
Abstract
Primary hypertension in children is increasing in prevalence with many cases likely going undiagnosed. The prevalence is currently estimated at between 3%-5% in the United States and may be higher in certain ethnic groups. Primary hypertension, once felt to be rare in children, is now considered to be about five times more common than secondary hypertension. This review provides information to guide physicians through an organized approach to: 1) screening children and adolescents for hypertension during routine visits; 2) using normative percentile data for diagnosis and classification; 3) performing a clinical evaluation to identify the presence of co-morbidities; 4) initiating a plan of care including subsequent follow-up blood pressure measurements, therapeutic lifestyle changes and pharmacologic therapies.
Introduction
The prevalence of hypertension in children and adolescents has increased in the past several years, likely as a result of the rise in childhood overweight and obesity. The prevalence is currently estimated at between 3%-5% in the United States and may be higher in certain ethnic groups, such as non-Hispanic blacks and Mexican Americans.1–3 This may actually be an underestimate as some experts believe that clinicians fail to recognize high blood pressure in children and adolescents. 3 Unlike in the adult population where absolute cutoffs exist based on observational studies, classification of blood pressure in children and adolescents is based on normative data derived from a national database of 70,000 healthy children in the US. 4
Blood pressure in children is classified as: (1) normal (systolic and diastolic blood pressure [SBP and DBP respectively] <90th percentile); (2) pre-hypertension (SBP and DBP 90th to <95th percentile or exceeding 120/80); (3) Stage 1 hypertension (95th percentile to 99th plus 5 mmHg); and (4) Stage 2 hypertension (>99th percentile plus 5 mmHg) based on sex, age and height on at least three separate measurements. 4 Patients are felt to have “white-coat hypertension” when BP is normal outside a medical provider's office but 95th percentile or greater in the office. Children have hypertension when blood pressures are persistently elevated greater than 140/90 or greater than the 95th percen-tile based on these classifications.
The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents is still the major reference point for recommendations regarding the diagnosis and treatment of hypertension in children and adolescents. 4 In 2009, the European Society of Hypertension released updated guidelines on management of high blood pressure in children and adolescents and used the same criteria to define hypertension as the Fourth Report. 5 The guidelines suggest an emerging role for the use of ambulatory and home blood pressure monitoring in children and adolescents for the diagnosis of hypertension especially in children with isolated clinic hypertension and assessment of response to treatment. 5 Isolated clinic hypertension is defined as blood pressure measurements >95th percentile in the office and <90th percentile in the outpatient setting. 4
Special considerations exist for measuring blood pressure in children and adolescents. In general, children greater than 3 years old should have their blood pressure routinely measured during each health care encounter. Blood pressure should be measured by auscultation as BP normative data was obtained using auscultation and there are many limitations to the use of automated oscillometric devices in children.4,5 A study done after the release of the Fourth Report recommendations involving 390 children at a pediatric hypertension clinic found that 74% of initial readings done at a standard vital sign station were higher (13.2 ± 8.9 mmHg for SBP and 9.6 ± 7.6 mm Hg for DBP) than those obtained in the examination room using protocols established by the Fourth Report. 1 As a result, the authors of this study suggest repeating blood pressures that are initially elevated.
Once the blood pressure is obtained, it should be classified by percentile based on age, sex and height percentile, as determined by the revised CDC growth charts. 4 Because these charts may be cumbersome to use in practice, a simplified table was created to identify cutoffs for children and adolescents needing further evaluation. 6 A more simplified blood pressure table was developed for children ages 3-18 for providers in the outpatient setting by Mitchell et al to improve recognition of pediatric hypertension in the outpatient setting. Blood pressure elevations that exceed these levels should prompt referral to standardized tables to confirm a diagnosis of hypertension. 7 On-line, web-based calculators also exist that can classify blood pressure by percen-tile to quickly and appropriately classify children and adolescents. An example of one online calculator can be found at Baylor College of Medicine Body Composition Lab in Houston, Texas. 8
Although less is known about the long-term consequences of hypertension in children and adolescents, elevated blood pressure in childhood and adolescence is a risk factor for hypertension and cardiovascular disease in adults and may be associated with left ventricular hypertrophy (LVH) at the time of diagnosis. 4 Primary hypertension, once felt to be rare in children, is now considered to be about five times more common than secondary hypertension. Primary hypertension is more common in older children and adolescents and is usually characterized by Stage 1 hypertension. 4 It is commonly associated with a family history of hypertension or cardiovascular disease. 9 Secondary causes of hypertension are more common in children less than 6 years of age and are usually renal or renovascular in origin. 10
Clinical evaluation of confirmed hypertension.

Comorbid risk factors also include diabetes mellitus and kidney disease. Reproduced with permission from Pediatrics, Vol. 114, Page 562, copyright 2004 by the AAP.
Classificiation of hypertension in children and adolescents, with measurement frequency and therapy recommendations.

For sex, age and height measured on at least three separate occasions; if systolic and diastolic categories are different, categorize by the higher value.
This occurs typically at 12 years old for SBP and at 16 years old for DBP.
Parents and children trying to modify the eating plan to the Dietary Approaches to Stop Hypertension (DASH) eating plan could benefit from consultation with a registered or licensed nutritionist to get them started.
More than one drug may be required.
In general, the goal of therapy is to reduce the blood pressure to less than the 95th percentile in children and adolescents with no co-morbidities. 4 Some experts recommend a goal of less than the 90th percentile for this group. 5 In the setting of chronic kidney disease, diabetes or target-organ damage such as LVH, the goal BP is less than the 90th percentile for sex, age, and height. 4 There may be a role for lowering blood pressure below the 75th percentile in patients with proteinuria. 5
Nonpharmacologic management of hypertension includes weight loss, aerobic exercise, restriction of salt intake, and stress reduction.11,12 Overweight increases the risk for the development of hypertension significantly.2,5 Although there is limited evidence, types of aerobic exercise thought to be most beneficial are walking, running, cycling, or swimming. The high degree of patient and family commitment required may limit their effectiveness. 13 During aerobic exercise, peripheral vascular resistance decreases, causing an increase in systolic blood pressure (SBP) and mean arterial pressure (MAP) and a reduction in the diastolic blood pressure (DBP); however, in static exercise such as weight lifting, the SBP, DBP, and MAP increase significantly and can exceed the values for aerobic exercise. There are usually both components in exercise so participation should only be granted when the demands for training and participating in the activity have been examined and determined that the child is not at risk for a catastrophic event from an abrupt increase in BP. 11 The preparticipation physical evaluation working group recommends those with Stage 2 hypertension avoid heavy weight and power lifting, bodybuilding, strength training and other high-static component sports. Those with sustained Stage 1 hypertension need individualized evaluation prior to participation. 14
The Dietary Approaches to Stopping Hypertension, or DASH diet, is recommended although its effectiveness in children and adolescents with essential hypertension has not been extensively studied. 15 The diet emphasizes the intake of fruits, vegetables, low-fat dairy and whole grains and limits intake of high fat foods and refined sugar. It has been shown to be effective in adults to reduce blood pressure and has no real side effects. 12 One study did review incorporation of the DASH diet in children with diabetes and hypertension and demonstrated a substantial reduction in the propensity of Type 1 diabetic children to have hypertension but this was not observed in those with Type 2 diabetes. 16 Most of the children with Type 2 diabetes were obese in the study which may explain the lack of improvement in this population.
While these therapies may be effective in reducing the blood pressure to the targeted levels, pharmacologic therapy will need to be considered if they do not. The etiology of the hypertension, the anticipated benefits for the child, and the potential adverse effects should guide the choice of medication.4,17 Given the lack of long-term pediatric data on benefits of therapy and adverse effects on growth and development, medications should be started cautiously. 18 First line antihypertensive medications for children include angiotensin-converting enzyme inhibitors (ACEIs), angiotensin receptor blockers (ARBs), calcium channel blockers (CCBs), beta-blockers (BBs) and diuretics. Treatments specific for secondary causes of hypertension and severe hypertension are beyond the scope of this article. Hypertension will refer to essential or primary hypertension for the remainder of the article unless specified otherwise.
Mechanism of Action, Metabolism, and Pharmacokinetic Profile
Most pharmacokinetic data for children has come from adult trials. With the passage of the Food and Drug Administration Modernization Act in 1997, there has been an increase in pharmaceutical-sponsored trials evaluating antihypertensive medications in children. This was reinforced with The Best Pharmaceutical for Children Act passed in 2002 and expanded by the Pediatric Research Equity Act passed in 2003 requiring all applications for new drugs to include pediatric assessment data unless the pharmaceutical company obtained a waiver or deferral. 12
Angiotensin-Converting Enzyme Inhibitors and Angiotensin Receptor Blockers
ACEIs are one of the most commonly used antihy-pertensive medications in the pediatric population. In general, they have few adverse effects in standard doses and have convenient dosing schedules to improve adherence. This makes them attractive choices for pediatric hypertension especially in adolescents. 19 Angiotensin-converting enzyme (ACE) facilitates the conversion of angiotensin I to angiotensin II and the degradation of bradykinin. Angiotensin receptor blockers (ARBs) selectively inhibit the binding of angiotensin II to the angiotensin II type 1 receptors. 19
Angiotensin II produces arterial vasoconstriction and activation of the renin-angiotensin system promoting salt and water reabsorption in the distal tubules mediated by aldosterone. Angiotensin II also stimulates the sympathetic nervous system and has a direct inotropic effect on the heart. Bradykinin produces vasodilatation via prostaglandin-mediated effects on endothelial cells. ACEIs prevent the conversion of angiotensin I to angiotensin II which reduces arterial vasoconstriction and the salt and water retention facilitated by stimulation of aldosterone release by angiotensin II and with reduced degradation of bradykinin, arterial vasodilation. Blood pressure falls gradually until ACE is inhibited by 90% rather than in a dose response effect.20–23 Angiotensin II produces vasoconstriction at both the afferent and efferent arterioles with preferential increases at the efferent arteriole; therefore ACEIs increase blood flow to the kidney despite lowering blood pressure. Additionally, the sulfhydryl group present on captopril is thought to have an anti-inflammatory effect. 24 ACEIs are separated by their route of elimination, presence of a sulf-hydryl group, and requirement for activation. 20
Calcium Channel Blockers
Calcium channel blocking antihypertensives inhibit the influx of extracellular calcium into the cellular membrane of the smooth muscle and other contractile cells by blocking the transmembrane transport of calcium. This results in reduced contractility and arteriolar smooth muscle tone in a dose-dependent fashion. Dihydropyridines are the major class of CCBs used to treat essential hypertension in children because of their relative selectivity for arteriolar smooth muscle. These include amlodipine, isradipine, and nifedipine. The non-dihydropyridines, another class of CCBs that includes verapamil and diltiazem, have greater affinity for cardiac cells thus reducing contractility and altering conduction at the sinus node pacemaker and atrioventricular node respectively. Additionally, increases in glomerular filtration rate (GFR) and renal blood flow occur with therapy presumably related to the reduction in renal vascular resistance.11,19-21,23 Non-dihydropyridines are rarely used for the treatment of essential hypertension in children and adolescents because of their effects on cardiac functioning. 22
Beta-Blockers
Beta-adrenergic antagonists reduce the effect of endogenous catecholamines on beta-adrenergic receptors. There are three identified types of receptors designated β1, β2, and β3. β1-adrenergic receptors are found primarily in the heart and kidney; β2-adrenergic receptors are located in multiple areas particularly the lung, vascular smooth muscle, and skeletal muscle; and β3-adrenergic receptors are located in adipose tissue. 21 In general, BBs competitively block β 1 -adrenergic receptors and β2-adrenergic receptors dependent upon the selectivity of the individual drug. 19 These medications are separated by several characteristics, including cardioselectivity, alpha adrenergic activity, hydrophilic and lipophilic properties and intrinsic sympathomimetic activity. Assessment of these properties can be useful in selecting the appropriate BB for use in a particular patient. 11
Included in this category are BBs that also have α-adrenoreceptor blocking properties. They exert their effect primarily by competitive blockade of peripheral post-synaptic alpha1-receptors producing vasodilation.19–21 Nonselective beta-blocker use has been associated with development of diabetes in contrast to the cardioselective β-antagonists. 25
Diuretics
Diuretics are used primarily as a second medication when adequate blood pressure has not been attained with monotherapy especially in adolescents and in children with renal disease with high volume states. The two types primarily used are thiazide and loop diuretics. Thiazide diuretics exert their effect on the distal tubule in the kidney to decrease sodium and water reabsorption and increase potassium secretion in an ion exchange mechanism by inhibiting the sodium-chloride membrane transporter. With long term use, the thiazides produce vasodilatation. Although the mechanism of action is not thoroughly understood, it is postulated it may be due to a decrease in interstitial volume, a decrease in intracellular sodium that alters intracellular calcium, or a change in cellular receptors to vasoconstrictor substances. Therefore, initial blood pressure reduction appears to occur due to a decrease in plasma volume and cardiac output and then occurs due to a reduction in peripheral resistance. Their efficacy is dependent on the glomerular filtration rate (GFR). They are most efficacious when the GFR is >50 ml/minute and ineffective when the GFR is <30 ml/minute.19–21 Thiazide diuretics produce elevations in blood glucose and insulin levels. 26
Loop diuretics exert their effect at the ascending limb of the loop of Henle by decreasing the reabsorption of sodium and water by inhibiting the sodium-potassium-chloride membrane transporter. They also increase renal blood flow by reducing renovascular resistance. They are more potent than thiazide diuretics but their efficacy also decreases as GFR is reduced.19,20
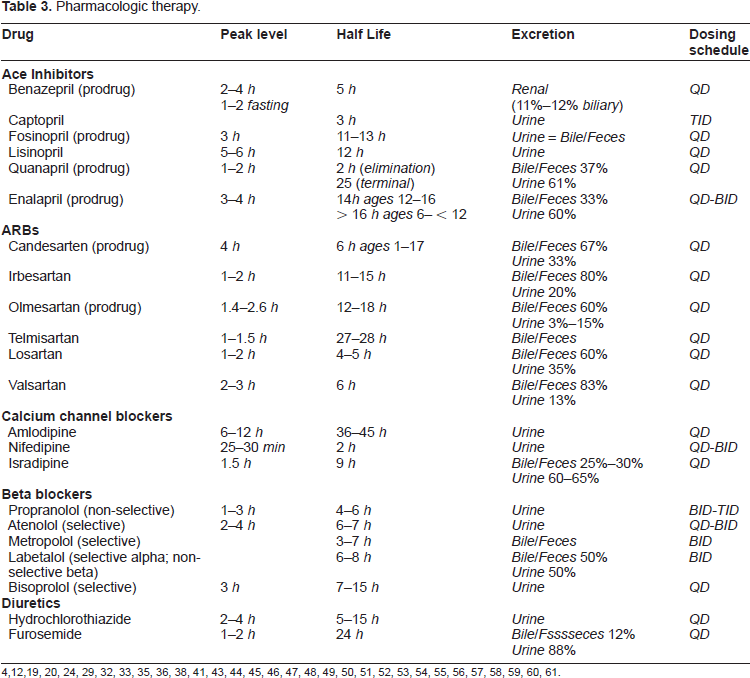
Pharmacologic therapy.
4, 12, 19, 20, 24, 29, 32, 33, 35, 36, 38, 41, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61.
Clinical Studies, Safety and Efficacy
Angiotensin Converting Enzyme Inhibitors
Safety and efficacy data are available for most of the ACEI. Enalapril and lisinopril both produce a dose-dependent reduction in blood pressure. Minimum effective dosages range from 0.08 mg/kg/day to 0.6 mg/kg/day and were well tolerated.12,27,28 However, fosinopril did not produce the same dose response reduction in blood pressure as that seen in the enalapril and lisinopril studies, but did demonstrate a significant reduction in SBP and DBP. The study participants were ages 6-16 years of age. Fosinopril is only recommended for children weighing $50 kg.12,29 Ramipril studied in children with chronic renal disease reduced the BP at 24 hours at a daily dose of 6 mg/m2 and at a dose of 2.5 mg/m2 reduced BP and proteinuria in children with essential hypertension and in those with chronic kidney disease. 5
Common side effects associated with ACEI medications include hypotension, cough, hyperkalemia and elevated creatinine. Monitoring of serum electrolytes and creatinine are recommended with initiation of therapy and periodically to monitor the potassium and creatinine.
Other adverse reactions include angioedema, headache, anemia, tachycardia, vertigo, dyspnea, rash, and leucopenia.27,28 One study found that children between 2-16 years of age receiving enalapril or captopril developed neutrophilic hypersegmentation. 30 One retrospective study of lisinopril found no effect on age-specific growth patterns despite the varying medical conditions of the participants. 28 A meta-analysis of studies evaluating ethnic differences in children treated with ACEI suggested a difference between black and white children to the antihypertensive effects of ACEI. Black children demonstrated a lesser antihypertensive response than white children. 31 ACEI are contraindicated in patients with bilateral renal artery stenosis.
Infants have an exaggerated response to ACEIs and should receive smaller weight-adjusted dosages than older children. This may be related to their dependence on the renin-angiotensin-aldosterone system for maintenance of renal blood flow. They can have severe, prolonged hypotension with oliguric renal failure. 27 In a study with children at least 6 months of age, captopril was given in dosages of 0.5, 1.0, and 2.0 mg/kg. Reductions in SBP and DBP were similar and independent of dosage; therefore, a dosage of 0.5 mg/kg is recommended as the starting dose in children ≥6 months of age. 21 ACEI should be avoided in pregnancy and used cautiously in those of child-bearing age. ACEI exposure during the first trimester can result in major congenital malformations. Exposure during the second and third trimesters is associated with fetal hypotension, growth restriction, pulmonary and renal hypoplasia, anuria, and death.11,27
Angiotensin Receptor Blockers
Several studies have demonstrated the efficacy of ARBs in the treatment of hypertension in children. In a systematic review, the ARBs irbesartan, candesartan, and losartan lower SBP and DBP, 10.5 mmHg and 6.9 mmHg respectively. They decrease proteinuria by over 50% as well. Losartan reduced DBP in a dose dependent fashion at doses from 0.75 mg/kg/day to 1.44 mg/kg/day and was well tolerated. A small irbesartan study indicated that doses of 75-150 mg/day were efficacious in the treatment of hypertension but a later study in children ages 6-16 years failed to show a significant antihypertensive effect.5,12,32 In the Assessment of Efficacy and Safety of Olmesartan in Pediatric Hypertension (AESOP) study, two groups of children ages 6-16 years of age were enrolled and given either low-dose (2.5-5 mg) or high dose (20-40 mg) Olmesartan daily for three weeks. Both groups demonstrated statistically significant reductions in SBP and DBP but much greater in the high-dose group. 33 Valsartan demonstrated efficacy in reducing blood pressure in children aged 1-5 years. During this study conducted in four phases, the children were randomized to receive low-dose, medium-dose, or high-dose valsartan. The fourth phase was a 52 week open label treatment period. Valsartan significantly lowered SBP and DBP in all of the dosage groups regardless of race or weight. During the open-label phase, participants received either valsartan alone or combined with hydrochlorothiazide. By the end of the period, >75% achieved a SBP less than the 95th percentile.34,35 Telmisartan at dosages of 1-2 mg/kg produced significant reductions in SBP in children ages 6 to <18 years of age. 36
Generally, ARBs are well tolerated. Side effects reported included cough, rhinitis, urinary and gastrointestinal infections, headache, dizziness, blurred vision, fatigue, anemia, and hyperkalemia. 32 Other adverse reactions reported include rash and pruritus, hypertriglyceridemia, edema, leucopenia, and thrombocytopenia. 34
The same precautions should be taken in pregnancy and in women of child-bearing age as with ACEI. Similar congenital malformations seen with ACEI exposure during pregnancy have been reported. 32 Studies involving candesartan, losartan, and valsartan showed no effect on growth during study periods of 52 weeks for each.32,34
Calcium Channel Blockers
The major class of CCBs used in the treatment of pediatric hypertension is the dihydropyridines because of their rather selective action on arteriolar smooth muscle. 11 Amlodipine, nifedipine, felodipine, nicardipine, and isradipine have shown efficacy in treating hypertension in children. 20 Several trials have studied the efficacy of amlodipine in the treatment of pediatric hypertension. In one study, dosages of 0.06-0.34 mg/kg/day effectively reduced SBP in children ages 6 to 16. 5 In a prospective study evaluating amlodipine, 21 children were given dosages based on weight: 5 mg/kg/day for children >70 kg; 2.5 mg/kg for those 50-70 kg; and 0.05 mg/kg for those <50 kg. Dosing was once daily. The 16 children with primary hypertension reached their target BP of <95th percentile for age, weight, and gender. 21 Long-acting nifedipine might be an option in older children that can swallow tablets but it cannot be crushed; therefore, its use is limited in young children. 21 Nicardipine is similar to nifedipine except it does not affect cardiac function. Typically nicardipine and isradipine are delivered by continuous intravenous infusion because of their short half-lives. They can be rapidly titrated to a desired BP. 27 A mean effective nicardipine dose of 1.8 ± 1.0 μ/kg/min achieved a 16% drop in SBP, 23% in DBP, and a 7% increase in heart rate within 2.7 ± 2.1 hours after initiation. 37 However, the oral preparation of isradipine was given to 12 children over a three year period. There were 6 boys and 6 girls, ranging in age of 10 months to 11 years. Initial doses were given at 0.1 mg/kg for all children and increased every 3-6 doses until the SBP and DBP were reduced to two standard deviations for their age. Dosing was either every 6 or 8 hours per day. The SBP was reduced 20% and the DBP 28% from initial parameters at doses of 0.6 ± 0.3 mg/kg/day. As with nicardipine, isradipine causes cerebral vasodilation and must be used cautiously in children with intracranial pathology if at all.27,38
The most common adverse side effects reported with the use of CCBs include peripheral edema, dizziness, flushing, nausea, headache, and postural hypotension. Other reported adverse events include gingival hyperplasia, chest pain, nausea and vomiting, and reflex tachycardia seen with nifedipine. Side effects are seen more commonly as maximum dosages of the drugs are reached.11,21,27
Beta-Blockers
There are limited studies evaluating BBs in children. Additionally, the variability of pharmacologic properties of drugs in this group and characteristics of each individual drug influence the selection of medication. There are few studies evaluating propranolol, a nonselective beta-blocker, as an antihypertensive in children. It has been used to treat hypertension for several years with much of the data extrapolated from studies in normotensive children with cardiac disease or portal hypertension. 5 Effective dosages range from 1 to 6 mg/kg/day. In one study of 11 children ages 7 months to 16 years receiving 2.5 mg/kg/day, SBP was reduced by an average of 26 mmHg and DBP by an average of 20 mmHg.19,21 Atenolol, metoprolol, and bisoprolol are more cardioselective beta adrenergic antagonists. Atenolol is a β1-selective adrenergic antagonist that can be dosed once daily with recommended doses of 1-2 mg/kg/day. It is as potent as propranolol when compared on a weight-by-weight basis and has demonstrated efficacy in adolescents.19,24 Metoprolol succinate in an extended release preparation and was studied in two phases, a 4 week treatment period and an open-label maintenance period for 52 weeks in children ages 6-16 years of age. Metoprolol is cardioselective but has no intrinsic sympathomimetic activity. The greatest reduction in SBP occurred at a dose of 1 mg/kg and for DBP; reductions were greatest at 2 mg/kg compared to placebo. Results were seen independent of age, race, sexual maturity, or gender. More overweight children had a somewhat reduced response. 39 Metoprolol reduces the blood pressure and heart rate response in exercise and reduces the sympathetic responses to mental stress but does not impact endurance. 21 Bisoprolol fumarate was studied in combination with hydrochlorothiazide (HCT) in children ages 6-17 years of age with Stage 1 hypertension over an eight week period. The group receiving the β1-cardioselective beta blocker in combination with the thiazide (HCT) diuretic achieved a reduction in SBP of 6.8% and DBP of 8.5% but those that reached the target BP <90th percentile were not significantly different from placebo (45% vs. 34%). Unfortunately there was also a significant placebo and dropout rate in this trial. 40 Labetalol possesses additional properties besides beta blockade. Labetaolol is not cardioselective, has no intrinsic sympathomimetic properties, but has significant α-adrenergic blockage. The ratio of α to β blockade is estimated at seven to one. It has been used both orally and intravenously for severe hypertension. 20 The α-adrenergic blockade counteracts the increase in systemic vascular resistance caused by β 2 -antagonism. In a trial of 27 boys evaluating labetalol infusion for hypertensive crisis in children ≤24 months of age, labetalol produced a mean BP reduction of 20% within 8 hours. 41 Similar results were obtained in children unable to tolerate oral medications that were administered labetalol by infusion. 19
Side effects attributable to propranolol include bradycardia, hypoglycemia, anorexia, asthma exacerbations, night terrors, and heart block.19,21 The most common side effects noted in the metoprolol succinate and bisoprolol trials were headache but other side effects reported were fatigue, upper respiratory tract infection, cough, nasopharyngitis, diarrhea, and dizziness.39,40 Labetalol can produce orthostatic hypotension and syncope because of reduction in the peripheral vascular resistance. 20
Additional side effects attributable to BBs include fatigue, cold extremities, and sexual dysfunction. 20 Lipophilic BBs exert more central nervous system side effects and β1-selective blocking agents have less adverse effects on the lungs. 24
Diuretics
There is a paucity of studies examining the use of diuretics for essential hypertension in children. In one study of 12 children ages 3-15 years involving chlorthalidone, statistically significant decreases in SBP and DBP occurred. High dose hydrochlorothiazide (50-100 mg) compared to clonidine improved BP in adolescents but not to the degree of the comparison medication. 20 Thiazide diuretics are more commonly used as adjunct therapy when monotherapy has failed to achieve the desired BP targets because of their synergistic effects with other antihypertensive medication. They particularly are recommended for adolescents in combination medications to improve adherence. 5 Thiazide diuretics are ineffective when the GFR is <30% from normal levels. 21
Safety and monitoring of phamacologic therapy.

4, 11, 20, 21, 27, 42
Place in Therapy and Patient Preference
There are no adequate trials of antihypertensive medications in children that compare the effectiveness of specific antihypertensives or classes of antihypertensives on key clinical endpoints. 4 Since pediatric trials do demonstrate the ability of these medications to lower blood pressure, the choice of specific agent is left to the discretion of the physician who should take into account patient preferences as well as other clinical considerations. The ability of the patient to swallow pills, ease of dosing and risk of pregnancy should be considered. Certain co-morbidities that favor certain classes of drugs include the use of an ACE or ARB in patients with diabetes and microalbuminuria or proteinuric renal disease. Beta-blockers and calcium channel blockers should be considered in patients with migraine. In general, black children and adolescents do not respond as well to ACEIs at standard doses. 31 Beta-blockers must be used with caution or avoided in patients with asthma and a reliable method of birth control must be in place for sexually active adolescents on ACEs or ARBs. Cough does not appear to limit the use of ACEs or ARBs in children and adolescents as it does in adults. 42
In general, the child or adolescent should be started on the lowest recommended dose for the specific medication and it should be titrated up, typically every 2-4 weeks, until target BP is reached or side effects limit its use.4,5 After maximum doses are reached, a second drug can be added if the BP is still not at goal. 4 The European guidelines recommend switching to another class of drugs as an alternative approach if goal BP is not achieved at maximum doses of a single agent. 5
The Fourth Report recommends that consideration should be given to using a second agent with complementary actions to the first. Examples include ACE inhibitors and diuretics, or a vasodilator with a diuretic or beta-blocker. There is limited data and practical experience with use of fixed-dose combination medications. 4 Children and adolescents may be considered for step-down therapy if blood pressure remains well controlled, especially if they achieve significant weight loss.
Conclusion
Primary hypertension in children is increasing in prevalence with many cases likely going undiagnosed. Physicians need to screen children and adolescents for hypertension during routine visits and use normative percentile data for diagnosis and classification. Providers can consider referral for ambulatory blood pressure monitoring to check for possible white coat hypertension. Once the diagnosis is made, a clinical evaluation must be performed to identify the presence of co-morbidities. Subsequent follow-up blood pressure measurements, therapeutic lifestyle changes and pharmacologic therapies are indicated based on the stage of the disease. The goal of therapy is to reduce blood pressure to at least <95% in patients without comorbidities and <90% in the presence of CKD, DM and target organ damage. Several non-pharmacologic management strategies exist for the treatment of primary hypertension and when they are not effective, pharmacologic treatment needs to be considered. The choice of a specific agent should take into account clinical considerations and patient preferences. ACE inhibitors or ARBs are useful in children, especially those with diabetes or kidney disease with proteinuria. Calcium channel blockers are also a good option in patients with diabetes or metabolic syndrome because they improve insulin sensitivity. Diuretics are also reasonable choice, although may not be as effective as monotherapy. Beta-blockers should usually be saved for second-line therapy given their side effect profiles, but consider them for children and adolescents with an additional indication such as migraines or tachycardia. In general, physicians should start with the lowest recommended dose and titrate every 2-4 weeks. If target blood pressure is not reached, physicians can switch to a new agent or add a complementary agent.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.