
Abstract
Systemic sclerosis (SSc) is a connective tissue disease that is characterized by tissue fibrosis, microvasculopathy, and autoimmunity. Interstitial lung disease (ILD) is a common complication of SSc and is one of the frequent causes of mortality in SSc. Although the exact etiology of SSc remains unknown, clinical and experimental investigations have suggested that genetic and environmental factors are relevant to the pathogenesis of SSc and SSc-ILD. More than 30 genes have been identified as susceptibility loci for SSc, most of which are involved in immune regulation and inflammation. It is thought that the key pathogenesis of SSc-ILD is caused by the release of profibrotic mediators such as transforming growth factor β1 and connective tissue growth factor from lung cells induced by a persistent damage. This review presents the genetic susceptibility to SSc-ILD, including human leukocyte antigen and non-human leukocyte antigen genes, especially focusing on connective tissue growth factor.
Introduction
Systemic sclerosis (SSc) is a chronic multisystem autoimmune disease that is characterized by autoimmunity, tissue fibrosis, and vasculopathy. Clinical and experimental investigations have suggested that genetic factors and environmental factors are relevant to the pathogenesis of SSc. 1 Recently, various genetic studies have shown that candidate genes and single nucleotide polymorphisms (SNPs) may be risk factors for the development of SSc. 2
Interstitial lung disease (ILD) is a life-threatening complication and is one of the frequent causes of mortality in SSc, along with pulmonary arterial hypertension. The key pathogenesis of SSc-ILD is thought to be initiated by a persistent injury to lung cells that induces profibrotic stimuli, which leads to fibroblast activation and myofibroblast transition. Lung injury results in the release of profibrotic mediators such as transforming growth factor β1 (TGF-β1) and connective tissue growth factor (CTGF); CTGF causes the additional recruitment of myofibroblasts and the overproduction and accumulation of extracellular matrix.3–5
Several studies show that an SNP in the CTGF gene plays a crucial role in SSc and SSc-ILD.6,7 CTGF is increased in the circulation, skin, and fibroblasts of patients with SSc. CTGF regulates the proliferation of fibroblasts and the production of extracellular matrix.8 10 Our aim in this review is to present the genetic susceptibility to SSc-ILD.
Genetics and SSc
The incidence of SSc is 1.5%-1.7% in people with a family history of SSc, while it is 0.026% in the general population. SSc is not inherited in a Mendelian fashion; however, having family members who have SSc or another autoimmune disease increases the relative risk. Having a sibling with SSc results in a 15- to 19-fold increased risk, and first-degree relatives have a 13- to 15-fold increased risk of having SSc compared with the general population. 11
Observation studies among Caucasian and African-American patients have suggested that African-Americans have a genetic tendency to develop SSc and also have a higher morbidity and mortality.12,13 Early genetic studies indicated that SSc was associated with the human leukocyte antigen (HLA) region. 14 Moreover, many candidate gene studies have identified multiple novel polymorphisms that increase susceptibility to SSc. Explorative genetic association studies later discovered significant associations between SSc and SNPs within the immune regulatory genes, including STAT4,15–17 TNFSF4,18,19 TBX21, 17 NLR family pyrin domain containing 1 (NLRP1), 20 BLK,21–23 BANK1,24,25 CD247,26,27 PTPN22,28–30 IL23R,31,32 CD226, 33 PLD4, 34 and TLR2, 35 and the inflammatory genes, including IL1A, 36 interleukin-1 receptor-associated kinase 1 (IRAK1),37,38 interferon regulatory factor 5 (IRF5),39–41 TNFAIP3,42,43 CTGF,6,7 CXCL8, 44 and CCR6. 45
Genome-wide association studies (GWASs) can be used for a comprehensive identification of novel loci. In 2010, a large GWAS reconfirmed the associations of SSc with HLA, IRF5, and STAT4 and identified CD247, IRF8, GRB10, and SOX5.26,46 Other GWASs in a French cohort recognized three new loci, namely, TNIP1, PSORS1C1, and RHOB, that were associated with SSc. 47
Genetic Association in SSc-ILD
HLA-Dependent Genes
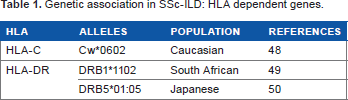
Associations among HLA alleles, susceptibility to SSc and specific autoantibodies, and clinical features of SSc have been identified. A study in Canada among Caucasian patients with SSc revealed that HLA-Cw*0602 is associated with patients with pulmonary fibrosis. 48 In South Africans, DRB1*11 is associated with pulmonary fibrosis. 49 Another study conducted in Japan suggested that the HLA-DRB5*01:05 allele was a risk factor for ILD patients with SSc (Table 1). 50
Genetic association in SSc-ILD: HLA dependent genes.
Non-HLA genes
As mentioned earlier, numerous genes have been identified as susceptibility loci for SSc. Some of them revealed an association with SSc-ILD. CTGF was significantly associated with the presence of ILD, and the details are presented below. The CD226 gene encodes DNAX accessory molecule-1, which is involved in the adhesion and activation of T-cells. The nonsynonymous CD226 rs763361 SNP (Gly307Ser) may affect the expression of the CD226 molecule. In European Caucasians, the rs763361 T allele was associated with a diffuse cutaneous SSc subtype (dcSSc), an antitopoisomerase I antibody, and SSc-ILD subsets. 33 IRF5 is a crucial component of type I IFN regulation. A large case–control study in French Caucasians discovered an association between the IRF5 rs2004640 T allele and SSc. Additional associations between T allele and fibrosing alveolitis were found. 39
NLRP1 performs as an endogenous microbial product and a metabolic stress sensor and consequently activates the innate immune system in conjunction with inflammasomes. These cytoplasmic proteins promote the inflammatory cytokines such as IL-1β, IL-18, and IL-33. IL-1β has been suggested to have an association with SSc fibroblasts. In European Caucasians, the NLRP1 rs8182352 variant was associated with antitopoisomerase I antibody and SSc-ILD. 51
IRAK1, which is located on the X chromosome, regulates T-cell receptor signaling pathways and Toll-like receptor activation. A study in European Caucasians discovered the notable association between the IRAK1 rs1059702 TT genotype and dcSSc, the antitopoisomerase I antibody, and SSc-ILD. 37 Another study in five independent Caucasian cohorts showed that the association of IRAK1 rs1059702 with dcSSc was interpreted by the nearby SNP of MECP2 rs17435, but the association of IRAK1 rs1059702 with pulmonary fibrosis was still present. 38
Matrix metalloproteinase-12 (MMP-12) is one of the proteins of the MMP family. An association between serum MMP-12 levels and severity of skin and pulmonary fibrosis and peripheral vascular damage in SSc patients has been reported. 52 In an Italian cohort, a significant difference was observed in MMP12 rs2276109 genotype distribution between patients with SSc and a control group. In particular, the homozygosity for the A allele was significantly associated with dcSSc, antitopoisomerase I antibody, and ILD. 53
Interleukin-1α (IL-1α) stimulates dermal fibroblasts to synthesize several types of cytokines and growth factors that activate fibroblasts to produce the extracellular matrix. It was shown that SSc fibroblasts constitutively produced high levels of pro-IL-1α. 54 The association among three SNPs at positions -889, +4729, and +4845 of the IL1A gene and SSc in Japanese patients has been reported. The three SNPs were in linkage disequilibrium, and the CTG haplotype frequency was significantly higher in patients with SSc than in healthy control subjects. The frequency of the diplotype CTG/CTG was significantly associated with SSc-ILD patients. 36
Hepatocyte growth factor (HGF) is an antifibrotic factor and acts against the profibrotic actions of TGFβ. However, SSc patients have high levels of HGF in circulation. These findings suggest that increased HGF levels are insufficient to inhibit fibrotic progression. 55 In Japanese patients, the distribution of HGF rs3735520 SNP was not significantly different between patients with SSc and healthy controls. However, the SNP was significantly associated with patients with end-stage lung disease. 56
Pulmonary surfactant protein B (SP-B) acts as a protective substance against lung injury. A study in Japanese patients showed that the frequency of the TT genotype in the SFTPB rs1130866 was not different between SSc patients and healthy controls but was significantly lower in patients with SSc-ILD than in those without ILD. This result suggested that the TT genotype in SP-B was associated with a lower risk of SSc-ILD (Table 2). 57
Genetic association in SSc-ILD: non-HLA genes.

SSc without ILD
SSc with end-stage lung disease (ESLD)
SSc without ESLD.
Gene Polymorphisms of cTGF Associated with SSc-ILD
CTGF was found to have increased expression in the circulation, skin, and fibroblasts of patients with SSc. Moreover, CTGF regulates proliferation of fibroblasts and production of extracellular matrix.8-10,58 Studies in the UK and Japan reported that an SNP in the promoter region of CTGF rs6918698 (-945C/G) was significantly associated with SSc.6,7
In a UK cohort study by Fonseca et al, the GG genotype of CTGF rs6918698 was significantly more common in patients with SSc than in control subjects. The study showed a notable association between the GG genotype and the presence of antitopoisomerase I and anticentromere antibodies. Additionally, a logistic regression analysis was performed among the clinical phenotypes, which revealed a significant association between the G allele and fibrosing alveolitis. The study also showed that the presence of C allele at position-945 is critical for transcriptional suppression of the CTGF gene through Sp3 binding. The result of this suppression would reduce CTGF production. A previous study reported that Sp1 often acts as a stronger activator than Sp3 and that Sp3 also often acts as a repressor in the CTGF promoter. Fonseca et al showed that the ratio of Sp1 to Sp3 binding in lung fibroblasts was approximately three times as high for GG homozygote cells as for CC homozygote, a finding that was in agreement with higher transcriptional activity from the G allele. Moreover, they showed that SSc fibroblasts had a generally higher ratio of Sp1 to Sp3 binding than control cells. This functional explanation would be reasonable for the observation that the G allele is associated with SSc. CTGF is constitutively overexpressed by fibroblasts in fibrotic skin lesions as well as in lung fibroblasts of SSc patients. 59 Furthermore, higher levels of CTGF are seen in bronchoalveolar lavage fluid from active SSc-ILD patients. 58 Such a functional explanation would be in agreement with the observation that the G allele is associated with SSc-ILD. Therefore, increased CTGF expression is comprehensible in the observation of functional analysis. 6
A study in a Japanese cohort by Kawaguchi et al confirmed the association between the frequency of the G allele in CTGF rs6918698 and the susceptibility to SSc. The study also confirmed a significant association between the frequency of the G allele and the presence of dcSSc, ILD, and antitopoisomerase I antibody in SSc. However, the authors did not indicate any association between the SNP and the presence of an anticentromere antibody in SSc. They discovered a significant association between the G allele and the GG genotype and patients with limited cutaneous SSc and ILD. Therefore, these observations suggest that the G allele and the GG genotype of CTGF rs6918698 may be susceptible to SSc-ILD, independent of skin fibrosis. 7
A replication study of the CTGF gene in 1311 North American patients (white Americans, African-Americans, and Hispanic Americans) did not validate susceptibility to any form of SSc. 60 A multicenter study in seven independent case–control sets, including Spanish, Dutch, German, French, British, Swedish, and North American groups, also failed to confirm an association between SNP and SSc. 61 Two other replication studies in France and Thailand also could not confirm this association.62,63 Zhang et al performed a meta-analysis of six published case–control studies including 3335 cases and 3589 controls. The study showed that the CC and CG genotypes of CTGF rs6918698 in Asians were significantly associated with a reduced SSc risk. In contrast, no association was revealed in Caucasians or the overall population. This meta-analysis did not assess any clinical phenotypes or antibodies because some of the studies lacked detailed data. 64
Discrepancies in the genetic association studies of different races have been reported.65–67 One of the possible explanations for this discrepancy between Asians and Caucasians could be a result of different gene–environment interactions among populations. A second explanation might be because of the linkage disequilibrium or correlation with a different SNP. The French study by Granel et al showed that CTGF rs6918698 was not correlated with another SNP (rs9399005). However, in the HapMap reference populations, the two markers were correlated. 62 Thus, these genetic and environmental factors affect the susceptibility to SSc and complicate these replication analyses (Table 3).
Summary of studies on association of the CTGF rs6918698 polymorphism with SSSSc.

The Difference of Susceptible Genes among SSc-ILD and Idiopathic Pulmonary Fibrosis
Genetic factors contribute to the susceptibility of idiopathic pulmonary fibrosis (IPF) also. In familial IPF cases, strong associations have been identified with rare mutations in the surfactant protein A or C genes. Several reports revealed that the genetic variants in the genes within the human telomerase components are associated with familial and sporadic IPF. These mutations result in telomere shortening and a consequent apoptosis of cells, including the alveolar epithelial cells. Recently, two GWASs reported that a common SNP of the MUC5B gene, which encodes airway epithelial mucin glycoprotein, is associated with the risk of IPF. These studies also identified other IPF-associated loci, including the Toll-interacting protein (TOLLIP), which negatively interacts with Toll-like receptor signaling. The MUC5B promoter and TOLLIP variants have been related to survival in IPF.
Interestingly, except HLA, none of the known genetic variants, including the MUC5B gene linked to IPF, have been associated with SSc-ILD.68,69
This discrepancy between SSc-ILD and IPF may be explained by the difference of the prominent pattern of the radiological and pathological patterns. The prominent pattern is nonspecific interstitial pneumonia in SSc-ILD. On the other hand, usual interstitial pneumonia is predominant in IPF. These findings suggest that the pathogenesis of SSc-ILD is different from IPF.
Conclusions
The pathogenesis of SSc is not fully understood. In this article, we reviewed the genetic association with SSc-ILD, especially the SNP in the CTGF gene that is involved in the development of SSc and SSc-ILD. SSc-ILD does not have an effective treatment and results in increased mortality in patients with SSc. Investigation of the pathogenesis, including genetic analysis, may result in the development of a novel therapy.
Author Contributions
Conceived and designed the experiments: AT, YK, HY. Analyzed the data: AT, YK. Wrote the first draft of the manuscript: AT. Contributed to the writing of the manuscript: AT, YK. Agree with manuscript results and conclusions: AT, YK, HY. Jointly developed the structure and arguments for the paper: AT, YK, HY. Made critical revisions and approved final version: AT, YK, HY. All authors reviewed and approved of the final manuscript.