
Abstract
It is encouraging to observe that a search for publications on “asymmetric dimethylarginine (ADMA)” in PubMed, as updated on June 2016, yielded >2500 items, 24 years after a splendid paper published by Vallance et al in which the authors proposed that ADMA accumulation could be a cardiovascular risk factor in chronic kidney diseases. ADMA is the endogenous inhibitor of nitric oxide synthase and is related to endothelial dysfunction, which plays an important role in vascular damage elicited by various cardiometabolic risk factors. Although current knowledge suggests that ADMA has critical central roles in renal diseases, there are still unexplained details. The present article aims to provide a review on ADMA and its relation as a biomarker in nephrologic diseases. We aimed to systematize articles in which ADMA levels were assessed in order to clarify its role in many diseases and establish its reference values in different populations.
Keywords
Introduction
In 1970, long before the discovery of nitric oxide (NO), Kakimoto and Akazawa were the first pioneers to isolate and describe N-N, N-G- and N-G, N‘-G dimethylarginine from human urine. Today, these substances are known as asymmetric dimethylarginine (ADMA; NG,NG-dimethyl-l-arginine) and symmetric dimethylarginine (SDMA; a structural isomer of ADMA). 1 Vallance et al first demonstrated that methylated arginines, capable of inhibiting NO synthesis, circulate in plasma and also showed that patients with end-stage renal disease (ESRD) on hemodialysis had higher ADMA levels than controls. The study was a milestone and game changer. After these findings, the possibility of these compounds acting as endogenous regulators of l-arginine to NO pathway in health and diseases raised considerably.2,3
ADMA is a naturally occurring post-translationally modified form of arginine that is generated in all cells during physiological protein turnover. This molecule has a low molecular weight (202 Da), and it is a relatively stable substance. It can also diffuse between cells (easy entry-exit), is excreted in urine, and can be found in tissues and cells.2,4 Intracellular entry of arginine can be supplied through the Y+ transporter – cationic amino acid transporter. 4
ADMA, but not SDMA, has a crucial role as an endogenous inhibitor of nitric oxide synthase (NOS; EC 1.14.13.39) by competing with l-arginine as a substrate (Fig. 1). NO has key roles in the pathophysiology of endothelial dysfunction, in the progression of atherosclerosis, and in cardiovascular diseases. 5 NO, also known as endothelium-derived relaxing factor or EDRF, is a simple gaseous molecule with countless remarkable physiological functions. NO is also an important messenger in many vertebrate signal-transduction processes. It is produced endogenously from arginine in a complex reaction that is catalyzed by NOS. NADPH and O2 are required for the synthesis of NO (Fig. 1). 6 l-arginine/NO biosynthetic pathway is involved in many physiological and pathophysiological processes. They include neurotransmission, vascular tone (by stimulating NO-sensitive guanylyl cyclase), regulation of gene transcription, mRNA translation, and production of post-translational modifications of proteins. 7
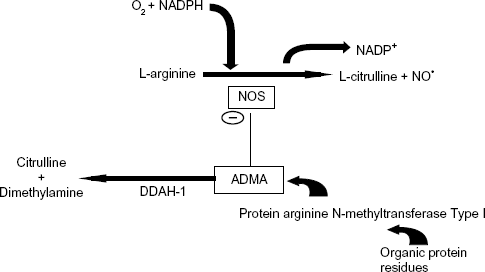
Arginine is a basic amino acid whose ionized group is a guanidinium. The side chains of this amino acid are fully protonated at pH 7. On the other hand, ADMA is created by protein methylation, a type of post-translational modification. This reaction is catalyzed by an enzyme set called protein arginine N-methyltransferase (PRMT; Fig. 1). These enzymes can transfer a methyl group from S-adenosyl methionine to the guanidino nitrogen of arginine.8,9 Although the origin of free ADMA in the circulation is not definitely resolved, ADMA-containing proteins are considered the exclusive source of free ADMA. Free ADMA is generally regarded as the major endogenous regulator of NOS activity. 10 Human beings generate ~300 μmol of ADMA per day. 11 ADMA is eliminated from the body either by renal excretion or by degradation to dimethylamine and citrulline by the enzyme dimethylarginine dimethylaminohydrolase (DDAH). 12 Renal excretion accounts for only 20% of ADMA elimination. The primary route of elimination (80%) is the metabolism of ADMA through the enzyme DDAH. 1 Most ADMA, but not SDMA, is degraded to citrulline and dimethylamine by DDAH, which is widely distributed throughout the body, particularly in the liver and kidney (Fig. 1).13,14 Reduction of NO production in renal patients due to elevated ADMA levels can be attributed to reduced DDAH activity along with endothelial dysfunction and oxidative stress. 14
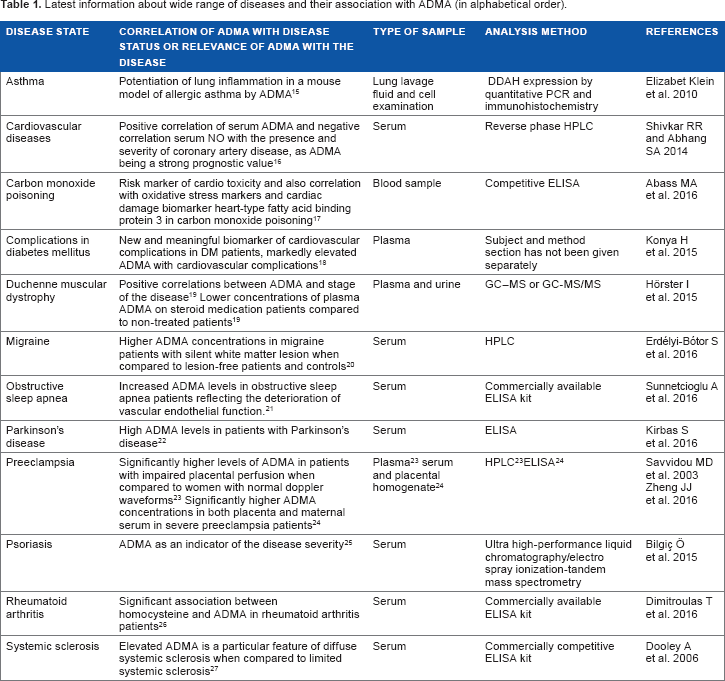
In clinical studies, a strong correlation between increased ADMA levels and impaired endothelial-dependent vasodilatation and cardiovascular morbidity and mortality has been documented in different populations, including in patients with renal disease. 8 Renal diseases, which are closely linked to endothelial dysfunction and are associated with cardiovascular morbidity and mortality, were the first among diseases in which elevated plasma levels of ADMA were reported. 2 Nowadays, in addition to renal diseases, elevated or impaired ADMA levels have been detected in a large number of diseases such as atherosclerosis, asthma, complications of diabetes, psoriasis, Parkinson's disease, migraines, preeclampsia, carbon monoxide poisoning, Duchenne muscular dystrophy, rheumatoid arthritis, obstructive sleep apnea, renal transplantation, and systemic sclerosis (Table 1). Endothelial dysfunction and free-radical damage are the intersection events throughout the course of these diseases and role of ADMA. Table 1 summarizes the role of ADMA in the aforementioned diseases.
Latest information about wide range of diseases and their association with ADMA (in alphabetical order).
Biochemical Measurement Methods of ADMA
The methods for ADMA measurement may often produce widely differing results, and few methods simultaneously offer satisfactory accuracy and precision with aspect of method validation (specificity, sensitivity, precision, accuracy, recovery, and linearity). Establishment of accurate and inclusionary reference values in different biological materials is substantial for both clinicians and researchers. Since it is related to cardiovascular risk management, high analytical precision has extreme importance to discriminate between normal and even slightly elevated concentrations of ADMA in all types of biological samples. Currently available methods for determination of ADMA include gas chromatography coupled with mass spectrometry (GC–MS), 28 high-performance liquid chromatography (HPLC) with fluorescence detection after derivatization, 29 HPLC with mass spectrometric detection (LC-MS and LC-MS/MS) underivatized30,66,67 or after derivatization, 31 and capillary electrophoresis (CE) coupled with ultraviolet32,33 or CE coupled with mass-spectrometric detection.34,35 Zinellu et al.32,33 later proposed a modified electrophoresis method in which both sample cleanup and derivatization procedures have been eliminated, thus reducing pre-analytical time and sample loss and also removing the typical problems due to derivatives’ instability. Mass spectrometric detection, either in combination with GC or LC, has been increasingly used but these methods are not ideal for routine clinical purposes because the procedures are time-consuming and the instrumentation is not always available in routine clinical laboratories.
All of these aforementioned methods are laborious and have a long turnaround period. To overcome these issues, Schulze et al developed and validated an easy to perform enzyme-linked immunosorbent assay (ELISA) method for the determination of ADMA levels in serum, plasma, or other biological fluids. Their ADMA ELISA kit is based on the principles of a competitive immunoassay. 36 Other than this, there are numerous ready-to-use ELISA kits that are commercially available for detection of ADMA. However, it should be kept in mind that an important study confirmed that ELISA measurements can overestimate ADMA levels in patients who have glomerular filtration rate (GFR) <30 mL/minute when compared to gold-standard liquid chromatographyelectrospray tandem mass spectrometry. 37 All new and emerging methods should be compared with gold-standard liquid chromatography-tandem mass spectrometry.
Discussion: ADMA as a Biomarker in Renal Diseases
The usage of biomarkers in research and in clinical routine practice as diagnostic tools has become commonplace. Their presence as primary end points in clinical trials is still a topic of interest. 38 Biomarkers are functional variants or objective quantitative indices of a biological process, which predict or reflect the evolution or predisposition to a disease or response to therapy. 39 Simply, a biomarker should provide an objective measurable value, and this value should give information about the consequences of the disease or health status of the subject.
Kidneys have dual function in ADMA metabolism; they excrete ADMA and possess high levels of DDAH. 40 As ADMA is considered as a “uremic toxin,” there is a growing datum demand from clinicians and researchers regarding levels of ADMA for nephrologic diseases. 41 It was shown that circulating ADMA concentrations decrease slowly and moderately during dialysis. After dialysis, circulating ADMA concentrations increase again, a phenomenon called rebound, and ADMA can reach higher levels compared to the baseline. 10 Increased ADMA levels in both early renal disease and ESRD are reported in many studies. 4 In a prospective observational follow-up study involving patients with type 1 diabetic nephropathy, increased ADMA was associated with a decline in GFR. 42 Patients with chronic kidney disease (CKD) are especially at increased risk of cardiovascular morbidity and mortality. Plasma ADMA levels may predict the progression of renal injury and guide the clinician during the follow-up of patients with early-stage CKD. This phenomenon could explain the high cardiovascular risk that typically accompanies renal diseases. Increased ADMA has been associated with more rapid renal disease progression and mortality.40,43 Possible mechanisms by which ADMA is involved in the pathogenesis of renal diseases 4 are:
Reduction in glomerular blood flow and ultrafiltration due to decrease in renal NO by ADMA,14,44,45
Vasoconstriction and increase in blood pressure, by impairing the endothelial-dependent relaxation and increasing the adhesion ability of endothelial cell, 11
Disturbance in intraglomerular hemodynamic state and impairment in both tubular glomerular retrograde regulation and the renal adaptation to sympathetic activity (sympathetic over activity),46,70
Increased renal oxidative stress and elevated renal levels of superoxide anion together with increased ADMA levels in serum,47,69
Induction of glomerular fibrosis and vascular fibrosis, apparently by increased collagen type I and II and fibronectin deposition, 47
Impaired amino acid metabolism due to abnormalities in synthesis or excretion, 14
Increased systolic blood pressure due to reduced plasma nitrite/nitrate levels, NO stable end-products, and a lower vasorelaxant reaction of the aortic tissues to accumulative acetylcholine concentrations, and 18
Renal parenchymal damage, resulting in reduced renal DDAH expression and activity. 4
ADMA and its role in renal incidences can be examined in detail in Table 2.
ADMA and its role in renal incidences (in alphabetical order).

Reference interval of serum ADMA levels was determined as 0.22–0.88 μmol/L (2.5th and 97.5th percentile values) in a recent study involving 120 healthy subjects aged between 34 and 61 years (mean age: 47.4 years). 60 Analogous to this information, Schulze et al. 36 found a mean ADMA level of 0.65 μmol/L in healthy subjects’ plasma by the help of ELISA. Ekim et al used HPLC to determine normal serum ADMA levels in a control group comprising 34 healthy volunteers (20 females and 14 males) with an average age of 46 years. They reported mean serum ADMA concentration as 0.37 μmol/L in their study. 61 Tsikas et al measured plasma ADMA (0.39 ± 0.06 μmol/L) and urine ADMA (3.4 ± 1.1 μmol/mmol creatinine). Their study included a healthy volunteer group consisting of five males, aged 27–64 years (mean: 33 years), and seven females, aged 24–43 years (mean: 31 years). They used a gas chromatography– tandem mass spectrometry method for the accurate quantification of ADMA in human plasma using de novo synthesized [2H3]-methyl ester ADMA as the internal standard. 28 Zhang et al performed a study regarding ADMA and its role in renal transplantation. They recruited a control group consisting of 36 people (20 males and 16 females, mean age: 46 ± 13 years) and measured mean ADMA as 0.49 ± 0.1 μmol/L by LC-fluorescence method. 56 In a study completed by Weaving et al in 2008, methylated arginines in human plasma and urine were measured by tandem mass spectrometry without need for chromatography or sample derivatization. Nine healthy volunteers were included in the study (mean age: 20.9 ± 2.5 years). Concentration of mean plasma ADMA was 0.39 ± 0.13 μmol/L and 24-hour urine ADMA was 47.8 ± 8.7 μmol/24 hours. 62 The most important source of difference in these numbers can be attributed to the method of choice applied by researchers. Age group and gender discrepancy of the studies can also add extra difference.
If concentrations of ADMA in plasma and urine of children and adolescents are to be considered, there is lack of large-scale studies. Cerbone et al investigated serum ADMA levels in 39 subclinical hypothyroidism patients and their counterpart healthy controls. ADMA concentration was reported as 0.60 ± 0.16 μmol/L for controls. 63 Another recent and valuable study involving 30 otherwise healthy children of both sexes, aged 6–18 years, who underwent minor surgery (hernia, phimosis, bone fractures, tympanostomy tube insertion, etc.) was performed to analyze plasma and urine ADMA levels. The plasma level was found as 0.61 μmol/L (0.42–1.10 μmol/L), and urine level was found as 89.8 μmol/L (51.8–162.3 μmol/L). 64 Brooks et al examined the relationship between these ADMA levels and estimated GFR in children and adolescents (n = 28) with stage 2–3 CKD and in matched intra-familial controls (n = 10, mean age: 11.3 ± 4.7 years). The plasma level of ADMA was measured as 0.8 ± 0.2 μmol/L in controls. 50 Other than plasma levels of ADMA, another biochemical aspect of the NO pathway can be the analysis of ratios. Arg/ADMA, Arg/SDMA, and ADMA/SDMA ratios are drawing increasing attention lately. El-Sadek et al conducted a research recently in which the results showed significantly higher Arg/ADMA and Arg/SDMA and significantly lower ADMA/SDMA ratios in chronic kidney pediatric patients compared to controls. 65
Challenges and Future Directions
Recent research and current information on ADMA have increased considerably both in basic and clinical settings during the previous three decades. ADMA is a good candidate to be accepted as a mediator, as a regulator, and also as a novel biomarker in many aspects. Confusion regarding the role of ADMA being a predictive biomarker and/or a prognostic biomarker can only be solved with larger and preferably randomized controlled studies including pediatric population. These studies should also focus on the mechanism of action extensively. Our increasing knowledge of the routes of synthesis and metabolism of ADMA will provide new horizons for novel mechanisms of acute or chronic renal diseases and will allow us to identify potential therapeutic opportunities through this pathway. Further studies are also needed to establish robust reference intervals of serum and urine ADMA for different ages. ADMA may exert additional largely unrevealed physiological or pathologic functions that are waiting to be enlightened.
Author Contributions
Conceived and designed the experiments: MES. Analyzed the data: MES. Wrote the first draft of the manuscript: MES. Made critical revisions: MES. The author reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
We acknowledge the authors of many excellent and valuable studies that we were unable to cite due to limitations. We also thank Dr. David T. Thomas for his valuable contribution during English editing process.