
Abstract
We present a rare cause of hypercapneic respiratory failure through this case report of a 72-year-old man presenting with progressive dyspnea and dysphagia over two years. Hypercapneic respiratory failure was acute on chronic in nature without an obvious etiology. Extensive workup for intrinsic pulmonary disease and neurologic causes were negative. Laryngoscopy and diagnostic imaging confirmed the diagnosis of diffuse idiopathic skeletal hyperostosis, also known as DISH, as the cause of upper airway obstruction leading to hypercapneic respiratory failure.
Keywords
A 72-year-old man lifelong nonsmoker presented to the emergency department with one week of progressive dyspnea on exertion, a non-productive cough and generalized weakness. Review of systems revealed progressive dysphagia, primarily to solids, over two years. He had an incomplete esophagogastroduodenoscopy (EGD) due to difficulty passing the scope. Further workup was deferred by the patient and he modified his diet to include mostly liquids. Multiple episodes of “bronchitis” were treated with antibiotics and he was given a diagnosis of chronic bronchitis by his primary care physician. Past medical history included hypertension, coronary artery disease and diabetes. He denied use of alcohol, narcotics or sedatives. While all personal identifiers pertaining to our patient have been removed, we received consent by the patient to publish the diagnostic images and clinical information relating to this case in our report.
Physical Examination
Vital signs were normal with a room air oxygen saturation of 97%. His respiration rate initially in the emergency department was between 16-18 per minute. He was alert and oriented. Neck exam showed limited range of motion for flexion, extension, rotation and tilt. Accessory respiratory muscle use was absent and his lung exam revealed upper airway inspiratory and expiratory wheezing. Positional changes from sitting upright to supine did not result in any immediate physical changes on exam, although the patient reported less dypsnea in the upright position. Peripheral lung fields were clear without adventitial sounds. Cardiovascular and abdominal exams were unremarkable. He had no peripheral edema. Neurological exam revealed normal strength and sensation with intact reflexes.
Laboratory and Radiographic Findings
Blood work revealed mild leukocytosis with absent left shift and a bicarbonate level of 32 mEq/L. Arterial blood gas (ABG) done 10 hours after arrival to the emergency room showed severe acute on chronic respiratory acidosis: pH 7.14, pCO2 111 mmHg, pO2 56 mmHg and O2 saturation 82.4%. Two hours after initiation of non-invasive ventilation (NIV), the ABG was pH 7.18, pCO2 90 mmHg, pO2 121 mmHg, and O2 saturation 98.5% and the patient's mental status improved. Twenty four hours after initiation of NIV, ABG improved to pH 7.39, pCO2 62, pO2 65 and O2 saturation 92%. CXR revealed right basilar atelectasis (Fig. 1). CT, MRI and MRA of the brain were performed to evaluate for neurologic disease that could contribute to his mental status change and hypercapnia, however they were unremarkable. The toxicology screen was negative. Thyroid stimulating hormone was normal and acetylcholine receptor antibodies were not detected. He was maintained on NIV continuously while sleeping and intermittently during the day. The patient's history of a difficult EGD led to a suspicion for hypercapnia secondary to airway obstruction. Laryngoscopy demonstrated extrinsic compression of the posterior pharyngeal wall with significant anterior displacement (Fig. 2).
Chest radiograph revealed mild right basilar atelectasis. No signs of hyperinflation or focal consolidation present. (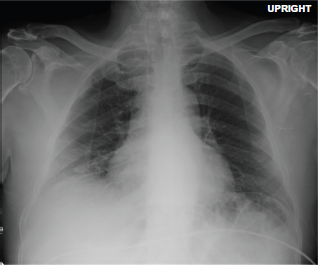

Diagnosis
Hypercapneic respiratory failure secondary to diffuse idiopathic skeletal hyperostosis (DISH).
Clinical Course
Our patient presented with acute on chronic hypercapneic respiratory failure manifested by increasing dyspnea and lethargy. He was initially treated for an exacerbation of chronic obstructive pulmonary disease (COPD) with methylprednisolone, ceftriaxone and azithromycin. In the emergency department he became lethargic and hypoxemic and NIV was begun for suspected hypercapnia secondary to COPD. He did not receive narcotics or benzodiazepines prior to evaluation by the medical intensive care unit (MICU). He was placed on NIV and transferred to the MICU for further workup and management. The patient's respiratory and mental status improved on NIV. He stayed in the ICU for close monitoring of his respiratory status and possible need for immediate endotracheal intubation however he remained alert on NIV with eventual complete resolution of hypercarbia. With improvement in the PCO2 levels, the patient was allowed to rest off of NIV for a few hours at a time as tolerated however, elevations in PCO2 were found on repeat ABGs, making it difficult to wean him off NIV. The history of dysphagia with a difficult EGD remained highly suspicious and prompted the performance of a laryngoscopy and CT scan of cervical spine.
The findings on laryngoscopy were confirmed on a CT scan of the cervical spine which revealed diffuse ossification anteriorly with a large anterior osteophyte at the C3-C4 level and severe mass effect on the hypopharynx and laryngeal inlet with multilevel anterior osteophytic ridging (Fig. 3). The hypercapneic respiratory failure was secondary to upper airway obstruction, a rare complication of DISH.
Noncontrast CT scan of the cervical spine revealed a large anterior osteophytic ridging at C3-C4 (arrow) with severe mass effect upon the hypopharynx and laryngeal inlet.
Orthopedics and otolaryngology were consulted for possible surgical treatment. After a difficult endotracheal intubation was performed in the operating room, both orthopedic and otolaryngology surgeons partnered to perform a partial corpectomy of C4 and C5. A transverse lateral approach was done with lateral mobilization of the carotid artery and revealed extensive ossification of the entire anterior aspect of the cervical spine. After excision of the osteophyte, a high-speed burr was used to smooth the bony surface, and the trachea and esophagus were subsequently decompressed. The patient was extubated on post-operative day 3 without complications. His blood gas normalized and he was discharged on room air without the need for NIV. At one month follow-up in clinic, he reported improved swallowing without symptoms of dysphagia, dyspnea or lethargy off NIV. Both his ABG and pulmonary function tests were normal.
Discussion
DISH, also known as ankylosing hyperostosis and Forestier's disease, is a noninflammatory process with calcification of spinal ligaments and entheses and hypertrophic anterior cervical osteophytes (HACO). Enthesopathy is part of the normal aging process and is usually asymptomatic; however in extreme cases such as DISH it can lead to life-threatening symptoms. The prevalence of DISH varies in the literature from 10% to 35% of patients above 70 years of age, worse in elderly men. 1 Involvement of the cervical spine from the fourth to seventh vertebra with anterior osteophytes most commonly causes dysphagia due to compression of the esophagus from the osteophyte. Dysphagia to solid food occurs in 17 to 28 percent of patients with DISH. 2 Upper airway obstruction secondary to DISH is very rare and can manifest as dyspnea, stridor, cough, or dysphonia, which results from displacement of the laryngopharynx by a large osteophyte typically at the C3 to C4 level. 1 Injury to the recurrent laryngeal nerve on the left side can cause vocal cord paralysis. Several case reports have been published 2 5 describing patients with severe stridor causing respiratory distress and requiring emergent tracheostomy however acute hypercapneic respiratory failure secondary to DISH is rarely described.
There are multiple causes of hypercapneic respiratory failure; our patient's hypercapnia was not consistent with the most common causes. He was not a smoker and did not have COPD by history. CXR revealed no hyperinflation or a significant lung parenchymal process. Obstructive sleep apnea or obesity hypoventilation was unlikely as the patient denied any sleep-related complaints and did not have the typical body habitus. Drug-induced hypercapnia was unlikely as the patient denied taking any medications known to induce hypercapnia, such as sedatives or narcotics. There were no apparent neurologic symptoms to suggest a cerebrovascular accident or myositis and radiographic imaging of his brain was normal. Antibodies for myasthenia gravis were negative. Musculoskeletal or chest wall abnormalities were also unlikely. The patient's history of dysphagia and recurrent bronchitis likely secondary to aspiration led to imaging studies that confirmed the diagnosis of DISH causing osteophytic pharyngeal compression.
Mainstay treatment is surgical excision of the osteophyte, allowing for extrinsic decompression of the laryngopharynx and esophagus with potential reversal of airway obstruction and dysphagia. However, large osteophytes can irritate the pharynx and esophagus, causing inflammatory hyperplasia leading to intrinsic compression of these structures. 3 Therefore an osteophectomy without addressing possible intrinsic compression may not fully resolve the airway and esophageal obstruction. Carlson et al conducted a retrospective chart review on patients who underwent osteophectomy and found that six of nine patients were diagnosed with DISH. Of the six, two had airway compromise; one required emergent tracheostomy and the other a concurrent tracheostomy. Both patients were reported to have complete resolution of their airway symptoms post-osteophectomy and underwent successful decannulation. 6
DISH is a rare cause of upper airway obstruction that may manifest as hypercapneic respiratory failure. Consider DISH in the differential diagnosis of hypercapneic respiratory failure when common etiologies have been ruled out and the history and physical exam suggest an upper airway obstruction. Radiologic imaging, such as CT, MRI, and plain radiographs, of the cervical spine is the major diagnostic tool for confirmation of DISH. Laryngoscopy is vital in evaluating for extrinsic compression of the posterior pharyngeal wall causing an upper airway obstruction. Severe airway compression caused extrinsically by a cervical osteophyte can be potentially reversed by osteophectomy however it is important to consider a reactive inflammatory process as a cause for intrinsic obstruction as well.
Disclosures
Consent was obtained from the patient by the authors to reproduce information and photographs appearing in this article. Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.