
Abstract
Molecular analysis of sputum can help diagnose lung cancer. We have demonstrated that Lung Flute can be used to collect sputum from individuals who cannot spontaneously expectorate sputum. The objective of this study is to further evaluate the performance of the Lung Flute by comparing the characteristics of parallel samples collected with and without the Lung Flute and the usefulness for diagnosis of lung cancer. Fifty-six early-stage lung cancer patients (40 current smokers and 16 former smokers) and 73 cancer-free individuals
Introduction
Cigarette smoking is the highest single risk factor for lung cancer. 1 With the reduction in the prevalence of smoking, lung cancer has become more frequent among former smokers than current smokers. 2 For instance, in a cohort study of more than 5,000 patients whose lung cancer was diagnosed between 1997 and 2002, only 25% were current smokers and more than 60% were former smokers. 2 An National Cancer Institute (NCI)–National Lung Screening Trail showed that the early detection of lung cancer by using low-dose computed tomography (LDCT) followed by appropriate treatments significantly reduced the mortality. 3 Non–small-cell lung cancer (NSCLC) accounts for 85% of all lung cancer cases. Therefore, LDCT is recently recommended to be used for NSCLC screening in smokers. 4 The computed tomography (CT) scan has dramatically increased the number of indeterminate pulmonary nodules in asymptomatic smokers. However, 96.4% of the pulmonary nodules were ultimately confirmed as false positives. 5 Therefore, LDCT screening for lung cancer has a low specificity.5,6 Radiology-based noninvasive and biopsy-based invasive techniques are presently used for the management of CT-discovered indeterminate pulmonary nodules. 7 Yet the noninvasive approaches may cause unnecessary procedures, radiation exposure, anxiety, and cost. Furthermore, biopsies have risks of pneumothorax, hemorrhage, and false-negative results. Therefore, it is imperative to develop noninvasive approaches that can supplement LDCT for the diagnosis of NSCLC. 5
Sputum is an easily available fluid that comprises exfoliated airway epitheliums of the lungs. 8 Cytological study of sputum can detect morphological abnormalities of bronchial epithelial cells under microscopy. However, the sensitivity of sputum cytology is very poor. 9 Studying sputum by using molecular approaches could detect cancer-related abnormalities that cannot be found under microscopy, thus presenting a potential tool for the diagnosis of NSCLC. 10–12 For example, we previously found that expression levels of 13 miRNAs (miRs-21, 31, 126, 143, 155, 182, 200b, 205, 210, 372, 375, 486, and 708) in sputum were associated with lung cancer.13–17 We further developed a set of sputum miRNA biomarkers (miRs-21, 31, and 210), which could diagnose lung cancer with a higher sensitivity compared with sputum cytology. 18 Therefore, the analysis of sputum miRNAs may provide a noninvasive tool for facilitating diagnosing NSCLC.
However, some subjects, particularly former smokers, are unable to spontaneously expectorate sputum, presenting a major obstacle in cytological and molecular diagnosis of lung cancer in sputum.19,20 To overcome this clinical challenge, we previously used Lung Flute to collect sputum. 19 The Lung Flute is a Food and Drug Administration (FDA)-cleared noninvasive, self-powered audio, and drug-free plastic device that was initially used as a therapeutic tool for numerous chronic pulmonary conditions. 21 It can generate sound waves, which is created by exhalation. Sound waves increase the clearance of mucus, thus making discharges of mucus easily expelled through coughing. Using the Lung Flute, we successfully collected sputum within 20 minutes from individuals who cannot expectorate sputum. 19 No adverse effect was observed. 19
The objective of this study is to further evaluate the performance of the Lung Flute by comparing the characteristics of parallel samples collected with and without the Lung Flute and the potential usefulness for diagnosis of lung cancer. Our results show that sputum collected by the Lung Flute exhibit comparable features as spontaneously expectorated sputum, and are of low respiratory origin without contamination from other sources. Using the Lung Flute may improve cytological and molecular analyses of sputum for the diagnosis of NSCLC.
Materials and Methods
Patients and sample collection and preparation
The study was approved by the Institutional Review Boards of the University of Maryland Medical Center and the Baltimore Veterans Affairs (VA) Medical Center. All patients with lung cancer and control subjects were selected and consented when they visited the clinics of the Division of Pulmonary and Critical Care in the two medical centers. Final clinical diagnoses for the lung cancer patients were confirmed by histopathologically examining biopsy or surgically resected tissue specimens. The histopathological classification and staging were decided based on the Tumour, Node, Metastases (TNM) classification as previously described.15–18 Control individuals were subjects aged 55–74 who had more than 30 pack-year smoking history and no prior history of any cancer. The smokers who had quit within the previous 15 years were considered as former smokers. Furthermore, all control individuals remained cancer free for a minimum 2-year follow-up. This research complied with the principles of the Declaration of Helsinki.
Sputum collection and preparation and sputum cytology
Collecting sputum was performed before any treatment regimen (eg, surgery, preoperative adjuvant chemotherapy, and radiotherapy). To reduce food and salivary contamination in sputum, the participants rinsed their mouth out with water and gargled three times before using the Lung Flute or spontaneously expectorating. Sputum was first collected into a sterile container by spontaneously coughing as described in our previous studies.13,14,16–18,22–26 After 1 hour, the participants were asked to rinse their mouth out with water three times again and instructed to use the Lung Flute (Medical Acoustics, Buffalo, NY, USA) for sputum sampling.19,21,27 Briefly, the subjects were asked to blow their nose and rinse their mouth to further diminish contamination of squamous cells from postnasal drip and mouth, blow out through Lung Flute, and cough up sputum into a sterilized cup. The collected sputum was immediately put on ice in dithiothreitol (Sigma-Aldrich Corporation, Saint Louis, MO, USA). The sputum samples were then centrifuged at 800
Isolation of RNA and analysis of miRNAs by real-time quantitative reverse transcription-polymerase chain reaction
RNA was isolated from the sputum samples by using a protocol developed in our previous studies. 13–18 The purity and concentration of RNA and RNA integrity were determined by using the methods as described in our previous reports. 15–18 Three miRNAs, miRs-21, 31, and 210, were previously identified as potential sputum miRNA biomarkers for lung cancer.15–18 In this study, the three miRNAs were evaluated for the expression in sputum by using quantitative reverse transcription-polymerase chain reaction (qRT-PCR) with Taqman miRNA assays (Applied Biosystems, Foster City, CA, USA).13–18 U6 was used as an internal control gene to normalize threshold cycle (Ct) values of the three miRNAs. We performed all assays in triplicates. Each experiment included one no-template control and two interplate controls.
Statistical analysis
Continuous variables were compared using /-tests, and categorical variables were compared using Fisher's exact test. Pearson's correlation coefficient tests with multivariate regression analysis were used to evaluate the relations between expressions of the miRNAs and characteristics of the cases and controls. Receiver operating characteristic curve and the area under the curve (AUC) analyses were employed to determine performance of miRNAs. 30
Results
Subject characteristics
The 56 lung cancer patients had a median age of 68.4 years (Table 1). Of them, 36 (64.3%) were men and 39 (69.3%) were White Americans. The lung cancer cases were stage I NSCLC. The cancer patients were smokers with a median of 38.3 pack-years of smoking. Among the 56 NSCLC cases, 40 (71.4%) were current smokers, while 16 (28.6%) were former smokers. Thirty-one (55.3%) were adenocarcinoma (AC) and 25 (44.7%) were squamous cell carcinoma (SCC). The 73 cancer-free smokers had a median age of 67.8 years and a median of 36.4 pack-years of smoking. Forty-seven (64.4%) were men and 52 (71.2%) were White Americans. Fifty-two (71.2%) were present smokers, while 21 (28.8%) were former smokers. In total, there were 92 current smokers and 37 former smokers in all cases and controls. There was no statistically significant difference of the age, race, and smoking status between the two groups (all
The demographic and clinical variables of NSCLC patients and cancer-free smokers.

Notes:
Former smokers are individuals who quit smoking within the last 15 years.
AII
Collection of sputum by using spontaneous coughing and the Lung Flute
All 92 current smokers, including 40 NSCLC cases and 52 controls, could easily cough sputum. When using the Lung Flute, they also produced sputum. Of the 37 former smokers (16 NSCLC patients and 21 cancer-free controls), only 7 (18.9%) were able to spontaneously expectorate sputum; however, 30 (81.8%) could not spontaneously expectorate sputum. Of the seven former smokers who were able to spontaneously expectorate sputum, there were three NSCLC patients and four controls. The 30 former smokers, who could not spontaneously expectorate sputum, included 13 NSCLC patients and 17 controls. If using the Lung Flute, however, all the 37 former smokers were able to produce sputum. Overall, the success rate of colleting sputum was 76.7% (92/129) for spontaneous coughing, whereas it was 100% (129/129) for the Lung Flute
Sputum collected by the Lung Flute has comparable characteristics as spontaneously expectorated sputum.

Comparison of characteristics of sputum samples collected by spontaneous coughing and the Lung Flute
As shown in Table 2, the median volume of sample collected by spontaneous coughing was 2.7 mL, while the median volume of sample obtained by the Lung Flute was 2.6 mL

Cytological examination of sputum (Papanicolaou's stain; original magnification ×40). (
Comparison of diagnostic efficiency of cytology and molecular analysis in sputum collected by spontaneous coughing and the Lung Flute
Cytology had 46.51% sensitivity and 89.29% specificity for the identification of NSCLC in sputum collected by the Lung Flute, 46.43% sensitivity and 89.04% specificity in sputum collected by spontaneous coughing (all
qRT-PCR for quantification of miRNA expression was successfully undertaken in the specimens, since all three miRNAs had ≤30 Ct values in each sputum sample. The three miRNAs displayed a significantly different level between NSCLC patients and control subjects (all
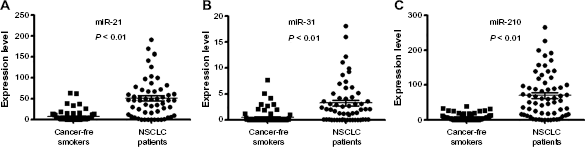
The expression levels of the three miRNAs in sputum collected by the Lung Flute from 56 patients diagnosed with stage I NSCLC and 73 cancer-free smokers. Horizontal lines denote mean values. The three miRNAs (A–C) show statistical significance of expression levels between NSCLC patients and cancer-free smokers (all
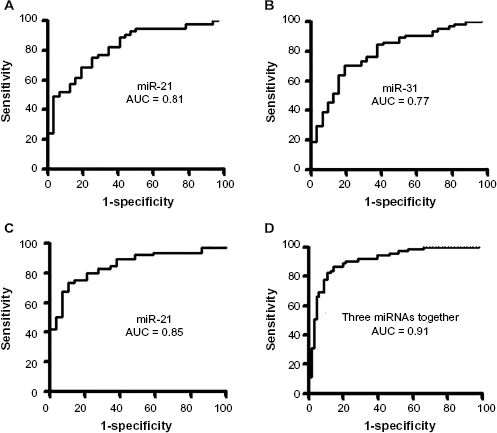
Receiver-operating characteristic (ROC) curve analysis of expression levels of the three miRNAs in sputum collected by the Lung Flute in 56 patients diagnosed with stage I NSCLC and 73 cancer-free smokers. The AUC for each miRNA conveys its accuracy for differentiation of NSCLC patients and cancer-free smokers in terms of sensitivity and specificity. The individual genes produce 0.77–0.85 AUC values (A–C), being significantly lower than 0.91 AUC created by combined use of the three genes (
Expression levels of miRNAs in sputum collected by the Lung Flute from NSCLC patients and cancer-free smokers.

Comparison of sputum cytology and miRNA panel in sputum collected by the Lung Flute showed that the sputum miRNA biomarkers had a higher sensitivity (83.93%) compared with sputum cytology (46.51%), while maintaining a similar specificity (87.67% vs. 89.29%,
Discussion
Very often some subjects, particularly former smokers, are unable to spontaneously expectorate sputum, presenting a major clinical challenge in developing sputum biomarkers. Overcoming this difficulty is becoming more clinically important, since lung cancer is now predominant among former rather than current smokers, with the decline in smoking. 2 To address the challenge, we previously used Lung Flute for sputum sampling and found that Lung Flute could be used to collect sputum from persons who could not spontaneously cough sputum. 19 To extend our previous study, here we assess the diagnostic performance of the Lung Flute by evaluating the characteristics of the parallel samples collected by using the two different approaches in smokers. Using the Lung Flute, we not only collect sputum from all current smokers, but the former smokers who cannot spontaneously cough sputum. Furthermore, the collected sputum samples by the Lung Flute have at least 2 × 107 cells/mL, suggesting the sputum samples have enough cell number for downstream cytological and molecular analysis. In addition, each sputum sample has less than 4% oral squamous cells and more than 50% alveolar macrophages. The findings strongly suggest that the sputum samples are of low respiratory origin without contamination from other sources, eg, saliva. Moreover, our head-to-head comparison shows no statistical diagnostic difference of sputum cytology for lung cancer in specimens collected by the two approaches. Sputum collected by the Lung Flute has equal features as spontaneously expectorated sputum. The Lung Flute was well tolerated by all participants. Altogether, the use of Lung Flute may overcome one of the obstacles in cytological diagnosis of NSCLC by efficiently collecting appropriate sputum from smokers.
Molecular analysis of sputum can identify the cells that contain cancer-related abnormalities and might be more sensitive than cytology for diagnosis of lung cancer. 8 We recently developed a panel of three sputum miRNA biomarkers (miRs-21, 31, and 210) for lung cancer. 18 In this current study, we successfully validate the three miRNA biomarkers in sputum collected by the Lung Flute using a different cohort of cases and controls. Furthermore, the analysis of the miRNA biomarkers in sputum collected by the Lung Flute had a greater sensitivity than sputum cytology, while keeping a similar specificity, thus confirming our previous findings.13,18 In addition, there is a similar diagnostic performance of the miRNA biomarkers in sputum collected by the two different approaches. Therefore, sputum collected by the Lung Flute may have equivalent clinical value as spontaneously expectorated sputum in molecular diagnosis of lung cancer.
There are some weaknesses in the present study. First, the sample size of cases and controls is not large enough to comprehensively validate the utility of the Lung Flute for sputum sampling. We are planning a larger scale validation study for the Lung Flute across multiple centers in a population screened by LDCT. Second, although showing promise, the panel of three sputum miRNA biomarkers only has 83.93% sensitivity and 87.67% specificity for lung cancer. Our ongoing efforts are to identify additional miRNA biomarkers that can be added to the three miRNAs to improve diagnosis of lung cancer. Third, we did not find statistical difference of sputum volume and cell populations in the specimens collected by the two approaches. We also did not observe statistical variance of the parameters in sputum samples of former versus current smokers. However, whether there is any difference in the biological characteristics of sputum samples collected by the two approaches as well as sputum samples of current versus former smokers needs to be investigated.
In summary, sputum collected by the Lung Flute has comparable characteristics as spontaneously expectorated sputum. The use of the Lung Flute may overcome one of the obstacles in the development of sputum biomarkers by safely and efficiently obtaining appropriate sputum from individuals, particularly prior smokers. Nonetheless, carrying out a multicenter clinical trial to validate the Lung Flute and the sputum miRNA biomarkers for lung cancer diagnosis in a large and prospective population is required.
Author Contributions
Conceived and designed the experiments: JS, NA, MAG, HZ, FJ. Analyzed the data: JS, NA. Wrote the first draft of the manuscript: FJ. Contributed to the writing of the manuscript: SAS. Agree with manuscript results and conclusions: JS, NA, MAG, HZ, SAS, FJ. Jointly developed the structure and arguments for the paper: SAS. Made critical revisions and approved final version: JS, NA, MAG, HZ, SAS, FJ. All authors reviewed and approved of the final manuscript.