
Abstract
Bacterial meningitis (BM) is a pyogenic infection present in the subarachnoid space, potentially fatal and frequently associated with neurological sequelae. During BM, cytokines (CTs) are locally produced. We sought to determine the CTs’ clinical role as disease severity predictors in adults, which is not completely clear. Using a bead-based flow cytometric assay, levels of six CTs were determined in cerebrospinal fluid (CSF) and plasma from 18 adult BM patients and 19 uninfected controls. Long-term neurological sequelae were evaluated using the Glasgow Outcome Scale (GOS). All evaluated CTs were higher in CSF than in plasma, and the levels of CSF interleukin (IL)-6, IL-8, IL-10, IL-1β, and tumor necrosis factor-α and plasma IL-10 and IL-12p70 were significantly higher in patients with severe sepsis than with sepsis, suggesting an association with clinical severity. There was a strong negative correlation between CSF IL-6 and plasma IL-12p70 with GOS score, supporting the possible role of these CTs in the development of neurological long-term sequelae. These findings could be helpful to identify candidates to receive neuroprotective treatments and early physiotherapy schemes.
Introduction
Bacterial meningitis (BM) is a suppurative infection present in the subarachnoid space, with an annual incidence of two to six cases per 100,000 adults in the developed countries 1 and mortality up to 30%. 2 Streptococcus pneumoniae, Neisseria meningitidis, and Haemophilus influenzae are the most frequently isolated pathogens and together constitute 62% of cases, followed by Enterobacteria (3.5%), Staphylococcus (1%), and Pseudomonas spp. (0.3%), although it is known that in 33% of cases, the responsible germ cannot be identified. BM is most frequent in children, 3 but the frequency of complications and disease-associated adverse results are comparable with adults. 2 Massive application of vaccines against major etiologic agents has changed the BM epidemiology, particularly in children, but it is still unmodified in adults. 4
A critical aspect in BM pathogenesis is the effect of immunity generated against infectious agent on the central nervous system (CNS). Once inside the CNS, bacteria proliferate and release pathogen-associated molecular patterns such as lipopolysaccharide, peptidoglycan, and nucleic acids. This process derives in the activation of resident macrophages, astrocytes, and microglia through toll-like receptors 2,4, and 9, stimulating the production of cytokines (CTs).5,6 In animal models of BM, CTs such as tumor necrosis factor (TNF)-α, interleukin (IL)-1β, IL-8, and IL-6 are early expressed in the CNS after local bacteria inoculation and are detectable up to 96 hours.7,8 Some of these CTs induce increased blood-brain barrier (BBB) permeability and stimulate massive recruitment of polymorphonuclear neutrophils (PMNs). 9 Treatment with anti-TNF-α monoclonal antibodies and IL-1β receptor antagonists reduces these effects.10,11 IL-6 is produced in response to IL-1β and is a potent inducer of acute-phase proteins and fever. 12 IL-6-deficient mice have higher CNS bacterial colonization and lower survival, supporting the critical role of this CT in innate immune response in BM. 13 After the release in subarachnoid space, proinflammatory CTs increase production of reactive oxygen species 14 that bind to lipids, proteins, and nucleic acids, leading to the activation of cell death pathways. Thus, neuronal injury is a frequent consequence of BM. 15
Despite significant advances in diagnosis and treatment of BM, complications and long-term sequelae (like deafness and focal neurological deficit) are present up to 60% of cases. 16–19 Therefore, the identification of early infection biomarkers in BM is highly required. Previously, the role of proinflammatory CTs as markers for diagnostic, clinical severity, and prognosis was evaluated, and particularly, cerebrospinal fluid (CSF) IL-6 has shown usefulness.20–26 However, the association of other CTs expressed in CSF and plasma with the clinical severity or, particularly, neurological outcome of BM in adults is not clear. Here, we aimed to determine six CSF and plasma CTs in BM adult patients and uninfected controls and analyze their association with clinical severity and neurological outcome, after a six-months clinical follow-up, and we hypothesized that selective expression of local and systemic CTs could be a useful marker of the clinical outcome and long-term disabilities in adult BM patients.
Methods
Patients and samples
This study was carried out in accordance with the Universidad Surcolombiana and Hospital Universitario de Neiva ethics policies on human subject research. Patients older than 18 years with clinical suspicion of BM according to the Infectious Diseases Society of America guidelines were included. 27 A suspected BM case was a patient who presented sudden onset of illness with fever (>38.3 °C) and at least one of the following: altered consciousness, meningeal signs, with or without purpuric or petechial rash, and abnormal CSF examination (cloudy appearance, leukocyte count >10/mm3 with predominance of neutrophils, total protein >45 mg/dL, and/or glucose <40 mg/dL). A confirmed BM case was a suspected patient with positive culture (CSF and/or blood) or detection of S. pneumoniae, N. meningitidis, and H. influenzae nucleic acids in CSF by polymerase chain reaction (PCR), as described below. All included patients were seronegative for Human Immunodeficiency Virus (HIV)-1 infection.
BM patients were clinically classified based on sepsis, severe sepsis (evidence of hypotension or sepsis-induced organ dysfunction), and septic shock following International Sepsis Definitions Conference and Surviving Sepsis Campaign criteria.28,29
After signing informed consent and before establishing antibiotic adjuvant therapy (corticosteroid), 2 mL of CSF was collected in sterile tubes, by standard lumbar puncture. Simultaneously, 2 mL of venous peripheral blood was taken in tubes with ethylenediaminetetraacetic acid (BD Biosciences). All samples were collected within the first 12 hours of hospital admission. A fraction of sample was also used for cytochemical and microbiological examination of CSF. Samples were centrifuged at 300 × g for 10 minutes, and CSF and plasma were stored at -70 °C until analysis. In one BM patient, plasma was not available. As controls were included adult patients who underwent nonemergency surgical procedures with spinal anesthesia by noninfectious causes. All experiments followed the principles expressed in the Declaration of Helsinki.
Microbiological confirmation
Gram staining, aerobic and anaerobic cultures, latex agglutination tests, and conventional PCR plus hybridization were used to identify causative bacterial agents. For the latter, Speed-Oligo Bacterial Meningitis kit (Vircell, Ref: SP006) was used, according to the manufacturer's instructions. To rule out fungal and tuberculous meningitis, KOH and Ziehl Neelsen stain, respectively, were used. Herpes simplex virus 1 encephalitis was also excluded by Real Time PCR. In eight patients, it was not possible to isolate the causative agent. However, based on clinical symptoms, CSF cytochemical findings, and therapeutic response to the antibiotic treatment, these patients were also included, as done previously.22,27
Evaluation of CSF and plasma CTs
CSF and plasma IL-6, IL-8, IL-10, IL-1β, IL-12p70, and TNF-α were measured by cytometric bead array (CBA), using Human Inflammatory Cytokine kit (BD Biosciences, Cat: 551811), following all manufacturer's recommendations. Samples were acquired in an FACS Canto II (BD Biosciences) flow cytometer, within an hour following the procedure. Detection limits (in pg/mL) to IL-6, IL-8, IL-10, IL-1β, IL-12p70, and TNF-α were 2.5, 3.6, 3.3, 7.2, 1.9, and 3.7, respectively. Samples were analyzed by duplicate, and variability <10% was noted. Only experiments with standard curves with R 2 > 0.98 and significant P to all CTs were included. FACS Diva (version 6.1.3) and FCAP (version 3.0.14) software, both from BD Sciences, were used for acquisition of beads and calculation of levels of CTs, respectively. To corroborate CBA results, CSF and plasma levels of TNF-α were also evaluated by ELISA using a commercial kit (R&D, DuoSet, Cat: DY210), according to manufacturer's recommendations. The detection limit of assay was 3 pg/mL.
Clinical follow-up and sequelae evaluation
Clinical and laboratory follow-ups through hospitalization were done to all patients. After hospital discharge, in a fraction of patients, a monthly telephonic follow-up was done and, after six months, Glasgow Outcome Scale (GOS) to identify neurological sequelae was performed in a programed patient visit to the Neurology Department of the Hospital Universitario de Neiva. GOS was applied as follows: (1) death (by infectious event), (2) vegetative state (the patient is unable to interact with the environment), (3) severe disability (the patient is unable to live independently but can follow commands), (4) moderate disability (the patient is capable of living independently but unable to return to work or school), and (5) mild or no disability (the patient is able to return to work or school). Evaluation of neurological sequelae by GOS has been widely used.22,30–32
Statistical analysis
Data are presented as medians and ranges. Statistical analysis was done with GraphPad Prism 6.0 for MAC software (GraphPad Software) using nonparametric tests. To determine differences between two or more independent groups, Mann-Whitney and Kruskal-Wallis tests were used. If the P-value of Kruskal-Wallis test was <0.05, Dunn's post hoc test was done. The correlation between variables was determined with Spearman correlation test. The cutoff of CT levels to predict severity was evaluated using receiver operating characteristic (ROC) curves. Better cutoff of each CT was chosen using Youden's index (sensitivity + specificity – 1). Frequency analysis was made with Fisher's exact test. In all cases, P-value < 0.05 was considered significant. For statistical purpose, for the samples with CT levels below assay limit of detection, a value equal to half thereof was assigned.
Results
Included patients
In this study, 18 BM patients (including two fatal cases) and 19 controls were analyzed. In 10 BM patients, it was possible to identify the infecting microorganism. The most frequently isolated bacteria were S. pneumoniae in six cases (60%), followed by N. meningitidis and H. influenzae in two subjects each (20%). Fourteen (78%) patients presented sepsis, and four patients developed severe sepsis (22%); there was no case of septic shock. Table 1 shows clinical and laboratory characteristics of included patients classified according to clinical severity. All patients presented systemic inflammatory-response signs such as fever and leukocytosis, without significant differences between sepsis and severe sepsis (P > 0.1, Mann-Whitney test). Furthermore, classic clinical manifestations of BM such as headache and meningeal signs were similar between both groups (P > 0.05, Fisher's test). Other neurological abnormalities were found in patients with sepsis and severe sepsis, respectively, as follows: Glasgow coma scale <12 in 14% and 25% and behavioral disturbances (confusion, irritability, disorientation) in 39% and 60%; furthermore, patients with sepsis presented seizures (28%) and focal neurological signs (14%). However, there were no significant differences in the frequency of these clinical manifestations between both BM groups (P > 0.05, Fisher's test). C-reactive protein was significantly higher in severe sepsis patients in comparison with sepsis patients, median (range) of 5.3 (0.5–28.6) in sepsis and 21.7 (20.8–29.4) in severe sepsis (P= 0.02, Mann-Whitney test). CSF characteristics such as high opening pressure, neutrophilic pleocytosis, increased proteins, and decreased glucose levels were similar, but leukocytes in CSF and blood were significantly higher in severe sepsis than in sepsis (Table 1). In summary, clinical and laboratory differences were found between BM groups.
Clinical and laboratory characteristics of patients cohort.

Notes:
Kruskal-Wallis test.
Fisher's test.
Mann-Whitney test.
P = 0.01 controls vs sepsis.
P = 0.001 controls vs severe sepsis.
CTs are locally increased in BM
Through CBA, levels of IL-6, IL-8, IL-10, IL-1β, IL-12p70, and TNF-α in pared CSF and plasma samples from BM patients and uninfected controls were evaluated. As shown in Figure 1, all CSF CTs were significantly higher in BM patients than in controls (P < 0.0001 for IL-6, IL-8, and IL-10; P = 0.01 for IL-1β; P = 0.0002 for IL-12p70; and P = 0.04 for TNF-α, Mann-Whitney test). For IL-6 and IL-12p70, there were also significant differences in plasma of BM compared with that of controls (P < 0.0001 and P = 0.002, respectively, Mann-Whitney test). Unexpectedly, of 18 analyzed BM patients, only four had detectable levels of CSF TNF-α. As TNF-α is critical for cellular activation and BBB disruption and previous reports have shown high CSF and plasma levels in BM patients,33,34 the CBA results were corroborated by ELISA. As shown in Supplementary Figure 1 and consistent with CBA results, CSF TNF-α was undetectable in most BM patients. In brief, BM induced the expression of differential patterns of CTs in the CNS and systemic compartments.
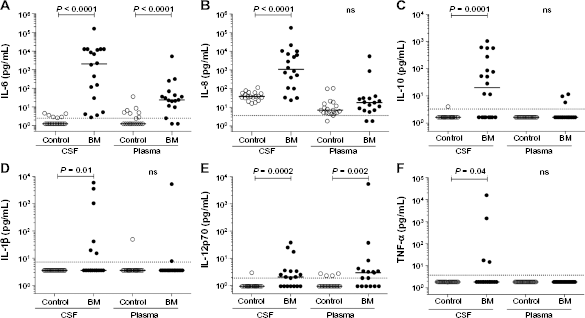
CT levels in CSF and plasma from BM patients. CSF and plasma IL-6 (A), IL-8 (B), IL-10 (C), IL-1β (D), IL-12p70 (E), and TNF-α (
Increased BBB permeability during BM is a critical aspect in its pathophysiology, and CTs locally produced during infection are probably released to systemic circulation. To evaluate this possibility, the correlation between plasma and CSF CT levels was determined. Only for IL-10, a moderate positive correlation was found (rho = 0.69, P = 0.004, Spearman test, data not shown), suggesting that CTs are generally confined to CNS and support a compartmentalized immune response in BM.
CTs locally secreted are higher in severe forms of BM
Using ROC curves analysis, we established the capability of each CT to discriminate between sepsis and severe sepsis. As shown in Table 2, CSF IL-6, IL-8, IL-10, IL-1β, and TNF-α had a strong discriminative capability between sepsis and severe sepsis (area under curve [AUC] ≥0.90 and P ≤ 0.01 for all of them) and sensitivity and specificity of selected cutoff values were ≥75% in all cases (Table 2). Interestingly, for plasma CTs, only IL-12p70 had a strong discriminative capability (AUC = 0.9, P = 0.01, Table 2). Thus, CSF and plasma CT levels could be useful to early identify severely ill patients.
Capability of CSF and plasma CTs to predict clinical severity in BM adult patients.

Selective patterns of CTs in CSF and plasma are associated with neurological sequelae in BM
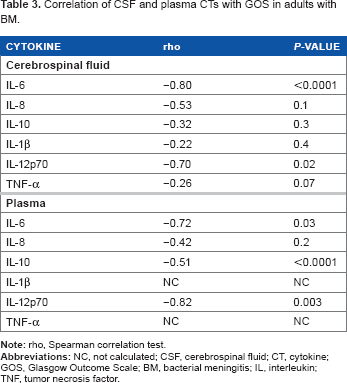
In eight BM patients (six sepsis and two severe sepsis cases), clinical follow-up and neurological evaluation were realized up to six months after infection. As shown in Table 3, a strong negative relationship between the level of CT and GOS score was found only for CSF IL-6 and plasma IL-12p70 (rho = –0.80, P < 0.0001, and rho = –-0.82, P = 0.003, respectively, Spearman test), indicating that these CTs could be associated with sequelae presentation in BM. Of note, plasma TNF-α and IL-1β correlation with GOS was unable to be calculated because all values were under detection limit of assay.
Correlation of CSF and plasma CTs with GOS in adults with BM.
Discussion
Herein, six CTs in pared CSF and plasma samples from adult BM patients were evaluated, and their utility to discriminate between major or minor clinical severity and development of neurological sequelae was analyzed. Eighteen suspected BM patients were included, and overall microbiological confirmation was obtained in 56%, according to previous reports.3,22
Experimental animal models of BM have shown that clinical severity is related to the magnitude of inflammatory process in CNS, and their immunomodulation could be key in the treatment of this infectious disease. 35 In agreement with previous reports,33,36,37 we found high concentrations of CTs in CSF of BM patients (Fig. 1). CSF TNF-α level was below assay limit of detection in a high number of BM patients (Fig. IF and Supplementary Fig. 1). Of note, dynamics of this CT is peculiar. In murine BM models, CSF TNF-α is produced within six hours of infection, and its level is almost undetectable after 24 hours. 7 In humans, TNF-α disappears in 24 hours from CSF after establishing the antibiotic treatment. 38 Unlike TNF-α, half-life of other proinflammatory CTs is longer, and high levels of them are found 96 hours after onset of infection in animals.7,39,40 We acknowledge that, in our study, it was not possible to accurately determine the time elapsed after the CNS infection; however, all the patients were admitted to the hospital between 24 and 48 hours of the beginning of symptoms, which could explain the low frequency of patients where CSF TNF-α was detectable (Fig. IF and Supplementary Fig. 1). Therefore, dynamics of local human CTs induced by CNS infection seems to be a critical and still unknown factor where future studies are necessary.
In animal models, it has been shown that response of CTs in BM is compartmentalized. 41 For example, CTs production is dependent of CN S bacterial load, explaining the higher levels in CSF than in plasma.42,43 Consistently, we did not find the correlation between CSF and plasma levels for most of the tested CTs, indicating that, despite increased BBB permeability, CTs cannot easily cross it, promoting the local inflammatory process and neuronal tissue damage. 44 Although high levels of CTs were found in CSF and plasma of BM patients, CSF could not be the source of plasma circulating CTs. However, CTs like IL-10 have transporters from CNS to circulation, but they are quickly saturable, 45 which could possibly explain the moderate positive correlation between CSF and plasma levels found for this CT (data not shown).
Previous studies have shown an association between inflammatory CSF CT levels in BM patients with clinical severity,43,46 consistent with what is found here (Table 2). Although some studies have evaluated the association of inflammatory CTs in septic process with clinical outcome, 47 a few have assessed it according to sepsis classification in BM. 48 In accordance with previous results, TNF-α is particular. 43 All few cases with detectable levels of this CT corresponded to severe sepsis patients, supporting its possible utility as a biomarker associated with severe forms of disease. Interestingly, an important discriminative capability was found between both clinical groups to plasma but not CSF IL-12p70. A study that analyzed IL-12p70 (active form) and IL-12p40 (inactive subunit and competitive antagonist of IL-12 receptor) in pared CSF and plasma of children with BM found higher levels of the inactive subunit in CSF in comparison with plasma, while the active form was detected in similar concentrations. 49 We propose that the measurement of IL-12p70 in plasma could be useful to identify and follow-up patients with severe sepsis in BM adults.
Severe disease is also associated with poor prognosis and neurological long-term sequelae.31,50,51 Some inflammatory CTs in CSF have shown to be useful as biomarkers’ predictors of sequelae after infection.24,25,52 In our study, IL-6 in CSF and IL-12p70 in plasma correlated strongly with neurological sequelae degree. In agreement with our results, in septic processes 53 and BM, higher IL-6 levels have been found in patients who do not survive to acute infectious events, 25 and increased levels of this CT are associated with poor prognosis. 24 Comparable findings have been shown for CSF IL-8. 34 IL-6 is a potent inducer of PMN migration to CNS, and in rat model of pneumococcal meningitis, the blocking of this CT resulted in lower pleocytosis and local protein content. 54 Therefore, higher levels of proinflammatory CTs (like the IL-6) lead to neuronal injury and worse clinical outcome. Thus, two of six locally secreted CTs were associated with severity, and one of them was related with a clinical outcome in adults with BM. However, more studies with a larger number of patients will be necessary to establish the accurate usefulness.
In summary, high inflammatory CSF CT levels in BM patients were found, apparently their secretion is confined to CNS, and these levels were positively associated with severe forms of disease and possibly with clinical outcome.
Conclusion
CSF IL-6 and plasma IL-12p70 could be helpful to establish neurological recovery and identify adults with BM who would benefit of additional neuroprotective treatments or early rehabilitation programs.
Author Contributions
Collected CSF and serum samples: MAT. Performed laboratory experiments: FP-C, MAT. Designed the study and critically evaluated the results: HO, JG-A, VM, LFD, GG, CFN. Analyzed the results and wrote the manuscript: FP-C, CFN. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
We would like to thank the patients who participated in the study and Departamento de Medicina Interna, Universidad Surcolombiana, and Hospital Universitario de Neiva. Also, we would like to thank German Pastrana, Juan Torres, and Juan Parra for their help in collecting the CSF and plasma samples.