
Abstract
Acute exacerbations of COPD (AECOPD) are major clinical events. They are associated with a more rapid decline in lung function, poorer quality of life scores, and an increased risk of dying. Exacerbations that require hospitalization have particular significance. Approximately 40% of the AECOPD patients who require hospitalization will die in the subsequent year. Since many AECOPD require hospitalization, they account for most of the expense of caring for COPD patients. Treatment with long-acting bronchodilators and combination inhaled corticosteroid/long-acting bronchodilator inhalers reduces but does not eliminate AECOPD. Roflumilast, a selective phosphodiesterase 4 (PDE4) inhibitor, is an anti-inflammatory medication that improves lung function in patients with COPD. In patients with more severe airway obstruction, clinical features of chronic bronchitis, and a history of AECOPD, roflumilast reduces the frequency of AECOPD when given in combination with short-acting bronchodilators, long-acting bronchodilators, or inhaled corticosteroids. It is generally well tolerated but the most common adverse effects include diarrhea, nausea, weight loss, and headaches. In clinical trials, patients treated with roflumilast experienced weight loss that averaged just over 2 kg but was primarily due to the loss of fat tissue. Weight loss was least in underweight patients and obese patients experienced the greatest weight loss. An unexpected benefit of treatment with roflumilast was that fasting blood glucose and hemoglobin A1c levels improved in patients with comorbid type 2 diabetes mellitus. Roflumilast, the first selective PDE4 inhibitor to be marketed, is a promising drug for the management of COPD patients with more severe disease.
Introduction
Chronic obstructive pulmonary disease (COPD) is the comprehensive term used to describe the variable amounts of emphysema, chronic bronchitis, and small airway disease that develop as a consequence of exposure to cigarette smoke and other forms of air pollution. 1 In the developing world, smoke from the burning of biomass for cooking and heating is the other most common cause of COPD.1,2 COPD is characterized by a different pattern of pulmonary inflammation than asthma. The primary inflammatory cells in the airways of asthma patients are CD4+ T lymphocytes and eosinophils whereas in COPD, the predominant inflammatory cells are CD68+ macrophages, CD8+ T lymphocytes, and neutrophils, especially during exacerbations. 4 These inflammatory changes contribute to airway swelling, luminal narrowing and a reduction in airflow. 5 Airway mucus gland hyperplasia results in mucus hypersecretion that contributes to cough and sputum production and to the further impairment of airflow. The associated parenchymal destruction, called emphysema, reduces elastic recoil further diminishing airflow.
The severity of inflammation increases with more severe airway obstruction.3,5 In COPD patients, elevated blood leukocyte counts are common suggesting that inflammation extends systemically from the lungs. 6 Fibrinogen and C reactive protein concentrations may be elevated in the circulation of COPD patients. 6 Concentrations of proinflammatory cytokines including tumor necrosis factor-α (TNF-α), leukotriene B4 (LT B4), interleukin-1β (IL-1β), IL-6, and IL-8 are also increased in COPD patients.6,7 Bronchial epithelial cells, CD8+ T lymphocytes, and CD68+ macrophages produce IL-32, contributing to increases in the levels of TNF-α, IL-8 and CXCL 2. 6 Blood levels of IL-32 are inversely related to FEV1, and increase with the severity of airflow obstruction in COPD patients. 7
Despite therapeutic advances that have improved survival, symptoms, and quality of life, COPD remains a major cause of disability and death. Increased smoking rates in the developing world will make COPD the 3rd most common cause of death worldwide by the year 2020. 1 The longitudinal 3 year ‘Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points’ (ECLIPSE) study found that patients with COPD experience more shortness of breath and have poorer quality of life scores than smokers with normal lung function. 8 They are also more susceptible to a variety of comorbid illnesses including heart and cardiovascular disease, anemia, osteoporosis, diabetes, muscle mass loss, and depression than either smokers without airway obstruction or normal subjects. 9 One hypothesis proposes that inflammation extends systemically from the lungs contributing to the comorbidities but which, if any, of the inflammatory markers are predictive of the relationship between these illnesses and COPD is unclear. 10
Acute Exacerbations of COPD
Acute exacerbation of COPD (AECOPD) is the term used to describe a flare-up of the condition. They are important clinical events and have prognostic significance. 1 They interfere with normal activity and both moderate and severe AECOPD require treatment with antibiotics and/or systemic corticosteroids. 10 Complete recovery from an AECOPD may take weeks to months. Exacerbations are associated with worse quality of life scores and with a more rapid decline in lung function.11,12 More severe AECOPD result in hospitalization accounting for the majority of health care costs associated with COPD. In Canada, AECOPD account for more hospital days than myocardial infarction, congestive heart failure, or pneumonia. 13 In 2008, patients hospitalized with an AECOPD in Canada spent an average of 10 days in hospital at an average cost of approximately $10000 per hospitalization. 13 In-hospital mortality rates range from 2.5% to 14% and average 7% in patients with an AECOPD. 14 The heightened risk of mortality associated with AECOPD extends beyond the period of hospitalization. As many as 40% of AECOPD patients requiring hospitalization will die in the subsequent 12 months. 15 A more recent Canadian study found that patients discharged after an AECOPD have a poor prognosis with approximately 30% dying in the subsequent 12 months. 16
The ECLIPSE Study
The results of a large, 3 year longitudinal study of COPD patients and two control groups; normal nonsmokers and smokers without COPD, are being reported in a series of publications. 8 In the ECLIPSE study, patients with more severe COPD experience more frequent AECOPD. 17 However, there are wide ranges in AECOPD frequency across the different GOLD stages. Some patients with moderate COPD, GOLD stage II disease, experienced frequent AECOPD and some with very severe COPD, ie, GOLD stage IV with a FEV1 less than 30% of the predicted value, did not experience any AECOPD during the three year prospective study. A patient's AECOPD history predicts what happens to them subsequently. During the ECLIPSE study, patients with a history of frequent, ie, two or more per year, AECOPD were more likely to continue to experience frequent AECOPD and those without a history of frequent AECOPD were unlikely to experience frequent AECOPD. 17 Patients with more frequent AECOPD had poorer quality of life scores. 17
Chronic Bronchitis
Chronic bronchitis is defined clinically as an almost daily productive cough for a minimum of three months for a minimum of two consecutive years. Patients with chronic bronchitis are at greater risk for poor outcomes than other COPD patients with similar degrees of airway obstruction. 18 Airway inflammation is greater in patients with the chronic bronchitis clinical phenotype. 19 There is also evidence that they experience a more rapid decline in lung function than other COPD patients.20,21 Although not reported in the ECLIPSE study, other investigators have reported that patients with chronic bronchitis experience exacerbations more frequently and a have higher death rate. 18
AECOPD
Potential causes of AECOPD include air pollution, allergen exposure, heart failure, and pulmonary emboli, but the majority are triggered by bacterial or viral infections.
10
Many COPD patients are chronically colonized with bacteria, primarily
Treatment of AECOPD
Antibiotics have been used to treat AECOPD for over 50 years despite numerous studies in the 1950s, 1960s, and 1970s failing to confirm their benefits.
24
Anthonisen and colleagues recognized that β error, ie, earlier studies did not recruit enough subjects to consistently demonstrate their effectiveness, was responsible and that a properly powered study might confirm the impression of most clinicians that antibiotics are advantageous in AECOPD. They designed a study that randomized patients with AECOPD to treatment with antibiotics, cotrimoxasole, doxycycline, or ampicillin, or to placebo.
25
Those treated with antibiotics had a 68% treatment success rate compared to 55%, (
Systemic corticosteroids are also beneficial in AECOPD. Aaron and colleagues randomized patients discharged from the emergency room to receive either prednisone 40 mg daily for 10 days or placebo. The relapse rate was 27% in the corticosteroid-treated patients compared to 43% in the placebo-treated group (
Prevention of AECOPD
The inflammatory changes associated with AECOPD contribute to symptoms and require time to recover. Corticosteroids are anti-inflammatory but have greater activity against CD4+ T lymphocytes and eosinophils, than on the predominant inflammatory cells in COPD; CD8+ T lymphocytes, CD68+ macrophages and neutrophils.3,7 Other strategies, including the introduction of novel medications with greater activity against the predominant inflammatory cells in COPD, will likely further reduce both the frequency and severity of AECOPD.
Obvious strategies include the prevention of COPD by smoking cessation and controlling air pollution, and the development of more effective medications to improve pulmonary function, reduce the rate of pulmonary function decline, and to prevent AECOPD. Moderate AECOPD are usually defined as increases in, or the new onset of cough, increased sputum production, increased sputum purulence, wheezing or dyspnea, or various combinations of these symptoms requiring treatment with antibiotics, oral corticosteroids, or both.27,28 Severe AECOPD are defined as those requiring hospitalization or resulting in death. 28 Several treatment options reduce the number or frequency of AECOPD and the number of AECOPD requiring hospitalization. Recent studies have found that treatment with tiotropium, combination inhaled corticosteroid (IHCS)/long-acting β2 agonist (LABA) inhalers, and treatment with tiotropium and combination IHCS/LABA inhalers reduce the number of AECOPD; especially in those with more advanced disease. 28 33
Uncertainty persists about the role of IHCS in COPD. Treatment with IHCS is not beneficial in patients with mild COPD.34,35 However, studies in patients with more severe COPD suggested that IHCS were beneficial.36,37 A meta-analysis of the IHCS treatment trials concluded that IHCS reduced all cause mortality by approximately 25%. 38 The study design and analysis of these trials have been criticized and their validity contested. 39 In some studies, the majority of patients were receiving IHCS prior to entering the trials. The apparent benefits of IHCS on the AECOPD rate increased with the proportion of patients taking IHCS prior to randomization. 39 Many of the patients previously treated with IHCS were randomized to the placebo arm and so their outcomes actually represent the effects of IHCS withdrawal, shown previously to adversely affect outcomes in severe COPD, and contributed to an overestimate of the apparent benefits of IHCS therapy.39,40 Another concern with these studies is that patients who withdrew prematurely were not always followed to the end of the trial potentially biasing the intent-to-treat analysis. 39 Some studies did not employ a weighted Poisson regression model and underestimated variability. 39 Consequently, the 95% confidence intervals were under estimated, falsely attributing statistical significance to the results. 40
A retrospective patient database analysis demonstrated that hospitalized AECOPD patients who received an IHCS prescription within three months of discharge had lower mortality rates and lower rates of rehospitalization. 42 Patients who were rehospitalized or died prior to filling an IHCS prescription were included in the non-IHCS group biasing the results. By including those with a poorer outcome in the non-IHCS group, the apparent benefits of IHCS therapy were exaggerated. 43 This source of error is called immortal time bias. 44 In a subsequent study of newly diagnosed COPD patients, bronchodilator users were compared to IHCS users to avoid immortal time bias influencing the results. 45 In this study, mortality was not less in the IHCS treated-patients. 44 Another concern is that treatment with IHCS may increase the risks of pneumonia and possibly also of tuberculosis in COPD patients.46,47 Current COPD guidelines recommend against the use of IHCS monotherapy because of doubts about their efficacy and their potentially serious side effects. 4
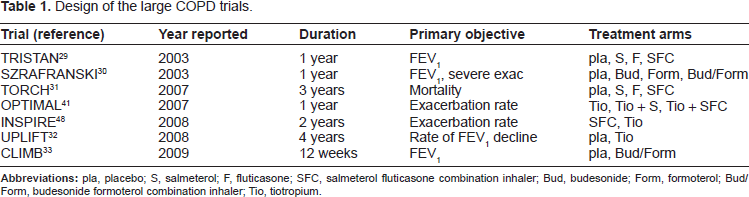
Design of the large COPD trials.
Demographics of the large COPD trials.

In the randomized, placebo-controlled UPLIFT trial, daily tiotropium for 4 years was added to the regular treatment regimen of COPD patients. 32 Improvements in pulmonary function, respiratory symptoms, and quality of life were reported in the tiotropium-treated patients. The rate of lung function decline was the primary objective so final outcomes were assessed one month after the end of the trial to allow for an adequate washout period. 32 Mortality was reduced at the end of the trial in the tiotropium-treated patients but the difference was no longer evident one month later. 32
The combined rate of moderate and severe AECOPD was reduced by 14% in the tiotropium study arm. The reduction in AECOPD was less than in the combination IHCS/LABA inhaler trials but the treatment arms in the combination inhaler trials were compared to placebo whereas in UPLIFT, tiotropium was added to regular treatment which often already included LABA, IHCS or combination IHCS/LABA therapy.31,32
An obvious question is whether combination of the three classes of inhaled medications, long-acting anti-cholinergics (LAAC), IHCS, and LABA is superior to LAAC monotherapy, or to a combination of LABA and LAAC. 41 A government agency-funded study incorporated an intent-to-treat analysis and a weighted Poisson regression model to account for all sources of variability to compare these treatment options in a double-blinded, randomized, three-arm trial. 41 The combination of three classes of inhaled medications, LAAC, LABA, and IHCS, did not reduce AECOPD compared to tiotropium, the primary objective of the study, but triple combination therapy reduced severe AECOPD requiring hospitalization and improved both pulmonary function and quality of life scores. 41 Subsequently, an industry-sponsored study compared the addition of budesonide/formoterol or placebo to tiotropium treatment and showed that the combination of the three types of inhaled medications reduced the number of AECOPD requiring treatment with systemic corticosteroids. 33
There are several important caveats when considering these treatment trial findings. Most importantly, the majority of patients in these trials had GOLD stage III or GOLD stage IV disease, ie, a FEV1 less than 50% of predicted or less than 30% of predicted, respectively. 1 It is unclear whether the results are applicable to patients with milder disease. Anywhere from 25% to 30% of the patients in the treatment arms and more than 40% in the placebo arms failed to complete the protocol in these studies.29–33,41 Since an intent-to-treat analysis was usually employed, patients leaving the study prematurely were often treated with another regimen resulting in distortion of the results.42,48 Since more patients left the placebo than the treatment arms and were subsequently treated with the medications that they were supposed to be compared to, the benefits of therapy may have been underestimated. 42
The studies were designed to include a high risk group at baseline so that the intervention could demonstrate a benefit. Most patients in the larger treatment trials had GOLD stage III or stage IV disease and at least one AECOPD in the year prior to entering the treatment trial. The treatment interventions demonstrated clinically important benefits including a reduction in the number of moderate and severe AECOPD but patients in the treatment arms still experienced an average of nearly one AECOPD per year.29–33,41,49 Considering their clinical importance, the development of medications to further reduce the rate of AECOPD and their consequences is essential. A variety of different medication classes are currently undergoing study for treatment of COPD. 7
Theophylline, a Nonselective Phosphodiesterase Inhibitor
Theophylline has been used since the 1930s for the treatment of asthma and COPD.50,51 It is a nonselective phosphodiesterase inhibitor with several potentially important actions including bronchodilation, enhancement of skeletal muscle contractility, and it is a CNS stimulant.50,51 Phosphodiesterase hydrolyzes the 3′-phosphodiester bond in cyclic nucleotides terminating their activity. 52 Theophylline has other effects including adenosine antagonism and histone deacetylase activity restoration. 50 More recently, anti-inflammatory effects have been recognized that may be important in COPD and asthma. 51 Disadvantages include its narrow therapeutic window and potentially life-threatening and difficult-to-treat adverse effects including nausea and vomiting, cardiac arrhythmias, and CNS stimulation and seizures. Theophylline overdoses are notoriously difficult to manage and severe ones may require charcoal haemoperfusion dialysis. It is metabolized via the hepatic P 450 cytochrome enzyme pathways and drug interactions can affect serum levels of theophylline and a variety of other medications, either reducing their activity or increasing the risk of toxicity. Theophylline levels have to be measured periodically to insure a therapeutic effect and to avoid toxicity.
Selective PDE Inhibitors
Eleven families of PDE isozymes have been identified and their distribution varies in different types of cells.53,54 Selective inhibitors of PDE5 relax vascular smooth muscle and have been very successfully marketed as treatments for erectile dysfunction and more recently as treatment for pulmonary hypertension. 55
PDE4 Inhibitors (PDE4i)
Adenylcyclase catalyzes the conversion of ATP to cyclic adenosine 3’,5′-monophosphate (cAMP). Cyclic AMP is an important intracellular signal for a diverse array of neurotransmitters, hormones, cytokines and medications that stimulate membrane-bound adenyl cyclase. 52 Phosphodiesterase (PDE) catalyzes the conversion of cAMP to its noncyclic monophos-phateform, terminating its activity.
Phosphodiesterase 4 (PDE4) is the predominant isozyme in most immune and proinflammatory cells 56 (Table 3). It has an absolute specificity for cAMP. Inhibition of PDE4 activity increases intracellular concentrations of cAMP, down-regulating inflammatory cell activity. 53 The PDE4 isozyme is also found in a variety of structural cells in the lung including bronchial epithelial, endothelial, smooth muscle, and nerve cells. 57
Cilomilast, was the first PDE4i to undergo extensive clinical testing. 58 Phase 3 clinical trials were underway when the decision was made to suspend its development because of an unfavourable side effect profile. 59 Within the PDE4 isozyme family, there are differences between the forms seen in the central nervous system (CNS) (PDE4D) and in immune and proinflammatory cells (PDE4B). 59 Cilomilast preferentially affects PDE4D causing an intolerable amount of nausea and vomiting. 59
Roflumilast has proportionately less effect on PDE4D than cilomilast and recently was the first PDE4i approved for the treatment of COPD. 60 It is a nonselective PDE4i and is less likely to cause nausea and emesis than cilomilast. 61 It is also a more potent anti-inflammatory than cilomilast.61,62 Roflumilast reduces moderate and severe AECOPD in patients with COPD; particularly in those with more severe airway obstruction (FEV1 < 50% of predicted), the clinical phenotype of chronic bronchitis, and a history of AECOPD. 63
Pharmacology of Roflumilast
The pharmacokinetics of roflumilast have been studied in different populations including children, healthy adults, and both asthma and COPD patients. 53 Roflumilast has 80% oral bioavailability and its absorption is not affected by cigarette smoking or food ingestion. 53 Absorption is not affected by either magnesium hydroxy- or aluminium hydroxy-based antacids. Its main metabolite is roflumilast N-oxide which also potently inhibits the PDE4B isozyme. The times to peak concentration are 1.5 and 10 hours and elimination half lives are 10 and 20 hours, for roflumilast and the N-oxide metabolite, respectively. 64 The N-oxide metabolite accounts for approximately 90% of the PDE4B activity and provides reasonable PDE4i over 24 hours allowing for once daily oral administration. 64
There are few clinically important drug interactions apart from potential concerns about the co-administration of roflumilast and rifampin. 65 Fluvoxamine reduces clearance of roflumilast. 53 Specifically, there are no interactions with warfarin, erythromycin, ketoconazole, or midazolam. There are no significant interactions with a variety of respiratory medications including salbutamol, formoterol or budesonide. 53
Preclinical Data
Effects of roflumilast, a phosphodiesterase 4 inhibitor, on various cell types.

Roflumilast Studies in COPD Patients
Grootendorst and colleagues investigated the effects of roflumilast on induced sputum indices in patients with COPD. 70 In a controlled, cross-over, placebo-controlled study of four weeks duration, roflumilast-improved both pre-and post-bronchodilator FEV1. The total number of inflammatory cells, and the numbers of neutrophils, lymphocytes, and eosinophils were reduced in the sputum during roflumilast treatment. 70 Roflumilast also reduced levels of inflammatory cell markers including neutrophil elastase, IL-8, eosinophil cationic protein, and α-2 macroglobulin, a marker of increased microvascular permeability. 70
A total of 516 COPD patients were randomized in a parallel-design, three-armed study comparing 26 weeks treatment with Roflumilast 250 mcg daily and Roflumilast 500 mcg daily to placebo. 71 Both doses of roflumilast improved FEV1 compared to the placebo arm. Morning peak flows and AECOPD rates were also improved with roflumilast. 71
In a second three arm study, patients were either treated for 24 weeks with roflumilast 500 mcg daily, roflumilast 500 mcg daily for 12 weeks followed by placebo for 12 weeks, or placebo for 24 weeks. 72 In patients treated with roflumilast for 24 weeks, FEV1 increased after one week and remained above baseline for the duration of the study. In the patients treated for 12 weeks, FEV1 improved during the roflumilast treatment period and then declined over the subsequent 12 weeks but remained better than pulmonary function in the placebo arm. 72
Phase III Studies in COPD Patients
M2-107 or the RECORD study
Reports of the large roflumilast trials.

Demographics of the large roflumilast trials.
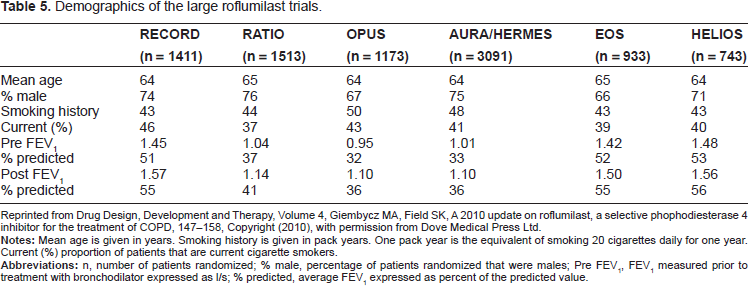
Reprinted from Drug Design, Development and Therapy, Volume 4, Giembycz MA, Field SK, A 2010 update on roflumilast, a selective phophodiesterase 4 inhibitor for the treatment of COPD, 147-158, Copyright (2010), with permission from Dove Medical Press Ltd.
M2-112 or the RATIO study
A subsequent study included patients with more severe COPD. 73 The mean postbronchodilator FEV1 was 41% of predicted in the subjects who were randomized to treatment with daily oral roflumilast 500 mcg for 12 months or to placebo. Treatment with constant doses of IHCS, to a maximum of 2000 μg of beclomethasone daily or its equivalent, and treatment with short-acting anticholinergics at constant doses were allowed but neither LABA nor LAAC were permitted. The co-primary objectives of the study were postbronchodilator FEV1 and the rate of moderate and severe AECOPD. Postbronchodilator FEV1 improved in the roflumilast-treated patients but the AECOPD rate did not. There were no differences in SGRQ between the two treatment groups. Patients treated with roflumilast were more likely to discontinue treatment and were more likely to experience nausea or diarrhea. 73
M2-111 or the OPUS study
An identical study, called OPUS, was undertaken in another population but the results have not been published separately. 74 However, a pooled analysis of these two identical studies, containing 2686 patients with a mean postbronchodilator FEV1 of 39% predicted, demonstrated a 13% reduction in the rate of AECOPD. Post hoc subgroup analyses demonstrated a more pronounced treatment effect in patients with the chronic bronchitis phenotype. 74
M2-124 or the AURA study, M2-125 or the HERMES study
Based on the pooled analyses of the data from the two previous studies, two identical placebo-controlled roflumilast studies were carried out in COPD patients with more severe disease, mean FEV1 less than 50% predicted, the clinical phenotype of chronic bronchitis, and a history of AECOPD. 63 Patients were randomized to treatment with oral roflumilast 500 mcg daily for 12 months or to placebo. The results of the two studies were pooled for analysis. Patients were allowed treatment with LABA but neither IHCS nor LAAC were permissible. Patients were stratified according to their smoking history and whether they were LABA users. The co-primary study endpoints were prebronchodilator FEV1 and the rate of moderate and severe AECOPD. A total of 3096 patients with a mean postbronchodilator FEV1 of 36% of predicted were randomized. Both pre- and postbronchodilator FEV1 improved in the roflumilast arm, 48 ml/s and 55 ml/s, respectively. The combined moderate and severe AECOPD rate was 17% less in the roflumilast-treated group. 63
M2-127 or the EOS trial
Two studies of the effects of adding roflumilast to long-acting bronchodilators were reported in a separate publication. 75 Patients in these studies had less severe airway obstruction than in the M2-124 or M2-125 studies. The mean postbronchodilator FEV1 was 55% and 56% of predicted in the EOS and HELIOS studies, respectively. 75 Chronic bronchitis was not a prerequisite for inclusion in the EOS study, but 79% of the patients recruited had chronic cough and sputum production. In the EOS study, patients taking salmeterol were randomized to receive oralroflumilast 500 mcg daily for 24 weeks or placebo. Both pre- and post-bronchodilator FEV1 were greater in the roflumilast treated group, 49 ml/s and 60 ml/s, respectively. There was a trend to a lower rate of AECOPD among the roflumilast treated patients but the difference was not statistically significant. The median time to the first AECOPD and the proportion of patients with an AECOPD were less in the roflumilast treated patients. 75
M2-128 or the HELIOS trial
In the HELIOS Study, patients treated with tiotropium were randomized to treatment with oral roflumilast 500 mcg daily for 24 weeks or to placebo. 75 Chronic bronchitis was a prerequisite for this study. The mean FEV1 in the study patients was 56% of the predicted value. In the roflumilast arm, pre- and post-bronchodilator FEV1 improved 80 ml/s and 81 ml/s, respectively. There was trend to a lower AECOPD rate in the roflumilast arm but the difference was not statistically significant. The median time to the first AECOPD was greater and the proportion of subjects with an AECOPD was less in the roflumilast treated subjects. The EOS and HELIOS studies revealed that roflumilast improved pulmonary function in patients treated with long-acting bronchodilators. 75
The effects of PDE4i in COPD were the subject of a recent Cochrane Database review. 76 Nine controlled randomized trials with roflumilast, containing data from 9211 patients, were included in the review. It concluded that roflumilast improved pulmonary function in patients with COPD of varying severity and regardless of concurrent therapy. Small but statistically significant improvements in quality of life scores were reported in roflumilast patients but were not considered clinically important. Exercise tolerance was not improved. Most importantly, roflumilast reduced AECOPD frequency (OR 0.78; 95% CI 0.72-0.85). Weight loss occurred in roflumilast treated patients and they experienced more non-serious adverse events, particularly gastrointestinal symptoms and headaches. 76
Addition of Roflumilast to IHCS
That patients treated with long-acting bronchodilators benefited from the addition of roflumilast is not surprising since the addition of anti-inflammatory IHCS to long-acting bronchodilator treatment improves outcomes in patients with more severe COPD.29–31,33 Roflumilast is also anti-inflammatory but has a different anti-inflammatory profile than IHCS. IHCS have a greater effect on eosinophils and CD4+ T lymphocytes whereas, in addition to its effects on these inflammatory cells, roflumilast is also effective against CD8+ T lymphocytes, neutrophils, and CD68+ macrophages.57,59,70 Obvious questions are whether roflumilast is beneficial in patients previously treated with IHCS and whether the addition of roflumilast to IHCS therapy, the combination of two anti-inflammatory medications, offers any benefits to COPD patients? In the AURA and Hermes studies, AECOPD were reduced both in patients with and without a history of IHCS treatment. 63
To investigate the effects of adding roflumilast to IHCS, a post hoc analysis of two identical studies, RATIO and OPUS, that allowed the concomitant use of IHCS, up to the equivalent of 2000 mcg of beclomethasone/day, was undertaken. Approximately 44% of the patients were being treated with IHCS and approximately 20% were receiving combination IHCS and LABA therapy.63,74 If one includes the results of all patients in the two studies regardless of their IHCS use, roflumilast reduced moderate and severe AECOPD by 14.3% (
The authors hypothesized that concomitant IHCS treatment selected for COPD patients with more severe disease who were more likely to suffer AECOPD. 77 The proportion of GOLD stage IV patients was greater in the IHCS treated cohort (28% versus 21%). Consistent with this hypothesis, the IHCS-treated patients randomized to placebo had a higher AECOPD rate than non IHCS-treated patients randomized to placebo (0.89 versus 0.46) making the treatment effects easier to demonstrate. 77
An Unexpected Benefit in Patients with Comorbid Diabetes Mellitus
An unexpected finding in patients with COPD and comorbid diabetes mellitus (DM) type 2 was that roflumilast reduced fasting blood glucose and hemoglobin A1c (HbA1c) levels. 78 Presumably, this effect is mediated by the action of roflumilast on cAMP levels since the small changes in weight would not be expected to have an effect of this magnitude. Fasting blood glucose levels did not change in COPD patients without comorbid DM. These findings suggest that roflumilast may improve glycemic control in patients with co-morbid DM. 78 In a separate study, roflumilast improved fructosamine levels, a marker of short-term DM control, and HbA1c in patients with treatment naive DM type 2 but who did not have COPD. 79 Further studies will be required to determine how roflumilast affects DM control, whether DM outcomes improve, and whether it can prevent some of the complications of DM.
Safety Data
Roflumilast treated patients were more likely to discontinue therapy.27,63,73,75 Serious adverse events were similar in roflumilast- and placebo-treated patients in a pooled analysis of 12,054 subjects in 14 roflumilast treatment trials. 80 Diarrhea (10.1% vs. 2.6%), nausea (5.2% vs. 1.4%), and headaches (4.6% vs. 2.0%) were more common than in placebo-treated patients. 80 Vomiting occurred much less frequently. 63 These symptoms generally occurred early in the treatment period. 27 Roflumilast patients lost an average of 2.2 kg compared to the placebo-treated patients. Weight loss was primarily due to loss of fat mass and was greater in obese and less in underweight patients. 80 The weight loss was partially reversible within 12 weeks of treatment cessation. 81 Cardiovascular adverse events (5.7% vs. 5.9%) and serious cardiovascular adverse events (1.8% vs. 2.1%) were slightly less common in the roflumilast treated patients than in the placebo groups. 80 Mortality and serious adverse events were not increased in roflumilast treated patients. Pneumonia rates were not increased in roflumilast treated patients compared to placebo treated patients. Neuropsychiatric adverse events and rates of the development of some solid tumours were infrequent but occurred more commonly in roflumilast treated patients. 81
Summary
Impact of various treatment interventions on AECOPD frequency.
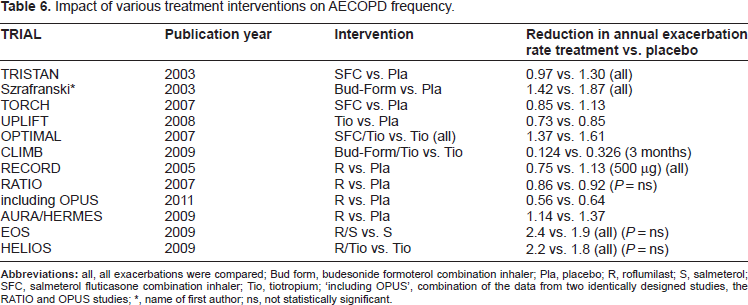
The benefits of roflumilast were greatest in patients with more severe COPD, GOLD stage III and IV disease, and with the chronic bronchitis clinical phenotype, and a history of AECOPD. Its effects on symptoms and consequently on quality of life are relatively small since it is an anti-inflammatory. 82 Although roflumilast is not a bronchodilator, it improved pulmonary function when combined with both short- and long-acting bronchodilators.63,75 The magnitude of the FEV1 increase was similar to that reported in other large COPD treatment trials with bronchodilators and with combination IHCS-LABA inhalers.29–33,41 The most common adverse effects were gastrointestinal symptoms and headaches. Weight loss averaged 2.2 kg more than in the placebo group but was primarily due to fat loss. Roflumilast improved pulmonary function and reduced AECOPD but not respiratory symptoms or quality of life. 76 Since roflumilast is not a bronchodilator, the lack of symptom improvement is not unexpected. 82 Roflumilast was effective whether given alone or in combination with long acting bronchodilators.29,30,31,33 Patients treated with IHCS also appear to benefit from roflumilast therapy. In the roflumilast clinical trials, there were more dropouts in the roflumilast arms than in patients treated with placebo. Convincing patients to continue treatment with roflumilast may be a challenge. 76 The lack of a beneficial effect on respiratory symptoms and the adverse effect profile may interfere with compliance.
Clinical Positioning
The majority of patients in the roflumilast clinical studies had severe (GOLD stage III) or very severe (GOLD stage IV) COPD. The benefits of the medication were less obvious in the earlier studies which included patients with milder disease. Although roflumilast improved pulmonary function and reduced AECOPD, it only mildly improved symptoms and quality of life scores. Patients with milder disease generally do not experience frequent AECOPD. Consequently, any benefit was not as impressive as in the studies with patients with more severe disease. There is not enough evidence to recommend its use in patients with mild disease so it will not have an indication as a first-line treatment. The data for its use was most compelling in patients with the chronic bronchitis phenotype and a history of frequent AECOPD. 83 Patients with chronic bronchitis have more severe airway inflammation that increases further with exacerbations which may explain why these features were predictive of a beneficial response to an anti-inflammatory medication. Exacerbations were decreased and lung function improved when patients with that clinical profile were treated with roflumilast. It was effective when added to short-acting bronchodilators, long-acting beta agonists, or to tiotropium.63,75 A post hoc analysis of two earlier studies demonstrated that it was also effective when added to IHCS. 74 Although contraindicated as monotherapy in COPD, IHCS appear to be beneficial when combined with LABAs in patients with more severe disease. 29 31 There are no head-to-head studies comparing the effectiveness of roflumilast versus IHCS as add-on therapy to long-acting bronchodilators but the addition of roflumilast to LABA resulted in similar reductions in the exacerbation rate as the addition of IHCS.29–31,75 Another option would be the addition of roflumilast to combined LABA and LAAC therapy. The addition of IHCS to the combination of LABA and LAAC did not reduce the overall AECOPD rate but did reduce the rate of severe AECOPD requiring hospitalization. 41 The increase in pulmonary function reported with the addition of IHCS to LABA was similar to the increases demonstrated by adding roflumilast to either class of long-acting bronchodilator. 75 A clinical trial comparing the addition of IHCS versus the addition of roflumilast to combined LAAC and LABA therapy could determine which strategy is superior.
Based on expert opinion, the addition of theophylline is recommended if patients remain symptomatic despite treatment with a combination of inhaled long-acting bronchodilators and IHCS. 4 Theophylline has both bronchodilator and anti-inflammatory properties.50,51 Although there are no comparative studies, this would also seem like a reasonable place to position roflumilast in the treatment algorithm. A clinical trial comparing the addition of theophylline or roflumilast to the combination of LAAC, LABA, and IHCS could resolve which strategy is more effective.
An obvious question with any new medication is whether it will be popular with clinicians and patients and whether it will be successful in the marketplace. 76 Initially, its use will be limited to patients with more severe disease since benefits were minimal in patients with milder disease and unlike the large trials that investigated the effects of long-acting bronchodilators and combination IHCS-LABA inhalers, more trial patients dropped out of the roflumilast treatment arms than the placebo arms. These medications improved respiratory symptoms and had greater effects on quality of life scores than reported with roflumilast. 29 33 It appears that treatment with roflumilast will reduce the cost of care for patients with more severe COPD which should convince governments and 3rd party payers to cover the costs of this novel medication. 84 Roflumilast reduced AECOPD and improved pulmonary function in patients with more severe disease but it had a minimal effect on symptoms and quality of life and gastrointestinal and headache adverse events were more common in the treatment arms. 76 It will be important to see whether patients will be willing to remain on chronic therapy with a medication that does not necessarily make them feel better. 76 This will likely determine its success in the clinical setting.
Abbreviations
acute exacerbation of COPD;
95% confidence interval;
chronic obstructive pulmonary disease
chemokine CXC ligand
diabetes mellitus
‘Evaluation of COPD Longitudinally to Identify Predictive Surrogate End-points’ study
Global initiative for chronic Obstructive Lung Disease
hemoglobin A1c
inhaled corticosteroid
interleukin
long acting anti-cholinergic
long-acting beta agonist
odds ratio
phosphodiesterase 4
phosphodiesterase 4 inhibitor
St. George respiratory questionnaire
TOwards a Revolution in COPD Health trial
tumour necrosis factor-α.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.