
Abstract
We present clinical features and tremor characterization in a patient with Parkinson's disease (PD) as well as in two cases of essential tremor (ET) with some parkinsonian features but no evidence of dopaminergic terminal loss on 123I-FP-CIT Single Photon Emission Computed Tomography (SPECT). Relatively slow frequency rest tremor and bilateral upper extremity bradykinesia without decrementing amplitude were observed in the ET cases, with unilaterally decreased arm swing in case 3. Alternating rest tremor and re-emergent tremor with 13 second latency was confirmed in the PD case. Re-emergent tremor had alternating characteristics, which to our knowledge has not been previously reported. The ET cases had synchronous postural tremor. Alternating re-emergent tremor in PD provides further evidence for re-emergent tremor as an analogue of rest tremor in PD. Two cases of ET with synchronous postural tremor and one to two year history of parkinsonian features had no evidence of dopaminergic terminal loss up to 40 years after the initial onset of ET. Tremor synchronicity characterization can assist in differential diagnosis between the two disorders.
Keywords
Introduction
Jean-Martin Charcot used handwriting samples to aid in differentiation of essential tremor (ET) and Parkinson's disease (PD), with ET demonstrating tremulous handwriting and PD demonstrating bradykinesia. 1 Today's clinician may be confronted with cases on the borderzone of ET and PD as some symptoms may overlap. For example, rest tremor and mild bradykinesia have been reported in ET. 2 We present three cases with overlapping symptoms along with clinical, electrophysiological, and nuclear imaging findings used to make the diagnosis. We hope this information will help clinicians facing similar diagnostic quandaries.
Detailed tremor characterization may be of help in differentiating ET and PD. Alternating flexor and extensor muscle contraction has been demonstrated in rest tremor of PD. 3 Re-emergent tremor has been described by Jankovic et al 4 as a possible analogue of rest tremor in PD patients, with similar frequency characteristics. Postural tremor in ET has been initially thought to be solely synchronous, 3 but Sabra and Hallett 5 described a less common asynchronous or alternating form of ET postural tremor. PD rest tremor has been shown to be alternating on short term recordings in multiple studies. 3 Long term tremor monitoring of ET and PD tremor without differentiating rest vs. postural tremor by Spieker et al 6 revealed a more variable pattern in both disorders, with alternating tremor still dominating in PD and having a 78% predictive value for PD vs. ET. 6 In a series of 15 patients with ET and 15 patients with PD, Nisticó et al 7 showed that all ET patients had synchronous rest tremor while all PD patients had alternating rest tremor on short term recordings. 7 To our knowledge, synchronicity characteristics of re-emergent tremor in PD have not been previously evaluated.
Other clinical findings that may help with PD diagnosis include bradykinesia with fatigable or decrementing amplitude, facial hypomimia, and decreased arm swing, but rarely even their presence is not fully consistent with idiopathic PD. 8 Patients with clinical diagnosis of PD who have normal nuclear imaging are termed subjects without evidence of dopaminergic deficit (SWEDDs) 8 and their tremor is thought to be due to dystonic tremor. 9
Materials and Methods
The patient were examined and videotaped with written consent while seated with arms at rest as well as in the outstretched position. Case 2 was also evaluated with elbow flexed at 30 degrees to demonstrate crescendo postural tremor that occurs when she holds a telephone handset to her ear. Patients were asked to perform activation maneuvers consisting of serial seven subtractions or foot tapping to demonstrate upper extremity tremor. Clinical rating of tremor severity according to MDS-UPDRS scale was performed. Regions of interest in video clips corresponding to each tremulous limb were analyzed via Fast Fourier Transform in TremAn software to obtain tremor frequency. 10
Rest and postural tremor was also analyzed in both positions via surface electromyography (EMG) electrodes of appropriate muscles. A dual channel recording was made via Teca Synergy EMG (CareFusion, San Diego, CA). Tremor frequency was obtained from muscle contraction frequency on EMG tracing in addition to data from TremAn. For rapid clinical evaluation of tremor synchronicity, visual assessment of simultaneous dual channel agonist and antagonist muscle contraction was used. The more complex mathematical evaluation of tremor synchronicity presented by Spieker et al 6 was not used given challenges in data acquisition and processing during a brief clinical visit.
Dopamine transporter imaging of cases 2 and 3 was performed via 123I-N-fluoropropyl-2b-carbomethoxy-3b-(4-iodophenyl) nortropane (123I-FP-CIT) single photon emission tomography (SPECT) with image acquisition 3 hours post intravenous injection of radionuclide (DaTSCAN; GE Healthcare, USA). Nuclear imaging of dopamine transporter allows for evaluation of presynaptic dopaminergic terminal loss in the caudate and putamen. These axon terminals are projections of dopaminergic neurons of the substantia nigra.
Case Presentations
Case 1
The first case is a 73 year old patient with a five year history of left upper extremity rest tremor, mild left upper and lower extremity bradykinesia, mild left upper and lower extremity rigidity without activation, and decreased left arm swing who carried a diagnosis of PD. Distal interphalangeal joint flexion consistent with left striatal hand deformity was present. The rest and re-emergent tremors had 3+ moderate amplitude wrist flexion/extension and pronation/supination components in addition to milder thumb flexion/ extension.
Video analysis via TremAn software showed a 4.53 Hertz (Hz) rest tremor and a 4.87 Hz re-emergent tremor with 13 second latency (Supplemental Video). A ten second recording of flexor and extensor carpi radialis longus muscle activity of re-emergent tremor was performed via surface EMG. 5.1 Hz frequency was identified on both flexor and extensor channels. Contractions were asynchronous (Fig. 1). A five second EMG recording of rest tremor of the same muscles in the left upper extremity showed asynchronous contraction with 5 Hz frequency. Given classic clinical features and asynchronous tremor, PD diagnosis was maintained.

Partial surface EMG tracing of the flexor (top) and extensor (bottom) carpi radialis longus muscles during re-emergent tremor showing asynchronous activity in case 1.
Case 2
The patient is a 71-year-old right-handed female who developed a right hand postural tremor forty years ago. This tremor was of a very mild amplitude and was noticed when she was holding a piece of paper. About five years ago, she was discovered to have thyroid disease and its treatment improved tremor amplitude. Two years ago, she developed a left lower extremity tremor, much more prominent than right while standing. This tremor seemed to improve after changing the position of her leg. At that time, she also developed a marked crescendo amplitude right upper extremity tremor first noticed when holding a telephone handset. The tremor was also present with other activities that required holding the elbow in a flexed position. She was diagnosed with PD two years prior by another neurologist. She took rasagiline for a year and a half and switched to selegiline due to cost issues. She was also treated with pramipexole during this two year period.
Examination was performed about 5 hours after the patient took immediate release pramipexole and selegiline. The lower extremity tremor could not be observed. There was a mild 1+ amplitude bilateral upper extremity thumb flexion/extension postural tremor with no latency. In addition, she demonstrated no latency crescendo to 3+ moderate amplitude right elbow flexion/extension postural tremor most prominent with elbow flexion to 30 degrees, as if holding a telephone handset to her right ear. There was a metacarpophalangeal (MCP) joint abduction/adduction and wrist flexion/extension rest tremor of the bilateral upper extremities. There was mild bilateral upper and lower extremity bradykinesia. There was no rigidity. She had normal arm swing and stride length as well as no upper extremity tremor during ambulation.
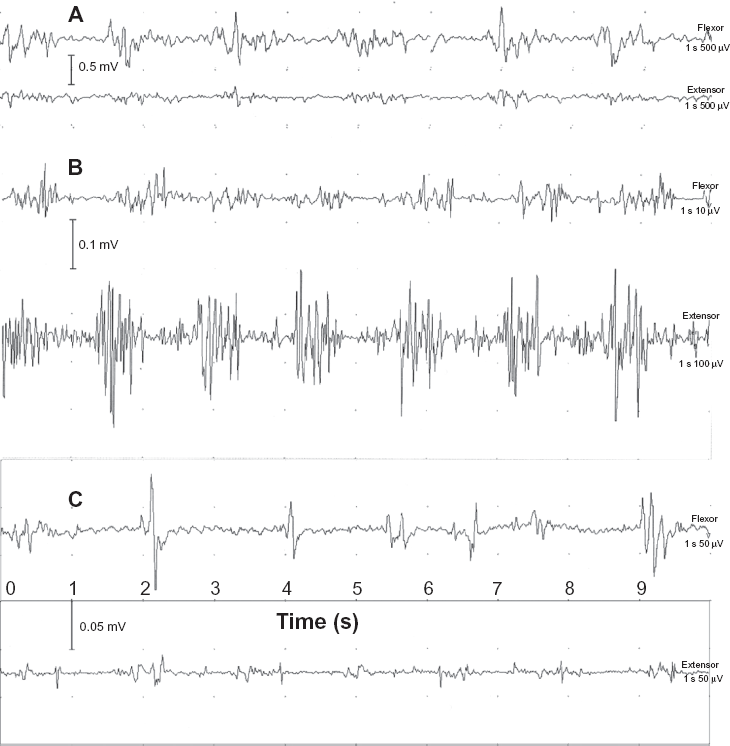
Video analysis via TremAn revealed 6.12 Hz frequency crescendo right elbow postural tremor without latency. TremAn evaluation of rest tremor with activation by foot taps was contaminated with 2.95 Hz video noise, but 4.9 Hz frequency peaks were demonstrated in the upper extremities bilaterally. Surface EMG evaluation showed 6 Hz biceps/triceps synchronous postural tremor of the right elbow (Fig. 2A).
(
123I-FP-CIT SPECT was physiologic. Diagnosis of ET was confirmed and she was tapered off from her PD medications without significant worsening of clinical features. Treatment for ET with beta blockers was initiated.
Case 3
The patient is a 68 year old right handed woman who first noticed action tremor in both hands at age 30. Her father had a history of action tremor of the hands. She has been taking sertraline for the past ten years for treatment of depression. She developed bilateral hand rest tremor and noticed tremor with handwriting one year ago. Bupropion has been tried five months prior to office presentation and was stopped after four months due to increased amplitude of action tremor of the hands as well as truncal tremor. The patient also tried a combination of sertraline and experimental selective norepinephrine reuptake inhibitor LY2216684 for two weeks prior to presentation.
On examination while on sertraline, she had a bilateral 1+ amplitude thumb flexion/extension rest tremor with a frequency of 7 Hz. There was also a no-latency 1+ amplitude postural tremor of the bilateral upper extremities with thumb flexion extension and metacarpophalangeal joint abduction/ adduction. There was mild bilateral upper extremity bradykinesia on finger taps hand grips, hand pronation/supination as well as on foot taps and heel taps. There was decreased right arm swing but no exacerbation of rest tremor during ambulation. There was profound instability with tandem stance. 123I-FP-CIT SPECT scan was physiologic. She was diagnosed with ET as well as possible drug-induced tremor.
EMG evaluation of the left flexor and extensor pollicis brevis muscles revealed a 7 Hz synchronous postural tremor (Fig. 2B) and a 7 Hz synchronous rest tremor (Fig. 2C). Mild amplitude tremor was not amenable to video evaluation by TremAn.
Discussion
These cases demonstrate the challenge experienced by clinicians when attempting to diagnose cases with features that may be present in both ET and PD. Electrophysiological evaluation assisted in diagnosing case 1, while SPECT scan was useful in properly diagnosing cases 2 and 3.
In case 1, presence of distal interphalangeal joint flexion due to striatal hand deformity and re-emergent tremor helped confirm PD diagnosis. Our results in case 1 agree with previous demonstration of alternating rest tremor in PD 3 and support the concept of re-emergent tremor as an analogue of PD rest tremor. 4 To our knowledge, the alternating characteristic of re-emergent tremor in PD has not been previously demonstrated. While re-emergent tremor has been thought to be almost pathognomonic for PD as opposed to SWEDD, 11 a case of re-emergent tremor, rest tremor, and decreased arm swing with normal dopaminergic function has been reported. 12 It would have been of interest to see if the re-emergent tremor in the reported SWEDD case was synchronously similar to rest tremor in present cases 2 and 3. Bajaj et al 8 found no difference in re-emergent tremor between tremor dominant PD and SWEDD groups, with median tremor latency 0.79 s and 0.82 s respectively, with interquartile range of 0–0.5 s and 0–2 s respectively 8 This is in stark contrast to data from Schwingenschuh et al 11 which found PD patients to have postural tremor latency of 2.8 seconds (range 2.6–6.4). Jankovic et al 4 reported postural tremor latency average 0.06 s (±0.28) range 0–1.29 s for ET and average 6.25 s (±9.76), range 0–47.0 s for PD. Given this data, it is likely that brief re-emergent postural tremor latencies (especially 2 s or below) are not useful for differentiating between PD and ET/SWEDD, while latencies of 2.6 s and above provided good separation between the groups with 56% sensitivity and 100% specificity in Schwingenschuh's data set.
Cases 2 and 3 emphasize that presence of some parkinsonian features in the setting of ET does not automatically imply a simultaneous PD diagnosis.
In case 2, relatively slow tremor frequency (about 6 Hz), bilateral rest tremor, and mild bilateral bradykinesia led to an inappropriate diagnosis of PD and unnecessary treatment with monoamine oxidase B (MAOB) inhibitors as well as dopamine agonist pramipexole. Crescendo right upper extremity postural tremor without latency was probably confused with re-emergent tremor of PD. Presence of normal arm swing bilaterally, lack of bradykinesia with decrementing amplitude, and synchronous pattern of tremor (more typical of ET 6 ) were clues to ET diagnosis. Normal 123I-FP-CIT SPECT confirmed absence of dopaminergic deficit. Given asymmetric tremor with exacerbation in flexed elbow position, differential diagnosis includes dystonic tremor. This patient may also be labeled as SWEDD.
In case 3, normal 123I-FP-CIT SPECT scan confirmed ET, with possible contribution of drug induced tremor from sertraline. Synchronous rest and postural tremor, associated with ET, 6 was present. PD was ruled out via nuclear imaging even though there was slow tremor frequency (7 Hz), bilateral upper extremity bradykinesia, and mildly decreased right arm swing during ambulation.
The possibility of SWEDDs with parkinsonism due to FMR1 gene mutation is intriguing. FMR1 gene contains a tract of CGG repeats which is expanded to 200 repeats or more in full mutation leading to Fragile X syndrome. Fragile X-associated tremor ataxia syndrome (FXTAS) occurs in the setting of 55 to 200 repeats, manifests with intention tremor and ataxia, and may occur in females. 13 Parkinsonism with and without evidence of dopaminergic loss on 123I-FP-CIT SPECT was seen in 64% of 22 FXTAS patients evaluated by Apartis et al. 13 The patients in that group were classified into ET-like tremor with average 5.3 Hz frequency distal postural tremor and absent rest tremor or cerebellar tremor prominent slow frequency (3.5 Hz) proximal upper extremity postural tremor and higher amplitude intention tremor, with complete absence of rest tremor. Our case 2 does not fit into either of these categories, as rest tremor was present and the frequency of biceps/triceps tremor was 6 Hertz. Tremor frequency in case 3 was also higher than frequency reported for ET-like tremor in FXTAS. Hence we do not believe that cases 2 and 3 were caused by FMR1 premutation.
Hall et al reported two female subjects with parkinsonism who had gray zone FMR1 expansions consisting of 41–54 CAG repeats as well as one male subject with premutation consisting of 60 CGG repeats. 14 Tremor frequency data was not provided for these patients. They presented with parkinsonism as well as atypical features for PD including head tremor in 2/3 cases and difficulty with tandem gait in 1/3 cases. All three had normal 123I-beta-CIT SPECT imaging. Our cases did not present with these additional features of head tremor or tandem gait difficulty and were unlikely to be caused by FMR1 premutation.
In our cases, mild discrepancy in tremor frequency between EMG and video evaluation may be due to error introduced by video capture and conversion process. It is of interest for future discussions of whether or not there is a mechanistic relationship between ET and PD that our synchronous tremor ET cases had no dopaminergic terminal loss one to two years after the development of multiple parkinsonian features and up to forty years after the initial onset of ET.
In summary, there is no single pathognomonic clinical finding for distinguishing ET and PD. Even presence of classic findings such as re-emergent tremor, decreased arm swing, and bradykinesia with decrementing amplitude does not guarantee idiopathic PD diagnosis via SPECT scanning. Out of these clinical signs, re-emergent tremor has the highest specificity. 11 Demonstration of asynchronous re-emergent tremor may provide additional diagnostic information in complicated cases.
Author contributions
Conceived and designed the study: RF. Acquired and Analyzed the data: RF and JL. Wrote the first draft of the manuscript: RF. Agree with manuscript results and conclusions: RF and JL. Jointly developed the structure and arguments for the paper: RF and JL Made critical revisions and approved final version: JL. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
RF has served as a consultant for Teva, Inc and Lundbeck, Inc, has received grants from Teva and payment for lectures from Teva and Lundbeck, and has received an honorarium from Medlink, Inc.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests. Written consent was obtained from the patients to reproduce information appearing in this work.
Supplementary Video
Footnotes
Acknowledgement
The authors would like to thank Frances Dyro, MD, for her suggestions.