
Abstract
Blastic plasmacytoid dendritic cell neoplasm (BPDCN) is an aggressive myeloid neoplasm derived from plasmacytoid monocytes. The most common presentation involves cutaneous manifestations, which are often accompanied by bone marrow involvement. The tumor cells reveal an immature blastic appearance and diagnosis is based on the expression of cluster of differentiation (CD)4 and CD56. The literature reports a high relapse rate and poor prognosis when treated with leukemia-type induction chemotherapy alone; however, long-term remission is attainable with allogeneic stem cell transplantation in the first complete remission. Here, we report the dismal course of a patient with BPDCN with cutaneous and bone marrow involvement unable to undergo an aggressive intervention.
Introduction
Blastic plasmacytoid dendritic cell neoplasm (BPDCN), previously known as blastic natural killercell lymphoma, is a rare hematological malignancy derived from immature plasmacytoid dendritic cells. 1 The tumor cells reveal an immature blastic appearance, and diagnosis is based on the expression of cluster of differentiation (CD)4 and CD56 in the absence of other lymphoid, natural killer, or myeloid antigens. 2 BPDCN has been reported in childhood, but the majority of affected individuals are elderly with a mean age of 66 years. 3 Male to female predominance is approximately 3:1. 4 Common presentation includes cutaneous lesions followed by tumor dissemination, though early bone marrow involvement can manifest like acute leukemia, requiring prompt intervention. Treatment with conventional chemotherapy has proven ineffective and requires allogeneic hematopoietic stem cell transplantation for remission. 5
Case Report
A 69-year-old male with a past medical history significant for atrial fibrillation and hypertension presented for a routine clinic visit in December 2011. A review of systems was negative with the exception of a 1-month history of fatigue. Physical exam revealed macular, lightly pigmented lesions on the chest and left shoulder (Fig. 1). Routine labs included a complete blood count (CBC), which showed a white blood cell count of 3,200, with the differential reported as 44% lymphocytes and 9% atypical lymphocytes (Fig. 2), hemoglobin of 11.2, with a mean corpuscular volume of 106.9, and a platelet count of 80,000. The patient was scheduled for bone marrow biopsy and biopsy of his skin lesions within the following month. Pathology from the bone marrow biopsy revealed 80% cellularity with interstitial infiltration by a mononuclear cell population. The aspirate showed numerous mononuclear cells with fine nuclear chromatin, variable prominence of nucleoli, and finely vacuolated cytoplasm, comprising 75% of the cells (Fig. 3). Additionally, there was erythroid megakaryocytic and granulocytic hypoplasia. On flow cytometry, the blast-like population stained positive for CD45, CD56, CD4, CD123, and CD43. Immunohistochemical stains revealed that the neoplastic cells were also positive for CD68. A punch biopsy of the left upper chest lesion showed a monomorphic population of mononuclear cells in the dermis that was infiltrative of adnexal structures (Fig. 4). The skin biopsy findings, in combination with the bone marrow biopsy results, were consistent with the diagnosis of BPDCN. A positron emission tomography scan was obtained, which revealed bony lesions in the right proximal humerus, L3 vertebral body, left ileum, and bilateral acetabula. Diffusely increased uptake was seen in the marrow in the proximal humerii, proximal femora, pelvis, and vertebral bodies. Initiation of treatment with hyper-central venous access devices (CVAD) and allogeneic stem cell transplant (allo-HCT) was evaluated. The patient was considered a poor candidate for high-dose chemotherapy after his course was complicated by pneumonia, in addition to the high morbidity and mortality rate associated with the patient's advanced age. Plans were made to initiate bendamustine, since more aggressive regimens were not an option; the patient opted for no chemotherapy given his poor prognosis.

Gross description of left-shoulder lesions.

Circulating neoplastic cell (Wright-Giemsa; original magnification ×100).

Neoplastic cells in bone marrow aspirate (Wright-Giemsa; original magnification ×50).
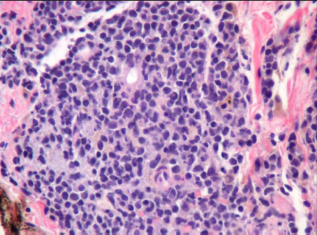
Dermal infiltrate of neoplastic cells (hematoxylin and eosin; original magnification ×50).
The patient's pancytopenia improved and his functional status returned nearly to baseline within the 2 months following the decision to decline chemotherapy. Unfortunately, 6 months after diagnosis, the patient's condition and performance status acutely and rapidly declined. In May 2012, the CBC revealed a white blood cell count of 33,200 and 30,000 platelets. Examination of this peripheral blood by flow cytometry revealed a leukocytosis with 80% abnormal blasts and decreased platelets. There was an abnormal blastic plasmacytoid dendritic cell population staining positive with CD45, CD56, CD123, CD10, human leukocyte antigen(HLA)-DR, CD38, CD4, partial CD36, and CD2. CBC 2 weeks later revealed worsening leukocytosis to 83,000 with 33% bands and a platelet count of 15,000. The patient decided to proceed with hospice care and died 10 days later.
Discussion
BPDCN is a rare neoplasm derived from immature plasmacytoid dendritic cells. The case presented demonstrates the classic presentation of skin and bone marrow involvement. The phenotypic appearance of the cutaneous lesions is variable, ranging from local to diffuse, and it can look like ecchymosis or deep red plaques. Many atypical skin rashes can mimic the cutaneous manifestations of BPDCN, but these are not typically associated with hematologic abnormalities. Without the hematologic findings of pancytopenia in our patient, the decision to biopsy may have been delayed. It is crucial to delineate BPDCN from atypical rashes, as well as from other differentials including T-cell lymphoma, lymphoblastic lymphoma, granulocytic sarcoma, and chronic myelogenous leukemia, as prognosis is poor with delay in treatment.
As seen in the case described above, diagnosis can be confirmed with skin and bone marrow biopsy. According to the 2008 World Health Organization classification of myeloid neoplasms, the blasts in BPDCN are characterized by the expression of CD4, CD43, CD56, CD123, BDCA-2/CD303, TCL1, and conjucated linoleic acid. 6 The flow cytometry for our patient stained positive for CD4, CD43, CD56, CD123, CD45, CD10, CD36, HLA-DR, CD38, and CD2 on bone marrow biopsy at the time of diagnosis, and on peripheral blood later in the disease course. The only differences noted on flow cytometry from the two samples was dim terminal deoxynucleotidyl transferase, dim CD33, and partial CD7 expression on the bone marrow biopsy that was not expressed on the peripheral blood sample. Identified key marker CD2-associated protein was not evaluated in our patient, but does appear to be restricted to plasmacytoid dendritic cells, making it potentially useful in confirming the diagnosis of BPCDN. 7
Due to the limited prospective data of this rare disease, no standard of care treatment has been established for BPDCN. The literature reports intense regimens such as hyper-CVAD to have the highest complete response (CR) rate, up to 90% in one study. 8 Daunorubicin plus cytarabine followed by high-dose cytarabine, or an acute lymphoblastic leukemia-like induction regimen achieved a CR rate of 83% in six patients, as reported in another study. 4 CHOP-like regimens (cyclophosphamide, hydroxyl doxorubicin, vincristine, and prednisone) and ifosfamide/etoposide-based regimens have been used, but according to the literature, they only have CR rates of 40%–50%. 7 The CR rates of induction treatment with these aggressive regimens are encouraging, but conventional chemotherapy alone without stem cell transplantation has not been proven to sustain longterm remission regardless of the therapy used.
Current literature supports allo-HCT in the first complete remission for long-term remission in patients with BPDCN. 5 Based on a report from the European Group for Blood and Marrow Transplantation, there was an increase in disease-free survival, an increase in overall survival, and no relapses within 27 months in patients who received allo-HCT in the first CR. There is rare data reporting the use of high-dose therapy followed by autologous stem cell transplantation, but no clear benefit or long-term remission was achieved. 7
In the case presented, the comorbidities and advanced age of the patient excluded him from any intense therapy. For cases such as this, reduced intensity regimens (RIC) are being used to expand treatment options. One case reported long-term remission in two out of four patients, 4 who underwent treatment with fludarabine, cyclophosphamide, and busulfan at subablative doses, or fludarabine plus treosulfan, followed by RIC allo-HCT. 4 Data is limited in regards to RIC regimens, but they are supported for patients unable to undergo more aggressive interventions. 7
The rapid decline of our patient highlights the aggressive nature of BPDCN without prompt intervention. Only 6 months passed from the time of diagnosis until death. Fatigue was intermittent throughout the course, but quickly became a debilitating symptom in the days before his passing. In any case, whether initiating intense treatment or discussing goals of care, it is important to understand this rare disease process to provide real expectations for the patients affected.
Author Contributions
Conceived and designed the experiments: LP, CD, SM. Analyzed the data: LP, CD, SM. Wrote the first draft of the manuscript: LP. Contributed to the writing of the manuscript: LP, CD, SM. Agree with manuscript results and conclusions: LP, CD, SM. Jointly developed the structure and arguments for the paper: LP, CD, SM. Made critical revisions and approved final version: LP, CD, SM. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.