
Abstract
Pulmonary involvement is common in rheumatoid arthritis (RA) and affects all the components of the lung. Interstitial lung disease (ILD) is the most predominant pulmonary manifestation and has been identified as the main cause of morbidity and mortality in RA. Clinically significant RA-ILD occurs in approximately 10% of RA patients. Several risk factors, such as old age, male gender, and smoking, have been reported to date. Histologically, the proportion of the usual interstitial pneumonia (UIP) pattern is higher in RA-ILD than in ILD associated with other connective tissue diseases, and RA-ILD also shows nonspecific interstitial pneumonia and organizing pneumonia patterns. High-resolution computed tomography scans are highly predictive of the histological UIP pattern with a specificity of 96%-100%. Acute exacerbation, which is the acute deterioration of the respiratory status characterized by newly developed bilateral infiltrates with unknown etiologies, has been reported in RA-ILD. Although acute exacerbation of RA-ILD has high mortality, similar to that of idiopathic pulmonary fibrosis, its incidence is lower in RA-ILD than in idiopathic pulmonary fibrosis. A consensus treatment has not yet been established. Current therapeutic regimens typically include corticosteroids with or without cytotoxic agents. Recent large longitudinal studies reported that the prognosis of RA-ILD was poor with a median survival of 2.6-3.0 years. Furthermore, histological and/or radiological patterns, such as UIP or non-UIP, have significant prognostic implications. RA-ILD patients with histological or radiological UIP patterns have poorer prognoses than those with non-UIP patterns. This review assessed the characteristics of RA-ILD by overviewing recent studies in the field and focused on the clinical significance of histological and/or radiological patterns in RA-ILD.
Keywords
Introduction
Rheumatoid arthritis (RA) is a systemic inflammatory disease with a prevalence of approximately 0.5%-1.0% in the general population. 1 Although this disease is primarily characterized by destructive inflammatory arthritis, a large proportion of RA patients present extra-articular manifestations, involving the skin, eyes, heart, and lungs. 2 Pulmonary involvement is common, affecting all the components of the lung, such as the airways, parenchyma, pleura, and pulmonary vasculature. Among these, interstitial lung disease (ILD) is the most predominant manifestation. The prognosis of RA-ILD was recently reported to be poor in several large studies, with a mean survival of only three years from the diagnosis of RA-ILD.3,4 Thus, RA-ILD is associated with high morbidity and mortality. 5
ILD comprises a wide variety of disorders with distinct histological and/or radiological patterns. In 2013, the American Thoracic Society (ATS)/European Respiratory Society (ERS) revised the multidisciplinary classification of idiopathic interstitial pneumonias (IIPs), including six major IIPs: idiopathic pulmonary fibrosis (IPF), idiopathic nonspecific interstitial pneumonia (NSIP), respiratory bronchiolitis–interstitial lung disease, desquamative interstitial pneumonia, cryptogenic organizing pneumonia, and acute interstitial pneumonia. 6 The histological and/or radiological pattern of IPF refers to usual interstitial pneumonia (UIP), while that of idiopathic NSIP refers to NSIP. In IIPs, distinguishing UIP from NSIP has important prognostic implications because the prognosis of IPF is markedly poorer than that of idiopathic NSIP. 6 These histological and/or radiological patterns have also been identified in other ILDs, such as connective tissue disease-associated ILD (CTD-ILD). Unlike IIPs, several studies have reported no prognostic difference between UIP and NSIP in CTD-ILD.7,8 The survival of CTD-ILD patients with the histological UIP pattern was shown to be similar to that of patients with the NSIP pattern.7,8 However, RA-ILD with the histological and/or radiological UIP pattern was more recently shown to have a poorer prognosis than that with the NSIP pattern.9–11 This finding suggests that distinguishing the UIP pattern from other patterns in RA-ILD may provide important clinical information on treatments and prognoses.
This review assessed the characteristics of RA-ILD by overviewing recent studies in this field and focused on the clinical significance of the histological and/or radiological patterns in RA-ILD.
Epidemiology and Clinical Manifestations
The prevalence of RA-ILD widely varies depending on the cohort studied and detection methods.12,13 Recent studies using high-resolution computed tomography (HRCT) reported prevalence at a range of 27%-67%14,15; however, a large proportion of these RA-ILD patients were asymptomatic. Clinically evident ILD occurs in approximately 10% of RA patients. 16 The prevalence of RA-ILD was recently shown to become higher among RA patients. 16 Several risk factors, including old age, male gender, smoking, high titer of rheumatoid factor, and elevated levels of serum anti-citrullinated protein antibody (ACPA), have been reported.3,4,17,18 Recent advances in the pathophysiology of RA have highlighted an important role of smoking.18,19 Tobacco exposure promotes protein citrullination in the lung. Indeed, elevated levels of citrullination are present in bronchoalveolar lavage (BAL) of smokers compared with nonsmokers. 20 Additionally, lung tissues of RA-ILD contain high amounts of citrullinated proteins. 21 It is hypothesized that the citrullinated proteins in the lung become targets for autoimmunity, leading to the generation of ACPA. In this process, the interplay between the ACPA and HLA-DRB1 share epitope increases the risk of RA.22–24 Because serum levels of ACPA have been shown to be highly associated with the risk of RA-ILD, protein citrullination in the lung caused by smoking may play a role in the development of RA-ILD. Possibly, other environmental factors, such as air pollution, may affect the effect of smoking on the development of RA-ILD. 24
Although the most common symptoms associated with RA-ILD are dry cough and dyspnea on exertion, asymptomatic, subclinical patients having only radiological and/or physiological abnormalities are not rare.13,25 Most RA-ILD patients present fine crackles primarily on bibasilar lung fields. ILD may precede the development of arthritis in RA. Lee et al reported three patients with RA-ILD in whom ILD preceded the diagnosis of RA (1.6-7 years). 26 Kono et al demonstrated that 4 of 111 patients with an initial diagnosis of IPF subsequently developed RA 1-4 years after the IPF diagnosis. 27 Patients who develop RA were significantly younger, more likely to be women, and had a better prognosis than those with IPF. Most importantly, these patients showed prominent lymphoid aggregates with germinal centers on initial surgical lung biopsy (SLB).
Pathology
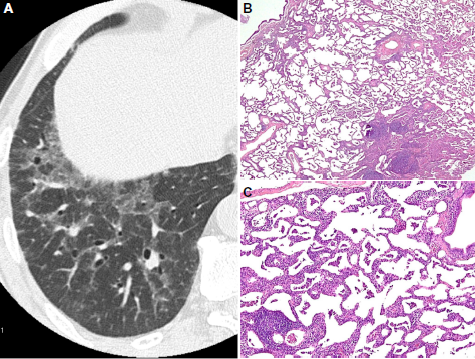
The histological patterns of RA-ILD are generally classified according to the current ATS/ERS international consensus classification of IIPs. 6 However, there are several histological differences between RA-ILD and IIPs. Lymphoid hyperplasia with germinal centers, and pleural and peribronchiolar lesions are more frequently detected in RA-ILD than in IIPs, whereas fibroblastic foci are less common (Figs. 1 and 2).28,29 Furthermore, mixtures of each histological pattern (eg, UIP plus NSIP patterns) are occasionally present, leading to difficulties in making a definite histological diagnosis of RA-ILD.

A case of RA-ILD with the histological UIP pattern. (
A case of RA-ILD with the histological Nsip pattern. (
In CTD-ILD, the most common histological pattern is NSIP.7–9 In contrast, the proportion of the UIP pattern was reported to be higher in RA-ILD. Table 1 summarizes the reported proportions of histological patterns in patients with RA-ILD.4,9,26,30-35 The proportion of UIP patterns in RA-ILD varied from 13% to 74%, with an average of 40%. Recent studies have constantly reported a high proportion of the UIP pattern (36%-54%) in RA-ILD.26,34,35 Cumulative data have indicated that RA-ILD with the UIP pattern has different clinical characteristics from that with non-UIP patterns. Thus, a histological diagnosis provides valuable information for the management of patients with RA-ILD.
Histological patterns of RA-ILD.

Radiology
In practice, SLB is not routinely performed in RA-ILD. Thus, radiological imaging techniques, especially HRCT, are used for subtyping RA-ILD or predicting its histological pattern. In RA-ILD, HRCT patterns are classified primarily as the UIP, NSIP, or organizing pneumonia (OP) pattern based on the recent guidelines of IIPs. 36 Briefly, the UIP pattern on HRCT is featured by subpleural and basal predominance, reticular opacities, and honeycombing with or without traction bronchiectasis (Fig. 1). The NSIP pattern includes bilateral ground-glass opacities, reticular opacities with or without traction bronchiectasis, occasional honeycombing, and often a subpleural sparing distribution (Fig. 2). The OP pattern is characterized by patchy consolidation in a subpleural, peribronchial, or band-like pattern, commonly associated with ground-glass opacities. UIP is the most common HRCT pattern, ranging from 24% to 65%, followed by NSIP (Table 2).9,11,30,37
HRCT patterns of RA-ILD.

Regarding the accuracy of HRCT in identifying the histological UIP pattern in RA-ILD, Assayag et al recently reported that a definite UIP pattern on HRCT (characterized by basal and subpleural interstitial reticulations and fibrosis, traction bronchiectasis, and honeycombing 36 ) was highly predictive of the histological UIP pattern with a specificity of 96% (26 of 27 cases) and a sensitivity of 45% (19 of 42 cases). 38 Hozumi et al also showed that the specificity and sensitivity of HRCT for the histological UIP pattern were 100% and 41.7% in RA-ILD, 37 respectively. Compared with similar studies in IPF, the specificity of HRCT is comparable, while its sensitivity is lower.39,40 Taken together, these findings provide evidence to support HRCT as a useful noninvasive tool for predicting the histological UIP pattern in RA-ILD patients, especially in those with the definite UIP pattern on HRCT.
Diagnosis
In a clinical setting, routine screening for ILD is recommended for all RA patients. The symptoms and signs suggestive of ILD, such as dry cough, dyspnea on exertion, and fine crackles on auscultation need to be routinely evaluated. In addition, a chest radiograph needs to be taken at the diagnosis of RA. When ILD is suspected, a further evaluation includes an assessment of pulmonary function tests and imaging with HRCT. HRCT is capable of detecting the early stages of ILD in patients without respiratory symptoms. Although the histological diagnosis of ILD, such as UIP or NSIP, has important prognostic implications, SLB is not recommended for all patients with RA-ILD. HRCT findings accurately identify histological patterns, especially the UIP pattern, with a high specificity. Transbronchial lung biopsy and BAL are not diagnostic, but are used to rule out other conditions, such as infection. Regarding BAL findings, higher proportions of neutrophils and/or lymphocytes with an increase in total cell counts have been reported in RA-ILD.41,42 Serum levels of Krebs von den Lungen-6 and surfactant protein-D, both of which are biomarkers for ILD, are often elevated in RA-ILD,43,44 although these biomarkers are currently used only as research tools in most of the countries other than Japan. Levels of matrix metalloproteinase-9 (MMP-9), MMP-7, pulmonary and activation-regulated chemokine/CCL18, and interferon-γ-inducible protein 10 (IP-10)/CXCL10 were also reported to be useful biomarkers for RA-ILD detection.45,46 Due to the wide utilization of HRCT imaging in clinical practice, the number of patients with subclinical RA-ILD, who have abnormalities suggestive of having ILD on HRCT in the absence of respiratory symptoms, has recently increased. Some of these patients will develop overt ILD over time 13 ; however, the clinical significance of subclinical RA-ILD has not yet been determined.
In any RA patient with diffuse lung disease, drug-induced lung injury and infection need to be carefully distinguished from RA-ILD. A number of medications for RA, including disease-modifying anti-rheumatic drugs and anti-Tumor necrosis factor (TNF) agents, have pulmonary toxicities.47–49 Thus, the differential diagnosis of drug-induced lung injury is often challenging. Although several diagnostic criteria for drug-induced lung injury have been proposed,50,51 it is essential to take a detailed medical history, including the use of the suspected drug, and temporal relationships between the onset and the drug usage. In addition, risk factors for drug-induced lung injury should be taken into account when giving medications for RA. For example, the identified risk factors for methotrexate-induced lung injury include male gender, smoking history, and existing ILD.52,53 Since medications used in the treatment of RA often cause an immunosuppressive status, pulmonary infections, such as pneumocystis pneumonia, need to be included in the differential diagnosis.
Acute Exacerbation
Acute exacerbation (AE) was established as a distinct condition with the acute deterioration of the respiratory status in IPF.36,54 AE is characterized by newly developed bilateral ground-glass opacities and/or consolidations on chest radiographs or CT scans, without other alternative causes such as infection, heart failure, pulmonary embolism, or other identifiable causes. AE has more recently been detected not only in patients with IPF but also in patients with other ILDs, including idiopathic NSIP, CTD-ILD, and chronic hypersensitivity pneumonitis.55,56 Among CTD-ILD, AE is the most common in RA-ILD with a poor prognosis (Fig. 3).55,57 Hozumi et al reported that AE occurred in 11 of 51 RA-ILD patients with a one-year cumulative incidence of 2.8%. 37 Although the cumulative incidence of AE in RA-ILD is lower than that in IPF (one-year cumulative incidence, 5%-20%),58,59 this is an extremely poor condition with a high mortality (64%), similar to AE in IPF. Furthermore, old age at the diagnosis of ILD, UIP pattern on HRCT, and methotrexate usage have been correlated with the development of AE in RA-ILD. Collectively, although the AE incidence in RA-ILD is not as high as that in IPF, this serious condition needs to be more carefully considered in RA-ILD.

High-resolution CT (HRCT) of acute exacerbation (AE) in an RA-ILD patient. (
Treatment
A consensus treatment for RA-ILD has not yet been established because there have been no randomized clinical trials in RA-ILD. Due to the absence of evidence for therapy and its potential adverse effects, the decision to treat needs to be made based on the balance between its benefits and burden of the disease in each patient. Disease progression and its severity are the two main factors that are considered when deciding to treat. Treatment is typically initiated in RA-ILD patients who show a progressive course with respiratory symptoms, while asymptomatic patients are generally just monitored. It is considered important to carefully follow-up RA-ILD patients at optimal intervals with imaging (chest radiographs and/or HRCT) and pulmonary function tests.
Current therapeutic regimens generally include corticosteroids (oral prednisolone 0.5-1.0 mg/kg/day) with or without cytotoxic agents, such as cyclophosphamide, azathioprine, cyclosporine, and mycophenolate mofetil (MMF). If a response is achieved, the dose of prednisolone is gradually tapered to 5-10 mg/day in 6-12 months. Pulsed intravenous methylprednisolone (1.0 g/day for 3 days) is occasionally administered for aggressive RA-ILD with severe respiratory failure or the AE of RA-ILD. Recent studies demonstrated the effectiveness of MMF in CTD-ILD.60–62 Of 125 CTD-ILD patients treated with MMF, the percentages of forced vital capacity (%FVC) improved slightly in 18 RA-ILD patients after the administration of MMF. 62 MMF has also been shown to be safe and well tolerated in CTD-ILD.60–62 Cyclosporine has been used in the treatment of RA-ILD.63,64 However, Tokano et al reported no persisting response to cyclosporine in four patients with steroid-resistant RA-ILD. 65 Thus, the effectiveness of cyclosporine in RA-ILD remains undefined and needs to be examined in more detail. Rituximab is a monoclonal antibody against the B-cell marker CD20, and evidence for its effectiveness in RA is increasing.66,67 Keir et al reported that rituximab offered an effective therapeutic option in 33 patients with severe CTD-ILD unresponsive to conventional therapy, including two patients with RA-ILD. 68 Hartung et al also successfully treated a case of refractory RA-ILD with rituximab. 69 These findings warrant future, prospective studies to validate the effectiveness and safety of rituximab in RA-ILD.
Several studies raised the possibility that the response to therapy correlated with the histological patterns in RA-ILD.9,10,26 RA-ILD with the NSIP pattern had more favorable responses to therapy than that with the UIP pattern, resulting in a better prognosis.9,10,26 Moreover, patients with the OP pattern typically showed rapid improvements in response to corticosteroid therapy with a complete recovery.70,71
In addition to the above medications, the cessation of smoking is regarded as essential in smokers with RA-ILD. Vaccinations for pneumococcus and influenza are also recommended, especially in RA-ILD patients receiving immunosuppressive therapy. Supplementary oxygen was shown to be beneficial for patients with hypoxemia. Lung transplantation is considered a therapeutic option for patients with severe respiratory failure.
Prognosis
Two large longitudinal cohort studies of RA-ILD, Early Rheumatoid Arthritis Study in England and the Rochester Epidemiology Project in the United States, recently demonstrated that the prognosis of RA-ILD was poorer than originally expected.3,4 These two studies provided similar information; median survival after the diagnosis of ILD was only 2.6-3.0 years with a five-year survival rate of 35%-39%, which was similar to IPF. Several poor prognostic factors of RA-ILD, such as old age at diagnosis, male gender, lower diffusing capacity of the lung for carbon monoxide, and a definite UIP pattern on HRCT, have also been reported.3,37,59 A recent systematic review by Assayag et al identified significant predictors of mortality using a multivariate analysis, including old age, male gender, lower diffusing capacity of the lung for carbon monoxide, extent of fibrosis, and the presence of the UIP pattern on biopsy or HRCT. 72
Recent advances have clearly highlighted the prognostic implications of the histological and/or radiological pattern of RA-ILD. Histologically, the prognosis of RA-ILD patients with the UIP pattern was shown to be poorer than that of patients with non-UIP patterns.8,34,73 On HRCT, a definite UIP pattern may predict a significantly worse survival. 9 Table 3 summarizes the reported prognoses of RA-ILD patients with the UIP pattern. Therefore, in a clinical setting, distinguishing UIP from non-UIP by either biopsy or HRCT is important for appropriately managing patients with RA-ILD. Furthermore, because HRCT is highly predictive of the histological UIP pattern with a high specificity, this imaging technique may be a more pragmatic, noninvasive approach for assessing the prognosis of RA-ILD patients. However, there is a conflicting report to show that overall prognosis of RA-ILD with a UIP pattern was significantly better compared with IPF. 74 The above studies that reported the prognostic significance of the UIP pattern included relatively small number of RA-ILD patients with a retrospective design. Further prospective studies in larger series of RA-ILD patients are required to confirm the prognostic role of the UIP pattern.
Prognosis of RA-ILD with the UIP pattern.

Conclusion
Although current improvements in therapies for RA (eg, biologic agents) have enabled us to control its disease activity, resulting in a decline in death from RA, the burden and mortality of RA-ILD are increasing. 16 Thus, RA-ILD has become a more critical cause of morbidity and mortality in RA. In this context, recent advances in RA-ILD have provided important information, as follows. The prognosis of RA-ILD is generally poor, similar to that of IPF. Histological and/or radiological patterns, such as UIP or non-UIP, have clinical implications for the prognosis of RA-ILD. HRCT may play an important role in the discrimination of UIP from non-UIP in clinical practice. Similar to IPF, AE also occurs in RA-ILD with a poor prognosis; however, its incidence is lower in RA-ILD than in IPF. Despite these recent advances, no consensus optimal therapy has been established to date because randomized controlled trials have not yet been conducted. Optimal treatments may differ with histological and/or radiological patterns in RA-ILD. Large controlled studies specifically designed to assess the effectiveness of treatments in each subtype of RA-ILD are urgently needed.
Author Contributions
Conceived the concepts: TS. Analyzed the data: TS. Wrote the first draft of the manuscript: TS. Developed the structure and arguments for the paper: TS. Made critical revisions: TS. The author reviewed and approved of the final manuscript.