
Abstract
The use of tyrosine kinase inhibitors (TKIs) in the treatment of solid tumors is the expected standard of care for many types of tumors. Since the description of signal transduction pathways, followed by the development of small molecules designed to inhibit those pathways, there has been significant improvement not only in progression-free survival and overall survival but also in aiming toward chemotherapy-free treatment of solid tumors to maximize quality of life. This article reviews available TKIs and discusses toxicity, dosing, and resistance.
Keywords
Introduction
Signal transduction pathways identified to induce cell proliferation in solid tumors include the growth factor receptor (ErbB/HER), the vascular endothelial growth factor receptor (VEGFR), anaplastic lymphoma kinase (ALK), MET, and KIT surface tyrosine kinases, as well as RAS/RAF/ MEK/ERK and PI3K/AKT pathways for intracellular signal transduction. 1 These signaling pathways are often abnormally upregulated and dependent on oncogenic mutations, such as exon 19 deletion and others for EGFR, 2 V600 for BRAF, 3 gene rearrangement with EML4 fusion gene for ALK, 4 and KIT for gastrointestinal stromal tumors (GISTs). 5 Since their description, there have been fruitful efforts in developing targeted drugs for effective blockade of the upregulated signaling pathways.6,7 The involvement of small inhibitory molecules (tyrosine kinase inhibitors or TKIs) binding the adenosine triphosphate site of tyrosine kinases successfully led to downregulation through autophosphorylation.
For the clinician the implications of TKIs have been revolutionary over the last decade. Following imatinib for the treatment of chronic myelogenous leukemia in 2001, there have been significant efforts taken to identify oncogenic mutations, and important advances in applying TKIs in the treatment of solid tumors. Through trials of TKIs in the treatment of tumors considered more oncogenic driven, such as renal cell cancer or melanoma, a new standard of treatment has been set. Nevertheless, expanding the use of TKIs to include treatment of other solid tumors has remained a challenge.8,9 Further research on signaling pathways has helped identify mutations that lead to enhanced signal transduction and tumor proliferation, or to pathway alterations that cause resistance to TKI treatment through feedback mechanisms.
In clinical practice, EGFR and RAS mutation analysis, applied to non-small cell lung cancer (NSCLC) and colon cancer, as well as EML4–ALK fusion gene testing in NSCLC are standards of care. In case of positivity, a chemotherapy-free first-line therapy option arises.
The issue of acquired resistance to TKIs and how this could be overcome remains a major topic of research and further trials. Moreover, the identification and handling of TKI-induced organ toxicity, especially where it leads to quality-of-life restriction, is of great importance.
This article reviews the current commercially available TKIs approved for use in the treatment of solid tumors.
Breast Cancer
In patients with HER2 overexpression and hormone receptor-positive metastatic breast cancer who had not received prior therapy for metastatic disease, lapatinib has been approved after a randomized trial with lapatinib plus letrozole vs. placebo plus letrozole. 10 Patients in the lapatinib plus letrozole group showed an improved progression-free survival (PFS) of 35.4 weeks, compared to 13.0 weeks for the placebo plus letrozole arm (hazard ratio = 0.71; P = 0.019).
In HER2 overexpressing metastatic breast cancer, lapatinib in combination with capecitabine compared with capecitabine alone in pretreated patients has shown improvement in the primary endpoint of time to progression (27.1 vs. 18.6 weeks; hazard ratio = 0.57; P = 0.001). 11
Colon Cancer
The small-molecule multikinase inhibitor, regorafenib, inhibits multiple membrane-bound and intracellular kinases, such as VEGFR, KIT, TIE2, PDGFR, FGFR, and BRAF In a phase III trial on pretreated patients with metastatic colon cancer, there was an overall survival (OS) benefit for patients treated with regorafenib (6.4 vs. 5.0 months; P=0.0052). 12
Gastrointestinal Stromal Tumors
In the presence of oncogenic mutations in one of two receptor tyrosine kinases, KIT or PDGFRA (platelet-derived growth factor receptor alpha), imatinib is the standard first-line treatment in unresectable or metastatic GISTs (Fig. 1). The majority of patients showed a response (53.7% had partial response and 27.9% had stable disease), improved survival (durable responses more than 42 weeks), and delayed disease progression.5,13 A dose escalation to 800 mg daily was tested in phase III trials, showing no significant benefit compared to 400 mg daily. 14 The authors concluded that a dose escalation can be considered in case of progression. 15 In cases of nonresectable GIST after imatinib resistance, the multitargeted TKI sunitinib showed a median time to tumor progression of 27.3 vs. 6.4 weeks for patients on placebo in a randomized trial (hazard ratio = 0.33; P < 0.0001). 16 Regorafenib has recently been approved for the treatment of GIST after the failure of imatinib and sunitinib, according to the GRID study, in which a PFS of 4.8 months was shown for regorafenib compared to 0.9 months for placebo (P < 0.001). After progression, 85% of the patients crossed over to regorafenib. 17

Patient with relapse of GIST tumor with peritoneal, adrenal, and hepatic metastasis (left images) 2 years after individual discontinuation of imatinib shows partial response after reexposure to imatinib 400 mg daily. Measurable response was shown in the liver (34.82 mm before and 29 mm after) and the left adrenal gland (40.13 mm before and 30.64 mm after). Peritoneal metastasis with thickening of the peritoneum is visible on the lower left image, showing regress on the lower right image.
Hepatocellular Carcinoma
Sorafenib in the treatment of advanced and unresectable hepatocellular carcinoma has shown a benefit in OS (10.7 vs. 7.9 months; P < 0.001), although the median time to symptomatic progression was not significantly different in the two groups (4.1 months for sorafenib vs. 4.9 months for placebo; P = 0.77). The endpoint of radiological progression was significantly different (5.5 months for the sorafenib group vs. 2.8 months for the placebo group; P < 0.001). 18
Melanoma
The identification of the BRAF mutation with the development of BRAF inhibitors has been a boon to the treatment of melanoma patients, increasing OS (84% OS after 6 months for vemurafenib vs. 64% for dacarbazine in a phase III randomized trial). The response rate of vemurafenib was up to 48% compared to 5% for dacarbazine. 19 Nevertheless, the effect of BRAF inhibition was short lasting. Further studies revealed a feedback mechanism through MEK-mediated reactivation of the ERK signaling pathway. 20 Either a dual inhibition of RAF and MEK or reexposure to BRAF inhibitor after drug holiday has been shown effective to overcome resistance.21,22 Dabrafenib, another BRAF inhibitor, has also shown effectiveness in the treatment of patients with advanced BRAF V600 mutated melanoma. 23 In a phase III trial vs. dacarbazine, there was a significant benefit in PFS (5.1 months for dabrafenib vs. 2.7 months for dacarbazine; P < 0.001), 24 but because of short duration of antitumor activity, current studies are being carried out in combination with the MEK inhibitor trametinib. 25
Non-Small Cell Lung Cancer
The use of a TKI in case of EGFR mutation positivity or EML4-ALK fusion gene evidence has become standard of care in NSCLC.
Several randomized phase III clinical trials showed benefit in PFS for patients with the upregulation of EGFR. 26 Erlotinib was tested in EGFR mutation-positive tumors in first-line treatment vs. chemotherapy in a European trial. It demonstrated a statistically significant improvement in PFS, 9.7 months compared to 5.2 months for the chemotherapy arm (P < 0.001). 2 Two Japanese trials tested gefitinib vs. chemotherapy in the first-line setting, showing PFS of 9.2 and 10.8 months for gefitinib compared to 6.3 and 5.4 months for the chemotherapy arms.27,28 The latest study was stopped after showing the above results at the interim analysis; most patients crossed over to gefitinib.
The second-generation TKI afatinib, which irreversibly blocks EGFR as well as HER2 and HER4, was tested in a phase IIb/III trial vs. best supportive care for patients with EGFR-mutated tumors, pretreated with platinum doublet and at least 3 months of EGFR-TKI gefitinib or erlotinib. There was an increase in PFS, but the primary endpoint, which was OS, was not significantly improved. In the first-line setting, afatinib showed a statistically significant difference in PFS of 11 months vs. 5.6 months in the LUX-Lung 6 trial (P < 0.001), but still no difference in OS. 29 Further sub-population analysis has been able to detect a benefit in OS in patients with a del-19 mutation (31.4 months vs. 18.4 months with chemotherapy; P = 0.02). 30
In nononcogenic-driven metastatic lung cancer, erlotinib remains an option as maintenance therapy after first-line treatment without tumor progression, 31 or after the failure of first-line or second-line chemotherapy. 32 In the metastatic setting, erlotinib showed similar PFS and OS compared to chemotherapy with docetaxel. 33
In the setting of chromosomal rearrangements of the ALK gene, the TKI crizotinib (dual TKI of MET and ALK) showed a significant benefit in median PFS (7.7 months in the crizotinib group vs. 3.0 months in the chemotherapy group; P < 0.001) in pretreated patients with advanced disease. 34 A phase III clinical trial of crizotinib as first-line treatment has also shown advantage in PFS (median 10.9 months with crizotinib vs. 7.0 months with chemotherapy; P < 0.001). The end point of significant improvement in OS was not reached, while the probability of one-year survival was 84% with crizotinib and 79% with chemotherapy. The relief of symptoms and the quality of life were greater in the crizotinib arm. 35
The potent ALK inhibitor ceritinib was approved for the second-line treatment of advanced NSCLC harboring ALK rearrangement. The majority of patients were pretreated with crizotinib. The overall response rate was 58% with a median PFS of 7 months. In the group of crizotinib pretreated patients, the response rate was 56% with a PFS of 6.9 months. The crizotinib naive patients showed 62% response rate, and the median PFS in this group had not been reached at the time of analysis. 36
Ovarian Cancer
The important role of angiogenesis in ovarian cancer has been well described, making VEGFR targeting appealing for clinical trials. 37 In a randomized trial for maintenance treatment, the VEGFR inhibitor, pazopanib, showed a median improvement in PFS of 5.6 months (hazard ratio = 0.77) vs. placebo, in 940 patients with advanced ovarian cancer who had not progressed after first-line chemotherapy; no benefit was shown in OS. 38
Pancreatic Cancer
The EGFR-TKI erlotinib has resulted in prolonged survival when added to gemcitabine for the treatment of advanced pancreatic cancer (median PFS of 6.24 months vs. 5.91 months) and increased the one-year survival to 23% for the combination therapy vs. 17% for gemcitabine monotherapy (P = 0.023). 39
Pancreatic Neuroendocrine Tumors
The antiangiogenic TKI sunitinib has shown efficacy in a phase III trial on patients with advanced, well-differentiated pancreatic neuroendocrine tumors. PFS was significantly prolonged (11.4 months for sunitinib and 5.5 months for placebo; P < 0.001). 40
Renal Cell Carcinoma
The refractory nature of renal cell carcinoma against radiation and chemotherapy led to early immunologic therapeutic approaches, such as cytokines, and observations about the efficacy of TKIs.
In a trial against interferon alfa, patients treated with sunitinib showed prolonged PFS (11 months vs. 5 months) and overall higher objective response rate (31% vs. 6%; P < 0.001). 41 The trial, conducted in 2007, put sunitinib in the first-line choice of TKI treatment for renal cancer.
Sorafenib was tested on advanced renal cell carcinoma patients in a phase III trial after the failure of prior treatment. It showed a significant improvement in PFS (5.5 months vs. 2.8 months; P < 0.001) and reduction in risk of progression of 51%. OS was 19.3 months for sorafenib and 15.9 months for the placebo group, which is not a statistically significant difference. 42
Several years later, the TKI pazopanib showed a significantly prolonged PFS compared to placebo (9.2 vs. 4.2 months) and response rate (30% vs. 3%; P < 0.001). 43 Compared to sunitinib, pazopanib showed similar efficacy but was better tolerated, 44 thus setting a second option for first-line treatment.
The antiangiogenic TKI axitinib was compared with sorafenib in a phase III trial of second-line treatment. Although OS was not significantly different (20.1 months for axitinib vs. 19.2 months for sorafenib; P = 0.3744), there was a statistically significant benefit in PFS (8.3 months for axitinib vs. 5.7 months for sorafenib; P < 0.001) that established axitinib as a second-line treatment for advanced renal cell carcinoma patients. 45
Soft Tissue Sarcomas
Two European Organisation for Research and Treatment of Cancer trials with the VEGFR-TKI pazopanib have shown significant improvement in PFS (4.6 months for pazopanib vs. 1.6 months for placebo; P < 0.001) and OS (12.5 months for pazopanib vs. 10.7 months for placebo; P = 0.25), cementing the place of pazopanib in the treatment of nonadipocytic soft tissue sarcomas after chemotherapy.46,47
Thyroid Cancer
Medullary
The TKIs vandetanib and cabozantinib are licensed for the treatment of advanced medullary thyroid cancer. Vandetanib showed a significant longer PFS vs. placebo (30.5 months vs. 19.3 months; P < 0.001) in both patients with sporadic and hereditary medullary thyroid cancer. Median PFS of vandetanib was not reached at the time of analysis, so the reported PFS concerns the predicted one. Subgroup analysis showed a higher response rate for patients with M918T mutations. 48 In the phase III trial comparing cabozantinib versus placebo, 48.2% of tumors harbored M918T RET mutations, 12% were negative, whereas for rest RET mutations status was unknown. The majority of patients suffered from sporadic medullary thyroid cancer. Cabozantinib showed a significantly longer PFS (11.2 months) vs. placebo (4 months; P < 0.001). The estimation of one year survival and progression free was estimated 47.3% for cabozantinib vs. 7.2% for placebo. 49
Differentiated
Patients with locally advanced or metastatic differentiated thyroid cancer refractory to radioactive iodine were randomized in a phase III trial to receive sorafenib vs. placebo. PFS was significantly longer for those in the sorafenib arm (10.8 vs. 5.8 months; P < 0.001), although no difference was noticed in OS. The risk of progression or death was reduced by 41% in the sorafenib arm during the double-blind phase. 50 The latest TKI that has been licensed for differentiated thyroid cancer is lenvatinib, which in a phase III trial vs. placebo showed a significantly prolonged PFS (18.3 months vs. 3.6 months, P < 0.001). 51
In Table 1, are listed the indications for use of the above described TKIs in solid tumors.
TKI lists according to the indication of use.

Exon 19 deletions or exon 21 (L858R) substitution as detected by FDA-approved test,
Dosing adaptation for renal or hepatic impairment omitted.
Discussion
Side effects
A major obstacle in treatment with TKIs is the variety and intensity of side effects that they induce (Table 2). Notable literature covers the spectrum and the adequate management of these side effects. 52 The majority of TKIs can cause gastrointestinal symptoms such as diarrhea, nausea, and emesis, as well as general symptoms including fatigue, weight loss, and anorexia. A particular feature of VEGFR–TKIs, but also indirectly a marker for successful VEGF inhibition, is the development of hypertension. The pathomechanism relies on the decrease of nitric oxide (NO) production after VEGF serum levels are reduced. Moreover, downregulation of VEGF causes endothelin dysfunction and renal podocyte cell dysregulation. These can also be responsible for hypertension and cause proteinuria. 53 The most appropriate antihypertensive treatment is angiotensin-converting enzyme inhibitors or angiotensin II receptor blockers, mainly because of nephroprotective ability. 54 Additionally, the use of long-acting nitrates in order to overcome the vasoconstriction caused by NO suppression is very effective in the management of VEGFR inhibition induced hypertension. 55 Further side effects of VEGFR-TKIs can include hemorrhage and impaired wound healing (Fig. 2).

Impaired wound healing after gluteal abscess under pazopanib and later axitinib treatment for metastatic renal cell cancer. Osteosynthesis material of the hip after surgery for fracture because metastasis is visible.
Metabolism and common side effects of TKIs.6,4,52,54
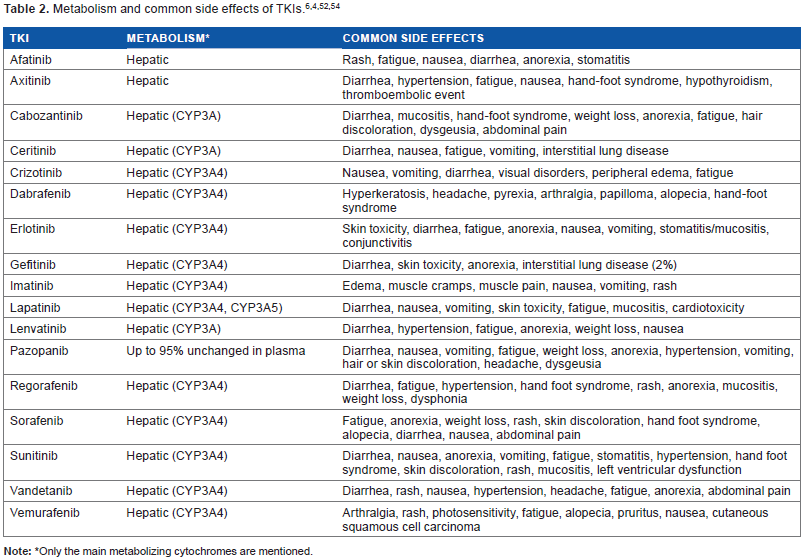
Only the main metabolizing cytochromes are mentioned.
Resistance Mechanisms
The restricted efficacy of TKIs compared to the length of survival achieved after immunotherapy remains a major drawback and raises further discussion regarding mechanisms of resistance. It mainly concerns upregulation through bypass pathways (upregulation of MET, overexpression of HER3, activation of IGF-1R, loss or downregulation of PTEN, abnormal dimerization of STAT3) or acquired receptor mutations (EGFR-T790M, HER2, PIK3CA/AKT mutations). 56 Moreover, the inability of TKIs to eliminate cancer stem cells presumably attributes to relapse under TKI treatment. 57 Approaches to overcome resistance to TKIs include the development of multitargeted agents, such as new-generation EGFR–TKIs and inhibitors of MET, IGF-1R, HER3, PIK3 A/AKT, ERK, or STAT3. 58 The use, safety, and efficacy of these agents in clinical practice, as monotherapy or in combination with already licensed TKIs, is the subject of further clinical trials.
The development of resistance to ALK TKIs has been attributed to acquired secondary mutations of the kinase domain, amplification of the ALK gene or activation of alternative signaling pathways (EGFR, c-KIT). The second generation ALK TKI ceritinib was effective through more potent inhibition. 59 In BRAF mutant melanoma, resistance mechanisms that have been studied revealed an increase in the amount of RAF dimers in tumor cells or bypass of RAF dependence for cell proliferation. 60 The dual blockade of RAF and MEK, in order to effectively inhibit the ERK signaling pathway, has been tested in trials after development of RAF resistance but showed rather modest efficacy and increased toxicity. Dual inhibition in first-line treatment appeared to be more effective in prolongation of PFS.22,25
Pharmacokinetics
The majority of TKIs are metabolized hepatically and commonly show interactions mainly through CYP3A4 induction. An individualized dosing approach applied through therapeutic drug monitoring may be indicated in order to avoid undertreatment or toxicity. 61
Conclusion
The past decade has been one of major importance for cancer therapy with TKIs, as many milestones have been reached in the development of targeted cancer therapies along with monoclonal antibodies. Although TKIs are well established in the treatment of solid tumors, such as renal cell carcinoma, melanoma, or GIST, their efficacy for other solid tumors still remains dubious. The future of TKIs remains challenging in terms of combination regimes, optimizing dosing, or broadening of the therapeutic spectrum. Studies to overcome resistance, enhance knowledge on pharmacokinetics, and manage side effects could provide effective future approaches to improve the efficacy of cancer treatment while preserving the quality of life.
Author Contributions
Conceived the concepts: MV. Wrote the first draft of the manuscript: M V. Developed the structure and arguments for the paper: MV. Made critical revisions: MV. The author reviewed and approved of the final manuscript.