebral body fractures, but less frequently with FES. Day et al described a case of FES in a patient receiving 25 mg/day of prednisolone following lung transplantation with numerous non-traumatic vertebral body compression fractures. 7 They pointed out the role of long-term steroid use in the development of vertebral fractures. Lewis et al reported FES in a patient with a lumbar wedge fractures following a fall. 8 In the present case, long-term use of steroids may have contributed to the development of fatal FES.
Regarding therapy for FES, supportive therapy and the fixation of fractured bones are essential following bone fracture; however, steroid therapy has also been proposed for treating acute endothelial injury and minimizing the inflammation caused by the release of fatty acids from bone marrow cells. 12 The question of whether steroid administration can prevent FES after bone fracture remains controversial. 16 A meta-analysis showed that steroid therapy decreased the incidence of FES to 78%; 17 however, there was no significant difference in survival rates between patients undergoing steroid therapy and those receiving no treatment. In addition, there is no consensus on whether large or small doses of steroids result in better outcomes. 18 In addition to balanced electrolyte solutions, albumin has been recommended for volume resuscitation because it not only restores blood volume but also binds to fatty acids and may thus decrease the extent of lung injury. Steroids, heparin, alcohol, and dextran have been found to be ineffective. 19
Conclusions
The present patient had autopsy-proven FES following a traumatic vertebral body fracture. Clinical and laboratory findings such as acute respiratory distress, increased A-aDO2 with lactic acidosis, and acute onset of ischemic skin lesions can help the clinician diagnose FES.
Author Contributions
Wrote the first draft of the manuscript: NN, YK. Contributed to the writing of the manuscript: HI. Agree with manuscript results and conclusions: SM, MK, KK, NS, KS, NM. Jointly developed the structure and arguments for the paper: TY. Made critical revisions and approved final version: TY, SB. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.