
Abstract
The discovery of the mammalian target of rapamycin (mTOR) molecular pathway has brought insight into its vital role in breast cancer pathogenesis. Several clinical trials have shown that the mTOR inhibitor everolimus could improve patient outcomes in several subtypes of breast cancer, including hormone receptor–positive, human epidermal growth factor receptor–negative metastatic disease that has progressed after prior endocrine therapy. This review summarizes findings from clinical trials that have demonstrated the benefit of everolimus in metastatic breast cancer and highlights some new research directions utilizing everolimus.
Introduction
Our understanding of the molecular pathogenesis of breast cancer has evolved exponentially since the discovery of the role of estrogen in this disease. In recent years, increased understanding of the multiple subtypes of breast cancer has led to the development of many new therapeutic targets specific to each tumor's molecular pathogenesis. 1
Approximately 75% of patients with breast cancer in both early- and advanced-stage disease have hormone receptor– positive (HR-positive) tumors. This subtype of breast cancer initially shows a high overall response rate to hormonal treatments such as selective estrogen receptor (ER) modulators (eg, tamoxifen), selective ER down-regulators (eg, fulvestrant), and aromatase inhibitors (ie, anastrozole, letrozole, and exemestane). 2 Nevertheless, resistance to endocrine therapies eventually develops. 1 In addition, some tumors have de novo resistance to endocrine therapy. Both de novo and acquired resistance result in tumor progression; thus, overcoming such resistance is important for the management of HR-positive breast cancer.1,2
The PI3K/Akt/mTOR pathway regulates several cellular functions in cancer, including cell growth, survival, and proliferation. 3 The increased activation of the PI3K/Akt/mTOR pathway is one mechanism of resistance to endocrine therapy. 3 Mammalian target of rapamycin (mTOR) is a modulator of both cell growth and proliferative signals. 3 mTOR is a serine/threonine kinase and a member of the phosphatidylinositol 3-kinase (PI3K)–related kinase family, which includes PI3K, DNA protein kinase, and ataxia telangiectasia mutated. 4 mTOR is a key integrator of signals governing protein and lipid biosynthesis and growth factor–driven cell cycle progression.3,4 The inhibition of mTOR leads to a cascade of events primarily by activating downstream protein kinases that are required for both ribosomal biosynthesis and translation of key mRNAs of proteins required for transition from G1 to S phase.3,4 mTOR functions to regulate the cellular signaling processes in two cellular complexes: mTOR complex 1 (mTORC1) and mTOR complex 2 (mTORC2). 3 Although in normal cells, hypoxia, nutrient deprivation, and DNA damage restrain mTORC1 activity, multiple genetic events constitutively activate mTOR in cancers. 4 mTOR drives cancer growth by activating the lipid and protein biosynthesis needed for robust tumor proliferation. 5
The mTOR inhibitor everolimus, a derivative of sirolimus (also known as rapamycin), binds with high affinity to its intracellular receptor, FKBP12, a protein belonging to the immunophilin family. 6 The everolimus–FKBP12 complex inhibits mTOR to prevent the downstream signaling required for cell cycle progression, cell growth, and proliferation (Fig. 1).6,7 Single-agent daily or weekly everolimus treatment in a phase II study of patients with metastatic breast cancer demonstrated modest clinical activity, with a response rate ranging from 0% to 12%. 8 However, everolimus in combination with exemestane has been investigated in patients with metastatic breast cancer resistant to hormone therapies and has demonstrated improved patient outcomes, 9 leading to US Food and Drug Administration (FDA) approval for this indication. 10 In 2012, the National Comprehensive Cancer Network guidelines added the everolimus/exemestane combination as part of its treatment recommendations for HR-positive metastatic breast cancer. 11 The positive outcomes of therapy with the everolimus plus exemestane combination 9 demonstrated that blocking an escape pathway clinically restores hormone sensitivity in breast cancer.

Inhibition of mTOR by everolimus.
Everolimus in HR-Positive Disease
BOLERO-2 (Breast Cancer Trial of Oral Everolimus-2) study
Based on the results of the randomized, phase III BOLERO-2 study, the everolimus plus exemestane combination was approved by the FDA for the treatment of HR-positive, human epidermal growth factor receptor 2 (HER2)–negative metastatic breast cancer after failure of treatment with letrozole or anastrozole.
9
The results of the BOLERO-2 trial demonstrated that everolimus plus exemestane led to significantly better progression-free survival (PFS) by approximately 4 months. Median PFS for the everolimus plus exemestane group based on local assessment was 6.9 months versus 2.8 months for the exemestane plus placebo group (hazard ratio, 0.43; 95% confidence interval [CI], 0.35–0.54;
The results of the BOLERO-2 study highlighted the potential benefit of the introduction of everolimus and exemestane into the management plan of HR-positive, HER2-negative metastatic breast cancer. A series of subanalyses of the BOLERO-2 study evaluated the everolimus plus exemestane combination in key patient populations. One subgroup analysis determined that everolimus plus exemestane versus placebo plus exemestane improved PFS in patients regardless of the patient's age (<70 years, 8.1 vs 4.0 months; ≥70 years, 6.8 vs 1.5 months). 14 Another subgroup analysis demonstrated the same effects of everolimus and exemestane in Asian and non-Asian subjects, proving that the positive effects of this combination represent an improvement in the management of postmenopausal women with HR-positive, HER2-negative metastatic breast cancer, regardless of ethnicity. 15 The BOLERO-2 trial included a substantial proportion of patients with visceral metastases (56%). 16 Because visceral metastasis is associated with poor prognosis, it is noteworthy that the addition of everolimus to exemestane extended PFS versus exemestane plus placebo regardless of the presence of visceral metastases (with visceral metastases, 6.8 vs 2.8 months; without visceral metastases, 9.9 vs 4.2 months). 16 Improvement in PFS with everolimus plus exemestane versus exemestane plus placebo was also observed in patients who had bone-only lesions at baseline (21%) (12.9 vs 5.3 months). 16 An additional exploratory analysis of the BOLERO-2 study evaluated the effect of everolimus plus exemestane as first-line therapy for advanced disease where the last therapy was an aromatase inhibitor in the neoadjuvant setting (19%). 17 The median PFS for everolimus plus exemestane versus exemestane plus placebo was 11.5 versus 4.1 months, respectively (hazard ratio, 0.39; 95% CI, 0.25–0.62). 17 Another subgroup analysis of the BOLERO-2 trial demonstrated that the everolimus/exemestane combination was associated with a longer time to deterioration in global health-related quality of life surveys versus exemestane plus placebo. 18
TAMRAD trial
Preceding BOLERO-2 was the TAMRAD trial, which investigated the everolimus plus tamoxifen combination versus tamoxifen alone in a randomized, phase II study in patients with HR-positive/HER2-negative metastatic breast cancer with prior exposure to aromatase inhibitors.
19
Patients were randomly assigned to receive everolimus plus tamoxifen (
BRE-43 study
In addition, a single-arm, single-center, phase II analysis evaluated everolimus in combination with fulvestrant in patients with ER-positive metastatic breast cancer whose disease progressed or relapsed on an aromatase inhibitor within 6 months prior to enrollment. 20 Of 31 patients available for analysis, the median time to progression was 7.4 months (95% CI, 1.9–12.1) and median OS was 24 months (95% CI, 18.3–28.7). 20 However, one-third of the patients exhibited de novo resistance to the treatment at the 8-week radiologic disease assessment. 20
Everolimus in other Breast Cancer Subtypes
HER2-positive tumors
Up to 30% of breast cancers overexpress the HER2 receptor,
21
leading to the activation of signaling pathways that stimulate cell proliferation and survival.
22
HER2-targeted therapy has substantially improved outcomes in patients with HER2-positive breast cancer.
22
Similar to therapies targeting HR-positive breast cancer, both de novo and acquired resistance to anti-HER2 therapy can occur. Resistance to trastuzumab, the monoclonal antibody used as an adjuvant therapy for early-stage HER2-positive breast cancer, has been attributed to aberrant activation of the PI3K pathway.
23
This resistance may be related to the loss or dysregulation of phosphatase and tensin homolog (
Compared with combination hormone-targeted therapies and mTOR inhibitors, data supporting combination anti-HER2 treatment and mTOR inhibitors are limited but promising. Results of a phase I trial demonstrated that everolimus had antitumor activity when combined with trastuzumab and paclitaxel in heavily pretreated patients with HER2-overexpressing breast cancer that had progressed during treatment with trastuzumab.
27
In another phase I trial, everolimus showed antitumor activity and provided clinical benefit when combined with trastuzumab and vinorelbine in heavily pretreated patients with HER2-overexpressing breast cancer that had progressed during treatment with trastuzumab; grade 3 or 4 neutropenia was the most common dose-limiting toxicity.
28
In the BOLERO-3 trial, trastuzumab-resistant patients treated with everolimus plus trastuzumab and vinorelbine had a median PFS of 7.0 months versus 5.8 months in patients who received trastuzumab, vinorelbine, and placebo (hazard ratio, 0.78;
Triple-negative tumors
Triple-negative breast cancer, defined by the absence of HER2 and HR expression,
31
is generally at an advanced stage at the time of diagnosis.
32
A phase II trial of everolimus and carboplatin in patients with triple-negative metastatic breast cancer has demonstrated efficacy of this combination treatment, with a clinical benefit rate of 36% and a median PFS of 3 months.
33
Reduction in the dose of carboplatin reduced hematological toxicity in these patients, while preserving the clinical responses.
33
Another recently completed phase II trial in patients with triple-negative breast cancer examined the response of adding everolimus to standard neoadjuvant chemotherapy.
34
Patients were administered paclitaxel ± everolimus weekly for 12 weeks, followed by a combination of 5-fluorouracil, epirubicin, and cyclophosphamide every 3 weeks for four cycles.
34
No significant differences were found between the everolimus-treated and nontreated groups in terms of 12-week response rate (47.8% vs 29.6%;
Future Directions
Ongoing clinical trials of everolimus in HR-positive breast cancer
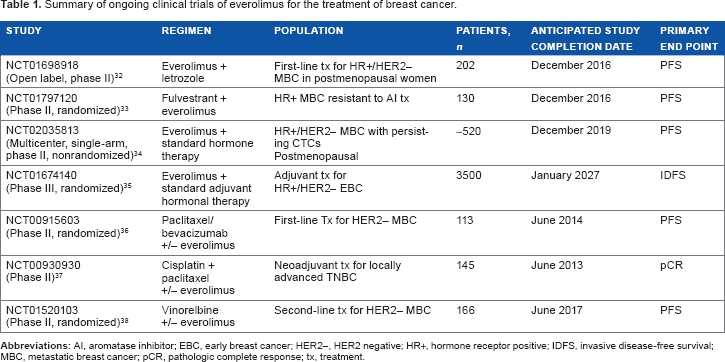
Table 1 summarizes the ongoing clinical trials investigating everolimus in breast cancer.
35
41
These trials are mentioned in this article because they are large studies (
Summary of ongoing clinical trials of everolimus for the treatment of breast cancer.
BOLERO-4 study
BOLERO-4 is an open-label, multicenter, phase II trial of everolimus plus letrozole in the first-line treatment of postmenopausal women with HR-positive, HER2-negative metastatic breast cancer. 35 In addition to investigating the efficacy of the everolimus plus letrozole combination in the initial treatment of this disease, BOLERO-4 aims to determine if this combination is an effective first-line treatment option for metastatic breast cancer and if efficacy can continue after progression using the everolimus plus exemestane combination. 35 BOLERO-4 will also assess whether a nonalcohol steroid mouth rinse can help ameliorate the severity of oral stomatitis, a common side effect of everolimus. 35 The stomatitis part of the study will be conducted only in the United States, where an alcohol-free 0.5 mg/5 mL dexamethasone oral solution is available. 35
Everolimus plus fulvestrant
In another ongoing phase II trial in postmenopausal women with HR-positive, HER2-negative metastatic breast cancer, everolimus in combination with fulvestrant is being investigated after progression on aromatase inhibitor therapy. 36 Patients are randomly assigned 1:1 to fulvestrant with everolimus or placebo and stratified for Eastern Cooperative Oncology Group performance status (0 vs 1), measurable disease versus nonmeasurable disease, and prior chemotherapy for metastatic disease (pretreated vs no prior chemotherapy). 36 Patients will be evaluated for disease response every 12 weeks for a total of 12 cycles. Patients with no evidence of progressive disease who remain on study after completing 12 cycles are unblinded and continue to receive their assigned treatment until disease progression or unacceptable toxicities occur. 36
DETECT IV trial
The DETECT IV trial will further elaborate on our understanding of the effects and mechanism of everolimus in the treatment of HR-positive, HER2-negative metastatic breast cancer. 37 It had been suggested that determining the prevalence and number of circulating tumor cells (CTCs) at various time points during treatment may be an effective tool for assessing treatment efficacy in metastatic breast cancer. 37 DETECT IV is a prospective, multicenter, open-label, single-arm phase II study for postmenopausal patients with HR-positive, HER2-negative metastatic breast cancer and exclusively HER2-negative CTCs. 37 The primary objective of the trial is to estimate the clinical efficacy of everolimus in combination with endocrine therapy as assessed by PFS. Additional research on CTC dynamics and characteristics will provide a better understanding of the prognostic and predictive value of CTCs in this setting. 37
SWOG S1207
Given everolimus's promising results on patient outcomes in the advanced breast cancer setting, using the drug to treat earlier stage disease would be a natural next step in investigating its potential impact in the management of HR-positive, HER2-negative breast cancer. SWOG S1207 is a multicenter, randomized, phase III trial that is investigating the effect of hormone therapy with or without everolimus in patients with early-stage breast cancer. 38 The goals of this study are to compare whether the addition of 1 year of everolimus (10 mg daily) to standard adjuvant endocrine therapy improves invasive disease-free survival in patients with high-risk, HR-positive, HER2-negative, nonmetastatic breast cancer. 38 Additionally, SWOG S1207 will compare whether the addition of 1 year of everolimus to standard adjuvant endocrine therapy improves OS, distant recurrence-free survival, safety, and tolerability in this patient population. 38
Targeting subtypes
The combination of everolimus with other traditional chemotherapies used to target other subtypes of breast cancer is also being investigated. One randomized, double-blind, placebo-controlled trial is evaluating the impact of adding everolimus to the combination of weekly paclitaxel plus bevacizumab in the first-line treatment of women with HER2-negative metastatic breast cancer. 39 Patients will be randomly assigned 1:1 to receive paclitaxel plus bevacizumab with everolimus versus placebo. 39 Patients will be evaluated for response to treatment every 8 weeks until tumor progression or intolerable toxicity occurs. 39 Another study is investigating the combination of cisplatin, paclitaxel, and everolimus as neoadjuvant treatment for locally advanced triple-negative breast cancer; the primary end point of this study is pathologic complete response at the time of surgical management, using the primary tumor as a de novo marker for sensitivity and response to combination therapy. 40 An additional study is investigating the vinorelbine/everolimus combination versus vinorelbine alone as second-line therapy for HER2-negative, locally advanced or metastatic breast cancer where palliative second-line chemotherapy is indicated; the primary end point is PFS. 41
Conclusions
Finding the optimal combination of therapies to manage patients with HR-positive breast cancer and overcoming endocrine resistance continues to be a challenging goal for clinicians and scientists alike. ER biology is inextricably linked to multiple cell-signaling pathways with known cross-talk and regulatory feedback loops between pathways. The PI3K/mTOR/AKT pathway has been identified as a major gateway behind resistant forms of HR-positive, HER2-negative breast cancer. The clinical studies highlighted in this article demonstrate that mTOR inhibition with drugs such as everolimus can target resistant forms of breast cancer and increases sensitivity to endocrine therapies. Ongoing studies with everolimus in earlier stages of the disease in the adjuvant and neoadjuvant settings (where there is greater opportunity for cure) can potentially benefit even larger numbers of patients.
More preclinical studies with human tumor samples and tissue-based pharmacodynamic studies will need to be performed to better understand the complexity of blocking the mTOR pathway and the resultant alterations in other linked pathways. It is of paramount importance that we continue to enroll patients in clinical trials intended to increase our understanding of endocrine-resistant cancer and to expand our approaches to its treatment.
Author Contributions
Both authors were responsible for the manuscript's conception, design, writing, and final approval.
Footnotes
Acknowledgments
Editorial support in the preparation of this manuscript was provided by Matthew Grzywacz, PhD (ApotheCom, Yardley, PA).